
Last Seen Blogs

thetrancemasterblog
John “The Trance-Master™” Cerbone

justformylofibeats
justformylofibeats

valdisrp
Valdis

dodollemak50
Dodol_Lemak

kaiserrreich
currently dropping ☕
Text
Time didn’t change me, community did!!!
As I reflect on the past, my experiences, my growth and my transformation, I am reminded of a quote by John F. Kennedy when he said, “Change is the law of life. And those who look only to the past or present are certain to miss the future”. Had i focused on what I was used to regarding practicals or focused on how uncomfortable the change from the usual to community, I would have certainly missed out on the growth opportunities that were presented to me. As the block began, I felt like a headless chicken, but as time continued, discussions were facilitated, unfamiliar experiences occurred, and my thinking was challenged I grew to realize how much bigger the world of OT is.
One of the many things I have learnt while working on community is that we don’t choose how we are groomed when growing up, but we have the power to change that programming and find our own unique individual voices. That with those voices we can empower other to find their voices thereby propelling each other forward and growing as a community. Privilege acts a form of veil that covers our eyes from seeing the world for what it is, but going into community, listening, and seeing made it clear to me that just because something is not being experienced b me or anyone, I know does not mean it does not exist. I always believe in taking care of our mental health but being in community and seeing the injustices and oppressions that women face everyday magnified the need for me to stand for maternal/women mental health, not only as an OT but also as a young woman from a rural area. I grew up knowing that women are strong and resilient, that no matter what they are always ready and up in arms to take care of the home. I valued that. I loved that we as women were considered “imbokodo”, mostly because I saw it in every female member of my family, and I thought them appearing strong in the eyes of a child meant that they were invincible. As I grow in community, I’ve learnt to look beyond ‘I'm fine’, to look beyond the smile underneath the mask, but to truly listen to the woman in front of me, to see the pain because that allows me to see the struggles of mental health and gives her the opportunity to deal with and address those issues.
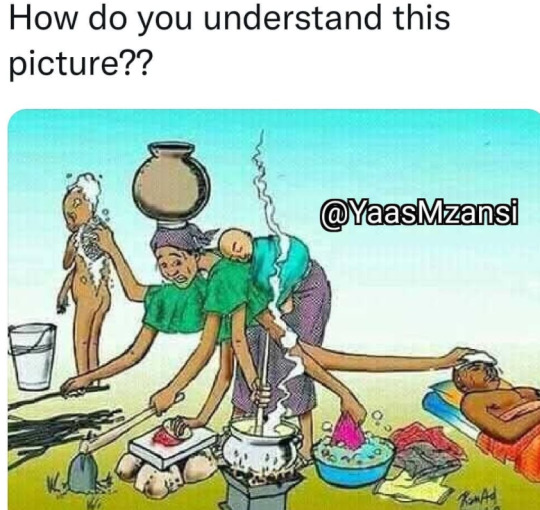
In these few weeks I have come to question the terms resilient and ‘strong woman’, I find them to be encouraging the injustices and inequalities that women all over the country endure. Hurley and Young (2020) defined resilience as the ability to withstand adversity and bounce back from difficult life events. They further allude that some people equate resilience with mental toughness, but demonstrating resilience includes working through emotional pain and suffering. Some have misconstrued the meaning of the word resilience, y making it sound like when you are resilient you are like a tennis ball that hits the floor and instantly jumps higher up. I too am guilty of this mentality, which is why going forward in community and in my daily life I plan to make it known to women that after a fall you don’t have to instantly pick yourself up. Rather it is okay to take time and truly heal so you can be able t bounce back higher than before, that takes mental awareness. The picture below depicts exactly how most women in the communities like Inanda and Mariannridge function daily, which is why most women have felt the need to instantly get up and move after a fall, without fully healing from the trauma they might have suffered.
In the MR community I met a lady who was a neighbor with an 84-year-old woman who lived alone and has issues with her leg, this lady took care of this lady as if she was her own mother without expecting payment or recognition. Her beliefs and values drove her to have the compassion and empathy to look after this old lady. This really touched my heart and had me thinking about what would happen if we as OTs were to care for our client’s as much as that lady cared for that older lady. To not just do our jobs because we get paid but to do it because we recognize the need for our services in these communities. Being in the community in these last few weeks has emphasized in me that, as OTs we need to proudly reclaim compassion as a core value and recognize it as the fuel which transforms empathy into person-centered occupational therapy practice (Thomas & Menage, 2016). In this block I have grown academically and personally, I have found that my compassionate personality has allowed me to better connect with individuals in community. But I have also learned that I have to take care of my mental health as well, so not to mainly focus on taking care of everyone else and neglect myself, to not bite off more than I can chew but to allow myself to be helped and guided.
Going forward, I thrive to not let my personal beliefs and opinions cloud my judgement when treating, but to be compassionate, to e holistic to allow myself to hear the things that are not said. My goal is to be available to women who struggle with mental health and this block has made me realize that there is a great need for that in our communities. In essence I can say there was life before community and there’s life after community,
#occupationaltherapy
#communityOT
References
https://thegoalchaser.com/the-past-is-the-past-quotes/
Hurley, & Young. (2020). What Is Resilience? Definition, Types, Building Resiliency, Benefits, and Resources | Everyday Health. Retrieved 26 August 2021, from https://www.everydayhealth.com/wellness/resilience/
Thomas, Y. et Menage, D.. (2016). Reclaiming compassion as a core value in occupational therapy. British journal of occupational therapy, 79(1), 3‑4. doi:10.1177/0308022615620682
https://www.instagram.com/p/CTCN-eqsnoM/
0 notes
Text
How have I implemented developmental goals in my fieldwork community?
In communities like Inanda and Mariannridge, which of the 17 sustainable developmental goals are implementable in such communities? Are these goals even practical for communities like these?
The beauty of working in a community is that we get exposed to ways of living that might be completely different from what we are used to. This allows us to come with fresh eyes into the community and recognize injustices in these communities, but also fresh eye working alone can do very little. But with our fresh eyes and ideas working together with individuals with lived experiences and who have been part of the community, will start a trajectory of change and development. Issues of unemployment, poverty, gender inequality, and lack of education are some of the issues that are present in these communities. These issues have imbedded themselves in these communities to such an extent that the community members don’t recognize them as issues but rather their normal or reality. Though these injustices have become part of the communities, it’s still our duty to shine the light on them and bring about change, as Ann Plato once said “to remove ignorance is an important branch of benevolence.”

The sustainable developmental goals (SDGs) were developed to be met by the year 2030 where all poverty as we know it would be the thing of the past, and people would be living in peace and prosperity ("Sustainable Development Goals | United Nations Development Programme", 2021). They came about after the Millennium Development Goals (MDGs) failed and diverged since they considered all countries and not just the developing ones. The logic in the SDGs is that each goal depends on another (Nilsson et al., 2016), and for that reason, it has been criticized over the years. There are 17 goals, the five that I will be looking at today are the ones I saw were mostly dependent on each other when it comes to implementing them in the community.
Goal 3: GOOD HEALTH AND WELL-BEING
As defined by WHO (1948), well-being is “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. This goal aims for complete mental, physical, emotional well-being, ensuring that epidemics like HIV/AIDS, TB infection remain low in our society and that all have access to free healthcare. In the Mariannridge community, free health care is available to all (permanent citizens or not) through the one clinic that is present even though it is under-resourced. Now, the question is how possible is it for the Mariannridge community to have complete well-being? As I stated before, these issues are interrelated, meaning we cannot strive for well-being without all the different factors that affect the well-being of the members of the community. The SDG 3 is also concerned about maternal and child health (Guégan et al., 2018), which are impacted by a vast number of factors in the Mariannridge community. Factors like unemployment, gender inequality, teenage pregnancy, poverty, women-headed household, HIV/AIDs, and many more. Well-being is a privilege that most mothers in the Mariannridge community do not have. The system was rigged against women long ago, the cultural beliefs, the prejudiced actions, the patriarchy have all ensured that well-being for some women in the Mariannridge community is but a dream. At the moment in this community, we are ensuring that women know about their physical, mental, and social well-being through health promotion speeches, screening, and the WEP. We are going to train CHWs to screen mothers for mental health issues so that we can empower women as professionals to care for their mental health by taking charge of their lives. Not only are we helping mothers, but we are also equipping community members with knowledge on diseases to promote well-being in the community. With the 3rd wave upon us, our role as OTs to promote well-being Is to ensure that all community members were masks and we sanitize with them regularly, and ensure that we all keep the safety regulations. During home visits or consultations at the clinic or creche/primary school/high school, we need to make sure we all adhere to the protocols.
GOAL 5: GENDER EQUALITY
SDG-5 calls on governments to achieve gender equality and empowerment of all girls, highlighting the importance of sexual and reproductive health (Summerfield & Regan, 2021). To achieve this goal, we do not only need to empower women but also work together with men to break the patriarchy. Gender inequality results from prejudiced beliefs and sometimes cultural beliefs, which is why sometimes what we might see as inequality the person experiencing it might view it as their normal. In the Inanda community, there is a youth group that we sometimes run with the staff members. This group is mostly populated by young females, it is a very informative and educational group that not only equips these young girls with information but also empowers them. What we can do for the communities to achieve this goal is have more youth groups, groups where females will be free and encouraged to speak out against the injustices they have faced, to teach them important life skills like leadership skills. We could implement this Programme at Mariannridge and Inanda by speaking to the CHW’s and developing a plan of action.
GOAL 4: QUALITY EDUCATION
In the Mariannridge and Inada communities, we work with primary and secondary schools as well as creches to ensure that all children get the education they need. Yes, we are not teachers, but we work together with teachers using the knowledge and skills we have to ensure children succeed academically. One of the targets of this goal is to ensure that all youth and a substantial proportion of adults, both men, and women, achieve literacy and numeracy. In these communities, we work with teachers to identify children with learning difficulties and if there are, we work with those children to ensure that they improve those skills they battle with to ensure that they succeed academically. By doing this we are ensuring that by the time these children are adults they would have substantial academic skills resulting in this goal being achieved. In high schools, we are giving information on life skills to ensure that the children are not only educated on academic skills but they are also equipped with the necessary life skills they need to be successful adults. In the Mariannridge community this will ensure to combat the issue of youth unemployment, drug use and high levels of teenage pregnancy and thereby break the cycle of poverty.
GOAL 16: PEACE, JUSTICE AND STRONG INSTITUTIONS
One of the targets is to reduce all forms of violence and related death rates everywhere ("Sustainable Development Goals | United Nations Development Programme", 2021) by promoting justice for all. The GBV protests that have happened and continue to happen are one of the ways that we are reducing violence and promoting justice for women. These projects like the WEP at Mariannridge empower women, which gives them the courage they need to speak out against injustices that they may face. As an OT in the community, I may not be directly reducing violence but the projects and programs we implement in the community work towards helping women realize the power they hold. The maternal health groups that will be run in the coming future will address the injustices that women face in their home, community, and workplace to ensure that women stand up for themselves and that justice is demanded.
GOAL 17: PARTNERSHIP FOR THE GOALS
We will be implemented this goal in the communities by strengthening the establishments we have developed. By creating groups in the community that shares experiences and values like the maternal mental health that will be run, we are establishing support networks and building lasting relationships. For example, Ms. X who was recruited for the WEP at Mariannridge is now part of the project and every UKZN student that works with her develops a relationship with her because of the good work she doe in the project.
The aim is to have a community that relies on one another, a community that aims for good change and growth, a community that laughs together, cries together, and succeeds together.
References
https://www.azquotes.com/quotes/topics/support-systems.html
Nilsson, M., Griggs, D. et Visbeck, M.. (2016). Policy: Map the interactions between Sustainable Development Goals. Nature, 534(7607), 320‑322. doi:10.1038/534320a
Guégan, J., Suzán, G., Kati-Coulibaly, S., Bonpamgue, D., & Moatti, J. (2018). Sustainable Development Goal #3, “health and well-being”, and the need for more integrative thinking. Retrieved 20 August 2021, from http://dx.doi.org/10.21753/vmoa.5.2.443
http://whygreeneconomy.org/the-politics-of-the-sustainable-development-goals-sdgs/
https://www.wisesayings.com/ignorance-quotes/
Sustainable Development Goals | United Nations Development Programme. (2021). Retrieved 20 August 2021, from https://www.undp.org/sustainable-development-goals
Summerfield, Jenny MA (Hons)*; Regan, Lesley DBE, MD, DSc, FRCOG† How Can We Achieve Sustainable Development Goal-5: Gender Equality for All by 2030?, Clinical Obstetrics and Gynecology: September 2021 - Volume 64 - Issue 3 - p 415-421 doi: 10.1097/GRF.0000000000000643
0 notes
Text
What are we without mental health?🤷♀️
From my early teenage years, I have found myself to be the red dot in the mist of white dot, and because I didn’t know better, I always tried to cover my redness. I’m the peculiar person in the group that cares about the things that nobody else cares about, I look deep into the things overlooked. Ever since I got to understand the term ‘mental health’ I have made it a point to advocate for the importance of it any chance I get. I guess you can call me a MENTAL HEALTH ACTIVIST. When it comes to mental health, I mostly relate to a quote by Robert Frost, which say “Two roads diverged in a wood, and I – I took the one less traveled by, and that has made all the difference.”
From infants to the elderly mental health impacts our lives all the same, regardless whether we overlook it or hold it dear to our hearts. I come from a rural community that suffers for the patriarchal gender roles, the community lives by a set of values and beliefs even though it results in a generational cycle of poverty. Men are believed to be the head of the household; women are meant to take care of children and the home. Since it’s a community that is rural it means that the men need to go live to a place closer to work, which actually lives the women as heads of the households every month. Mothers are believed to be these “strong, superwomen” beings, but do we ever stop to wonder whether our mothers are actually this unbreakable “Imbokodo” or they are strong because they feel they have no other choice. Mental health problems in women are prevalent and are determined by circumstances of day-to-day life that are beyond individual control, and by gender-based risks, which may result in disability, reduced quality of life (Fisher et al., 2014). Though this might be the case, mental health of women is still not addressed enough especially in these low socioeconomic areas. Yes! of course, women are strong and powerful, but we really need to stop ad ask our selves this- have we glorified being strong so much that we’ve made struggling with mental health seem like a shameful weakness for women?

The picture above is a clear depiction of the life of some of the women in different communities. Women get consumed so much with taking care of everyone in the home and neglect to take care of themselves, and that is where we depression, anxiety and all mental issues come from. The first year after child birth has a lot of changes for women and that often results in feelings of inadequacy and powerlessness which makes them vulnerable to depression (Rosander et al., 2020). My friend Ms. X, gave birth in the year 2019 to her beautiful baby girl, recently she disclosed that 6 months post giving birth she felt anxious, alone and hopeless. She hid her struggles because she felt it would have appeared ungrateful to her family because they were taking care of her child for her while she was continuing with her studies. She did not feel comfortable with venting to her friends as she figured we would not understand as she did not understand herself. This got me thinking to my thinking process back then, I assumed she was happy because she said she was and she had no stress st the baby was being taken care of. As the saying goes “a child is a blessing”, how many mothers out there are ashamed to be vulnerable enough to say they are struggling mentally even though they have the blessing in their hands? At the communities I am working at I have seen many mothers come to the clinic for their baby’s health, but now when I see them this question arises in me. Which is why I make it a point to speak to them about mental health even if they say they are “fine”.
We ought to advocate for women’s mental health, because in doing so we get to uncover the deeper truths and reasoning for mental health being overlooked in our communities. Although women are living longer, they are not necessarily living better or healthier lives (Douki et al., 2006). It is important to enquire about every patient’s mental health even if they only present with physical conditions, this will ensure that as occupational therapists we are being effective/impactful and holistic. In one of my home visits in the community of Mariannridge I met Ms. K who is a 77-year-old woman who lives with her 72-year-old brother who require 24 hr. care. She also suffers from arthritis, but she still makes sure to care for her brother everyday with assistance from family members sometimes if they visit. In that home visit it was my responsibility to not only assist his brother and advise her on her physical health, but also to advocate for her mental health even though she is an older woman. it is my responsibility to ensure that she prioritizes her health and I saw my positionality play a huge role in my services provision as i was talking with her and giving her ways she should use to care for her mental health. Incorporating my positionality into my practice has opened my eye to the inequality, patriarchal and prejudiced way of living in the communities and how women are possibly bleeding in silence due to the desire to keep up with societal expectations.
Cultural beliefs guide our way of living and they have a range of implications for mental health for in community members. When voicing our “activist points” we should heed the people’s opinion and be conscious of their culture. My beliefs and personality traits are bound to impact the way I deliver my services to the community, I am an emotional person and I tend to put myself in other people’s shoes and I believe that traits enables me to deliver the best treatment. But as a professional I should be able to back down and not enforce beliefs and ideas that people do not want into their lives, our personality traits can affect all aspects of life, including interpersonal relationships and job performance (Masmouei et al,. 202). We can not change how a person thinks unless they want to change, but all we can do to advocate for women mental health is to incorporate it into conversations every chance we get. For example, if we see a teary woman underneath a mask at the clinic, we should always offer a shoulder to cry on and if she is not comfortable be understanding and still make her aware of the possible mental ill-health, she is faced with don’t just leave her there hoping se will eventually feel better. Incorporating women’s mental health in the programmes we run in community will ensure that the subject is not ever overlooked as we will be constant reminders that these are the issues that we need to normalize talking about to smash the stigmas in the communities.
At Mariannridge community we will be implement a p6 week program that is in alignment with my positionality, but it will be more focused on maternal mental health. This program will open up a platform to encourage women to speak about their mental health before and after giving birth. I believe we will make a huge difference in the community with this project because I truly believe that many women suffer from postpartum depression. The Inanda community can also greatly benefit from such a program especially because the rate of teenage pregnancy there is high. Which is why I believe that we should open a forum discussion around the issues of women’s mental health to the Inanda community to uplift the community and communicate change.

We cannot pour from empty cups indeed; this means we ought to take care of ourselves before we even attempt to care for other because by doing that, we would be more effective. We should advocate for women and let them know that taking care of yourself before caring for other is not selfish or irresponsible but it’s necessary. We should promote the widespread understanding that women’s mental health is an essential part of their overall health in our community practices. As OTs working in low socioeconomic communities, we are likely to meet women that suffering from sexual or domestic abuse, poverty, and they are likely to be the main caregivers for their children. So, we should raise awareness on anxiety, depression and other mental health issue to work towards creating change in the interest of preserving women’s mental health ("Oregon counseling", 2021).
References
Douki, S., Ben Zineb, S., Nacef, F. et Halbreich, U.. (2007). Women's mental health in the Muslim world: Cultural, religious, and social issues. Journal of affective disorders, 102(1-3), 177‑189. doi:10.1016/j.jad.2006.09.027
Fisher, J., Nguyen, H., Mannava, P., Tran, H., Dam, T., Tran, H. et Luchters, S.. (2014). Translation, cultural adaptation and field-testing of the Thinking Healthy Program for Vietnam. Globalization and health, 10(1), 37. doi:10.1186/1744-8603-10-37
Masmouei, B., Bazvand, H., Harorani, M., Bazrafshan, M.-R., Karami, Z. et Jokar, M.. (2020). Relationship Between Personality Traits and Nursing Professionalism. Journal of client-centered nursing care, 6(3), 157‑162. doi:10.32598/jccnc.6.3.267.2
Oregon counseling. (2021). Retrieved 12 August 2021, from https://oregoncounseling.com/article/3-ways-to-support-womens-mental-health/
Rosander, M., Berlin, A., Forslund Frykedal, K. et Barimani, M.. (2020). Maternal depression symptoms during the first 21 months after giving birth. Scandinavian journal of public health, 140349482097796. doi:10.1177/1403494820977969
.
0 notes
Text
“Maternal and child mental health”- a big deal!!!
“There will be many times you will feel like you have failed. But in the eyes, heart and mind of your child, you are supermom.” – Stephanie Precourt
It’s shocking to see that even in the 21st century mental health is still overlooked and stigmatized as if it was still the 1800. With the issues facing the country mental health should be really advocated for, issues like unemployment, trauma, HIV infection, GBV, COVID 19 and now this looting and violence are bound to cause emotional unrest. Only a small percentage of people with severe mental health issues are being treated in South Africa, which indicates the neglect in the health system (Nguse & Wassenaar, 2021). In low socio-economic status communities, mental health is especially overlooked due to lack of awareness and lack of education. Which is why in the Inanda and Mariannridge communities we incorporate health promotion talks to improve awareness in the community as Occupational therapists.
“The children are the future” we always here, but we fall short to think beyond the child and look at the person taking care of the child. Maternal mental health is so crucial, yet the topic is not discussed enough for people to actually be aware of it. According to Kimmel (2020) depression and anxiety is common in the perinatal period and it can result in insufficient care to the child or the mother committing suicide. The stress of becoming or being a mother or pressure of being a “good” mother can also result in anxiety or depression, but most mothers do not recognize or disregard the symptoms of post-natal depression due to having the mentality that they need to be strong for their children. At Inanda and Mariannridge, the health talks done at the clinic by the UKZN student OTs addresses these issues to bring awareness to the general community.
These projects are crucial because in these communities since there is a vastly high rate of teenage pregnancy, just to inform them on these conditions since most of them are often first-time mothers, especially because teenage mothers face plenty of challenges, from dealing with the shame and stigma of an unplanned pregnancy to finishing school and finding employment (Reese, 2018). I had an experience at Inanda clinic which I found eye opening. Ms. X had come to the clinic for her checkup as she was pregnant, I spoke to her and informed her about maternal mental health. Upon enquiring about her mental health, she appeared uncomfortable but stated she was fine, this indicated to me that mental health has been so stigmatized that we get uncomfortable even talking about it with strangers or people we know. Women with perinatal mental illness often don’t get treatment even if it is available, because women choose not to disclose and seek help (Moore et al., 2016). Postpartum depression interferes with a mother’s ability to bond with her infant and negatively impacts the infant’s development and behavior (Murray, 1996; George, 2011). In the communities we are working in we could run groups with mother that are about to give birth and groups with mothers that have given birth to ensure that the have a space/community where they are free to talk about their mental health/share experience/get educated on maternal mental health to ensure that they are the best mothers they can be for their children.

As occupational therapists we are also interested in child mental health, which is also overlooked in our communities due to lack of awareness and education. Conditions like ADHD, ODD, CD often go unnoticed in children in low socioeconomic status communities because the child is labeled as hyper or defiant. After speaking to one of the employees at the Inanda Clinic about the youth support groups that we will run with them, and how the children in the community are struggling with mental/psychosocial issues secondary to HIV, teenage pregnancy and many more, it is clear that socioeconomic inequality is another factor that increases mental health problems in childhood and adolescence (Reiss, 2013).
Even though I have not had the opportunity to screen or treat any pediatric clients with mental health issues or developmental delays in the communities I and currently working. I am aware that in these communities there are children in creches and primary schools that do have developmental delays or learning difficulties and they could benefit greatly from occupational therapy intervention. As occupational therapists in these communities our role is to identify these children with difficulties and assist them to promote safe and healthy environments for learning, growth, and development by addressing mental health aiming to promote successful participation in the occupations using a client-centered evaluation process (Mahaffey, 2016).
As occupational therapists at Inanda and Mariannridge we work with children in creches/preschools, primary and secondary school. We ensure that before working with the child, we get consent from the mother and gather information from the mother and the teachers since they spend most of the time with the child to gain better understanding of their behavior. This also allows parents to e informed of their child’s improvements and changes and what they can do as parents to foster that when they are at home. It is crucial that we work with the parents for the child and the teacher when working with the child to ensure that their way of handling the child does not foster the negative behavior we are trying to combat, which is why caregiver education is so such an integral part of occupational therapy community practice.
Intervention is provided through both group and individual therapy, through purposeful, and occupation-based interventions aimed at enhancing emotional well-being, social competence, and the skills required to resume participation in essential daily roles including academic, self-care, home, or community-based (Schwarzschild, 2017). At Inanda we also do storytelling projects, fairy tree, tractor building, and sandpit to encourage imaginative thinking from children and improve self-esteem and engaging in play since children learn best through play. According to Lashbrook (2018) play for children can promote joy and excitement, which can improve their mood and decrease anxiety and sadness, whereas insufficient playtime increases symptoms of depression, anxiety, inattention, and conduct problems in children.
How many mothers out there in the Inanda and Mariannridge community are uncomfortable speaking about maternal health dur to the negativity around it? In the short time that I have been in these communities I have seen a vast number of mothers and mother-to-be, and this has motivated me more to advocate for child and maternal mental health in these communities. One thing I have learned is that as OTs if we focus on the child alone, we are creating an imbalance which could have dire effects in the long run. But we must remember that advocating for mental health is not just feeding people information but rather listening to the communities’ views and concerns and providing the necessary support ("What is advocacy?", 2018).
#mentalhealth
#perinatal depression
#childmentalhealth
References
George, M. (2011). Proposed Role for Occupational Therapy to Serve New Mothers. Retrieved 5 August 2021, from https://core.ac.uk/download/pdf/48846559.pdf
Kimmel, M.. (2020). Maternal Mental Health MATTERS. North carolina medical journal, 81(1), 45‑50. doi:10.18043/ncm.81.1.45
Lashbrook, A. (2018). Playtime May Bolster Kids' Mental Health. Retrieved 5 August 2021, from https://www.theatlantic.com/health/archive/2018/08/playtime-may-boost-kids-mental-health/568186/
Mahaffey, L. (2016). Occupational Therapy’s Role with Mental Health in Children and Youth. Retrieved 05 August 2021, from https://www.aota.org/About-Occupational-Therapy/Professionals/MH/children-youth-mental health.aspx#:~:text=Occupational%20therapy%20practitioners%20can%20assist,with%20economic%20or%20social%20disadvantages.
Moore, D., Ayers, S., & Drey, N. (2016). A Thematic Analysis of Stigma and Disclosure for Perinatal Depression on an Online Forum. JMIR Mental Health, 3(2), e18. doi: 10.2196/mental.5611
Nguse, S. et Wassenaar, D.. (2021). Mental health and COVID-19 in South Africa. South african journal of psychology, 51(2), 304‑313. doi:10.1177/00812463211001543
Reese, D. (2018). The Mental Health of Teen Moms Matters — Seleni - Maternal Mental Health Institute. Retrieved 5 August 2021, from https://www.seleni.org/advice-support/2018/3/14/the-mental-health-of-teen-moms-matters
Reiss, F.. (2013). Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Social science & medicine, 90, 24‑31. doi:10.1016/j.socscimed.2013.04.026
Schwarzschild, J. (2017). The Role of OT in Pediatric Mental Health. Retrieved 05 August 2021, from https://aaspeech.com/role-ot-pediatric-mental-health/
What is advocacy?. (2018). Retrieved 5 August 2021, from https://www.mind.org.uk/information-support/guides-to-support-and-services/advocacy/what-is-advocacy/
0 notes
Text
Advice for my future self as a person and as an OT
If this year or this pandemic has been full of something(s) it’s lessons, lessons we learned the hard way, lessons we learned through listening and lessons we learned through watching others go through stuff. This year mostly taught us to not only think of ourselves and own safety but to think of others too.
My advice to my future self would be to be considerate and compassionate to others because we do not know what is happening in people’s live ad just because it’s not happening to me, it does not mean it is not happening to the next person. This pandemic did not only take a lot of people’s lives, but it also highlighted and increased the level of crime, gender-based violence and child abuse. A lot of women and children here in South Africa were in hell during the lockdown because of the abuse they suffered in their homes, a lot of women lost their lives and even now women and children are still being violated and are trapped in loveless homes. We who have the power and the voices to speak out about such things we must do that because you do not know whose life you are saving with just a twit or post. Widad Akrawi said “We are determined to answer evil with GOOD, slavery with FREEDOM, rape with hope”, so it is my hope that we do just that.

To the future OT that I will become, I would say Don't be afraid to try something new, the thoughts outside of the box are actually better than the ones inside the box. It can be a scary world out there and breaking out of my comfort zone into a new environment can be tough. It’s a lot of work to get ready to jump into a way of doing things. But it can be very worthwhile, and you shouldn't let fear hold you back as long as you're willing to do the work and think that it will align well with your interests and passions. This year has put a lot of strain on people’s mental health, so as OTs we also have a role to play in helping people deal with things like depression, anxiety etc. mental health is very important and as OTs we are supposed to put the FUN back in FUNCTIONAL, so let us do just that because the people need us. This block has been one of the highlights of this year and the growth that it came with it, getting to learn without the pressure of passing or failing and having support from the other group members made all the difference and I would advise my future self to keep forming friendships everywhere I go and maintain the ones already form to get the best experience as an OT.

This year I learnt that sometimes it’s good to be alone and to detach from the world because that is when real growth happens. We learnt that we had strengths that we wouldn’t have discovered had it not been for the virus, we found ourselves to be stronger than we actually thought we were, and that is what will make us the GREATEST OTs in the future because we were thrown in the deep end and we survived. And with a great group members or friends by my side was the greatest experience that I will cherish forever and knowing that the bonds that we formed can never be easily broken gives me more hope for the future.
https://www.freepik.com/premium-vector/happy-women-girls-standing-together-holding-hands-group-female-friends-union-feminists-sisterhood-flat-cartoon-characters-isolated-colorful-illustration_6594345.htm
https://www.dreamstime.com/illustration/helping-hands.html
Website: Powa
Phone number: 011 642 434/6
Social media: Facebook and Twitter
Website: Stop Gender Abuse
Toll-free helpline: 0800 150 150
Social media: Facebook and Twitter
0 notes
Text
In a nutshell- coming out of your shell and beyond
The world has changed and the fact that it’s not like how it used to be or how we expected it to be does not mean that we have to stop living or live in fear because that’s not really living, “Fear defeats more people than any other one thing in the world.” Emerson (2018). Online learning had some negatives and positives but initially I was more focused on the negatives because it was out of my comfort zone, but now that I’ve been at it for so long the negatives don’t even matter anymore because I get the work done.
Doing practicals online was a bit of a challenge initially because it was something new and there was fear of not doing great in the tasks. This new normal brought to my attention that I had poor time management, poor planning and another thing that online learning exposed about me that I did not like about myself was that I do a lot of procrastinating that is why I get stressed so much. What’s interesting is I got to learn and understand more about these unlikeable characteristics through OT4 and OT3 telehealth groups. I must admit that being asked to be part of a group run by other students was a bit uncomfortable for me, but I joined because I wanted to get the experience and learn more from my peers and from the OT4s. I honestly learnt a lot from these groups about stress management, understanding emotions and time management. So, I can say that these experiences were part of the good thigs that happened due to COVID-19.
Getting to work with simulated cases and having a client that was referred by the ADO to us was very eye opening and a great experience. Since I had not been on psych block since last year first semester, my assessment and observation skills were a bit rusty. I got to remind myself of assessments without the rush and pressure that is I usually have when I am actually onsite. Treating my colleagues and referred a client assessment findings really required me to have good observation skills and really consider what would be best beneficial to them and think back to the first day of this block and looking at me now I see and understand how I have improved and how I still need to improve and how to implement what I have learnt on this block on site. One of the most important things I got to experience more of on the previous block is that as OTs we are responsible for peoples well-being and how successful they are in their lives, and that made me fall more in love with being an OT.
One of my lecturers told us that one day we will look back and tell a story of how we adapted to learning and thriving during a pandemic. And I truly believe that we will succeed through online learning even though it’s not what is normal because the harder the struggle, the more glorious the triumph. I feel I have gotten better in my assessment and treatment skills in this block and my rapport skills have improved, and that gives me hope that I will make a great OT someday.
Covid-19 Counselling: 0800 786 786 (Monday – Friday 9am – 4pm)
For Medical or Psychiatric Emergencies contact ER24 084 124
https://www.youtube.com/watch?v=5QbtU8daKc8
https://quoteinvestigator.com/2018/10/30/fear-not/
0 notes
Text
COVID- Trick or Treat?
When I think of this year all that has been going on in it I think of a quote by Victor Frankl which says, “When we are no longer able to change a situation, we are challenged to change ourselves.” It is an undeniable fact that Covid-19 shook and turned every bodies lives upside down, but the choice was left to us to either adapt and survive or allow the year to swallow us whole.
No one thought they would ever live in a time where there is a disease that has the power to stop the normal functioning of the world and has brought so much pain, fear and disruption. But I guess that’s the thing about change, it comes unexpectedly and whether you want to or not you have to adapt. Staying at home for close to four months, not seeing most of my friends, not attending lectures, not going to practicals was a big change that took me a little while to adjust to. I had to change my learning schedules to fit with the new normal and doing that was hard because studying at res or in class is very different to studying at home. At home they don’t really understand the pressure you are in as a student, and even me as a student my priorities got a bit messed up for some time there because my life was changed. I had never done online learning before, so I had to learn how to use ZOOM and rely rely and improve communication with the lecturers and the other students. The fact that this was the new normal was encouragement enough for me to learn to adapt and be calm in the storm to preserve my sanity and mental health.

I’m an introvert so I must say that since I have gotten used to and adapted to this new life I find that it is not all that bad. When online learning first stared it was like everything was piling up together and didn’t know where to start sorting things out. Starting second semester online was not as bad as I had expected it to be, because I was back at res and I was now familiar with working online. That’s when I learned that expecting the worst out of situations is not the best option that is out there. It’s like Jan Dargatz says, “A positive statement propels hope toward a better future, it builds up your faith and that of others, and it promotes change.”, hope is what we are living on now, hope that they find a vaccine, hope that our loved ones or us don’t get infected and hope that we make the most of our time and focus on our studies even though we are in a pandemic.
2020 has most definitely been a tricky year. We have learnt a lot and a lot happened that I did not think would happen, there was a lot of personal growth and much needed adapting. COVID-19 is trick that everyone wishes was over or had never even started, but since it’s here and is not going anywhere we are trying our bet to control it and not let it control us.
For Afterhours Mental Health support contact · Lifeline 0861 322 322 · SADAG 0800 567 567 · 24 hour helpline 080 456 789 · Medical Students Discovery Helpline 0800 323 323 Covid-19 Counselling 0800 786 786 Monday – Friday 9am – 4pm For Medical or Psychiatric Emergencies contact ER24 084 124.
0 notes


Text
Multidisciplinary team and teamwork
According to Mitchell et al. (2008) “A multidisciplinary team involves a range of health professionals, from one or more organisations, working together to deliver comprehensive patient care. The ideal multidisciplinary team for the delivery of care includes: general practitioners; practice nurses; community health nurses; allied health professionals such as physiotherapists, occupational therapists, dieticians, psychologists, social workers, podiatrists and Aboriginal Health Workers; health educators.” The team must share goals, information technology and decision making, but most importantly it must provide patient cantered care.
This week I learned that when working as a multidisciplinary team it is important to understand the roles that each health professional plays in helping to get the patient better. I also learned that it is important to under stand your role as an occupational therapist in the patient’s life, but because physiotherapy and occupational therapy can be similar in some way or share roles it is easy to use an intervention method or approach that would have been used by a physiotherapist. The key is to correct that mistake and ensure it does not happen again to keep the peace in the department and have functional and meaningful sessions with the patient. According to Catherine “The fields of occupational therapy and physical therapy are often confused. While both roles provide essential hands-on rehabilitative work to help clients perform everyday tasks as independently as possible, each field takes a diverse approach in helping people get back to their usual way of life. The main difference between occupational therapy and physical therapy is that OT focuses on improving a client’s ability to perform activities of daily living (ADL) and PT focuses on improving a client’s ability to perform movement of the human body.”
So, this week was the last week of physical block of fieldwork and I realised the importance of writing the soap notes, how important it is to do thorough assessments and report on correct findings, because those findings will guide your treatment and treatment planning. I realised that the soap notes are inspiring teamwork because you get to see progress of the patient from different professional’s’ points of view. According to azcenreal.com “Improved productivity results when multidisciplinary teams function efficiently. It’s important that team members commit themselves to listen carefully, respect the opinions of others, and value other team members' skills and strengths…Team members need to remember to withhold initial criticism, welcome unusual ideas, and consider how to combine and improve ideas. Removing personal bias and entertaining new ideas can solve problems.” In this block I got to observe other occupational therapist and physiotherapists treating and working together for the benefit of the patient, this helped me understand that the patient’s recovery is dependent on every member of the MDT’s contribution in treatment.
Overall, this block has been very insightful and the feedback from the supervisor and the therapists in the venue will be helpful going forward. Even though there are areas I still need to improve on I learnt a lot and I’m very grateful to have had the opportunity to such experienced individuals during this difficult phase of our lives.
https://yourbusiness.azcentral.com/multidisciplinary-teams-importance-teamwork-21959.html
https://otaonline.stkate.edu/blog/fields-occupational-therapy-and-physical-therapy-whats-difference/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6201820/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6201820/
0 notes
Text
Clinical reasoning cycle and cultural humility
Levett-Jones et al (2009) describes clinical reasoning as a process by which medical professionals collect cues, process the information, come to an understanding of a patient problem or situation, plan and implement interventions, evaluate outcomes, and reflect on, and learn from the process. The authors describe the five rights of effective clinical reasoning. These are cues, action, patient, time and reason. According to Watwer and Asbill (2013) “cultural humility is a humble and respectful attitude toward individuals of other cultures that pushes one to challenge their own cultural biases, realize they cannot possibly know everything about other cultures, and approach learning about other cultures as a lifelong goal and process.”
Having had lectures/sessions on clinical reasons the week before practicals started made me understand clinical reasoning and we are supposed to apply it as a skill we need as Occupational therapy students. When I had assessed my client, I tried to get as much information as I can so that those assessment findings could help me come up with therapeutic treatment session. Clinical reasoning is basically explaining why you are using that particular method or activity to treat your client or client factors. So that is why having accurate and correct assessment finding is important to generate proper and strong clinical reasoning. I have put the clinical reasoning cycle into practice during my treatment session write ups, because I had to look at my assessment finding and see which principles could I implement during the session to improve/treat that client factor then I had to reason why I felt that principle was going to be the correct one to implement. Clinical reasoning also helped me explain to my client why they needed to do the session, making them understand how it was going to be beneficial for them and help them get better.
During the session I implemented cultural humility because it is important to respect and get oriented to another person’s culture. During the interview I made sure to ask the client what their culture is or how they identify based on cultures. This was done so that that sessions I plan, and my clinical reasoning does not offend the client, because even if you are the same race as another person you can still fall under different cultures.
The feedback about choosing activities for my session from the supervisor brought a new way of thinking about treatment sessions for my clients. Prior to receiving the feedback, I used to plan treatment sessions based on the thing I felt that the client should be doing and not considering the clients goals for treatment or therapy. Now that I have been advised to ask the clients what THEIR goals for treatment are, I feel it will make my sessions go smoother and they will participate more willingly because it is something they want to do and something they was to improve or see change in. my activities will now be more client-centred functional goals. As Randall and McEwen (2000) said “Perhaps the most important reason for having patient-centred functional goals is that people are likely to make the greatest gains when therapy and the related goals focus on activities that are meaningful to them and that will make a difference in their lives”
According to Aiken et al (2003) effective clinical reasoning skills have a positive impact on patient outcomes. Conversely, those with poor clinical reasoning skills often fail to detect impending patient deterioration resulting in a “failure-to-rescue”. So the question is my clinical reasoning appropriate and is it benefiting my clients during treatment?
https://www.utas.edu.au/__data/assets/pdf_file/0003/263487/Clinical-Reasoning-Instructor-Resources.pdf
https://blogs.utas.edu.au/snm-pep/2012/05/28/clinical-reasoning-cycle
https://www.apa.org/pi/families/resources/newsletter/2013/08/cultural-humility
https://academic.oup.com/ptj/article/80/12/1197/2842443
0 notes
Text
Communication
Clear and good communication between a therapist and a client as well as between a therapist and other medical professionals is very important to build rapport and to provide appropriate treatment for the client and have positive health outcomes. Communication can be described as the exchange of information between two or more people and that can be verbal or non-verbal. Price (2017) states that an occupational therapist must utilise good communication skills to build a healthy relationship with their client.
During a one session with my client I learnt that verbally communicating with the client can enhance the level of the session being therapeutic for the client, for example telling the client to move their affected arm out if the way when mobilizing them rather then just moving it myself can improve the client’s awareness of their affected side. Talking to the client and getting to know them also helps you to plan a session that is relevant to them and increases their interest in the activity and they engage more. I used English to communicate with the client since it’s her first language which made her feel at ease to talk to me and voice out her opinions about the session. (https://www.youtube.com/watch?v=dFnJ9RyY8q0) HEE talks about continuously explaining the actions to the client which makes them aware that they are involved in the session, I ensured this by continuously reminding the client that she tells me when the pain was beginning to be too much so we could stop.
“Members of an inter professional team share a common set of goals and a mutual understanding of purpose; thus, effective communication between health professional is essential for them to successfully achieve their goal” said Shoham, Harris, Mundt, and McGaghie, (2016). This week I needed to communicate with my supervisor, the occupational therapist in the hospital and the physiotherapist about making a splint for my client. This improved my understanding of how decisions are made by in the hospital by an interprofessional team about a client, and how that benefits the client and it’s advantages.
(https://www.ipsf.org/article/importance-interprofessional-teamwork)\
Verbal communication is not the only way to communicate with the client, I use nonverbal communication a lot when I’m with my client. I use demonstrations or gestures to make her understand the instructions and I always make sure that my facial expressions are showing empathy. I use empathy communication with my client and Lasley (2017) states that empathy communication is important to give quality care to the patient. The take home message for this week for me is that I must always communicate with the client and learn to read nonverbal communication from them to make sure that therapy is effective and that I don’t their opinions, requests and pain limitations.
https://communicationinoccupationaltherapy327.wordpress.com/
([email protected] OR 086 574 8073) contact information of a clinical psychologist since she has depression.
0 notes
Text
Client centred therapists
The second week of practicals was interesting and fun. This week was physically and psychologically challenging for me because I had to et to know a new client and all the activities I did with my other client were client were done in sitting meaning I had to do transfers which was a bit more difficult than I thought. Client-centered therapists aim to understand how the world looks from the point of view of their clients and this Is what I tried to do this week with my client’s.
This week I had to do a two person transfers using a transfer board twice, this made me realize that I still needed to work on my transferring skills as the posture I was in while transferring the client was not favoring my back. In the activities I did with my other client he was standing but his balance was not safe/good and so the supervisor gave me feedback/advice on how to ensure safety for the client by holding on his belt and putting my hand in front of him. I applied this on him today and I felt I was providing more safety for the client and that I felt more in control. Today I did a session with my CVA client that has poor sitting balance and the session was therapeutic I that it allowed her to sit and strengthen trunk muscles, but the chosen activity was to difficult for the client to understand so I had to change and do another activity. Basically, the session did not go as well as I wanted, this taught me to think hard and well about the activities I do with my client and consider all the aspects of it including the client’s level of cognitive abilities. I also got to do a home programme exercise for the first time, I put together activities for the client to do at home that would help him be able to get better and go back to work i had to get ti know him and his home environment so that i knew which recommendations to make and which exercise were better suited for him, and got feedback about the mistakes I made which was helpful because now I feel like I can do a home programme.
This week was insight on what I needed to work on with my client’s and also on myself to benefit my clients more. My client also informed me that I was good at what I do since I was respecting her pain threshold and she told me that she enjoys our session, getting positive reaction from her made me understand that what we do as Occupational therapists really does matter.
https://www.health.harvard.edu/newsletter_article/Client-centered_therapy
https://www.youtube.com/watch?v=o0neRQzudzw
1 note
·
View note
Text
From theory into practice
this week on Monday was first day of practicals i got two client one with CVA and another with GBS. i was nervous on the first day because it had been such a long time since i last assessed a patient. I made a mistake of not reading up on the different conditions and when i got a client with GBS i just didn’t know where to start, likely our supervisor is really nice so she helped by telling me about the condition and during Assessment she assisted me and gave me feed back which helped me to prepare for the second session.
As today was the second day of practicals, i got to do a session of bed mobility with my CVA client and it was a success i was very happy with how i handled the client and it also helped that there was an OT during the session to assist me. i also got to do two-person-transfer for the first time which was a bit difficult but i managed to do it without injuring the client. I couldn’t see my GBS client today unfortunately but i did get to treat another client, that session was not properly planned so it was very short and more physio based than OT based. overall toady was good day and i enjoyed treating the patients, the feedback from the supervisor will help me to plan for my following sessions.
2 notes
·
View notes