
xafterlifex
.Life.
Hi anons!
Just thought I'd actually type something in this here box because I've had this blog for a while and haven't added a...about me? idek what you'd call it. more like read this because you're on my page xS So, on a serious note:
I know that some of my followers are going through some rough shit in life and are struggling to keep -anything at all- together. I've been there I'm still getting through problems of my own. But if you're suffering in silence, talk to someone. In a perfect world kids should be able to talk to their parents or guardian about anything that bothers them. I understand that you cannot always talk to your parent or guardian, but at least tell someone. Whether that person be a friend, teacher, counselor, etc. I'm also always open to listening and helping people get through their shit because I've been in really tough places. Take some deep breaths, relax yourself and think about those people who you know would be affected if you disappeared...whether that person is a friend, relative, even a kid who's in your math class who talks to you once in a while. I know this probably sounds stupid, but someone cares about you. Even if that person hasn't made it clear that they care. I don't want to go into a whole discussion on things you can do to make yourself feel better (that are positive!) But send me a question and I don't care if you're an anon or not.
If you decided not to read anything that I wrote above, at least read this:
Suicide is not the answer. It does not eliminate the chances of life getting worse. It destroys the hope of a better life.
17809 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs




Text
When I first start a pharmacology test

When I get to page two

Select all that apply
Classmate asks how I think I did after the test

90 notes
·
View notes

Photo
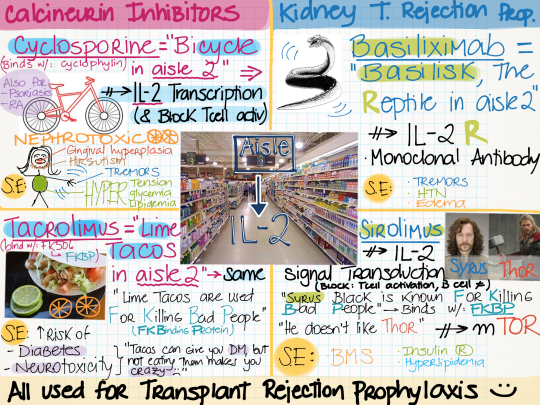
Immunosupressants Drug Mnemonic
Bc everything’s better when I study with Harry Potter references.
I’m reposting it, because I love this chart
201 notes
·
View notes
Photo
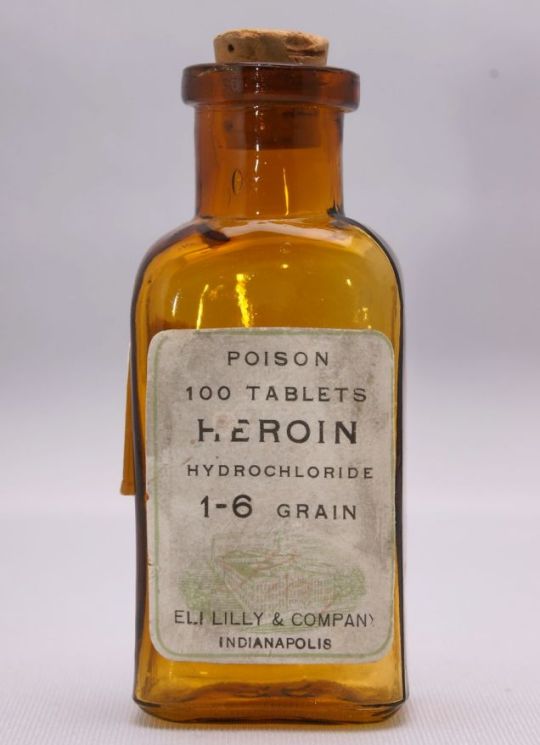
While working on my opiate lecture, I stumbled upon this picture of a vintage heroin bottle from Eli Lilly. Awesome.
1K notes
·
View notes
Photo
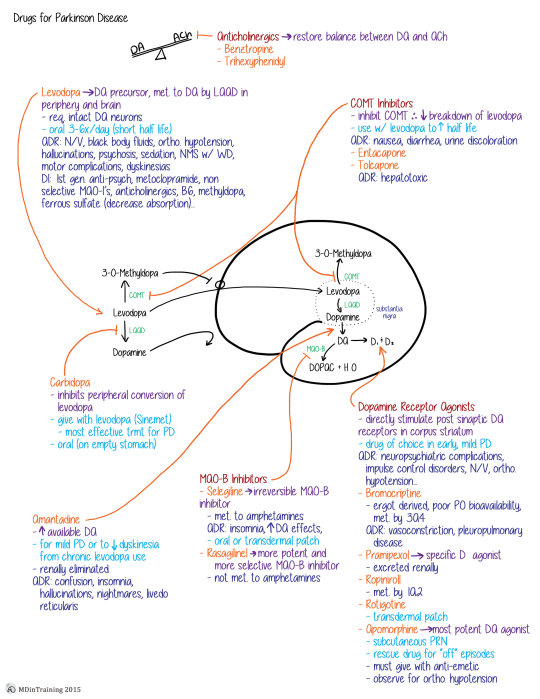
Drugs for Parkinson’s Disease Concept Map
ADR = Adverse drug reactions
DI = drug interactions
Red = class of drugs, orange = drug name, purple = mechanism of action, light blue = dosing and use, dark blue = ADRs/DIs/notes, green = enzyme
205 notes
·
View notes
Photo
Antibiotic mechanisms and microbial resistance…examples of darwin’s evolution at its finest and most terrifying
134 notes
·
View notes
Photo
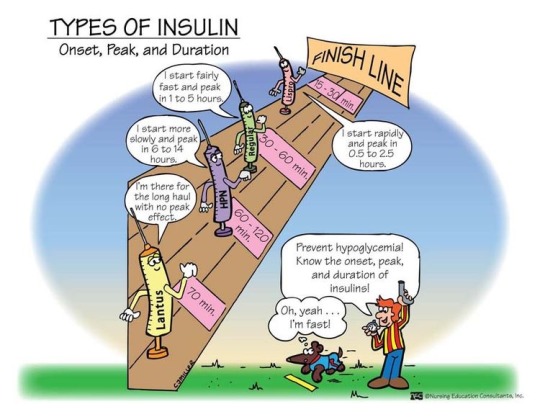
Very important and commonly asked information on INSULIN that you are usually expected to answer at any med exam.
487 notes
·
View notes

Text
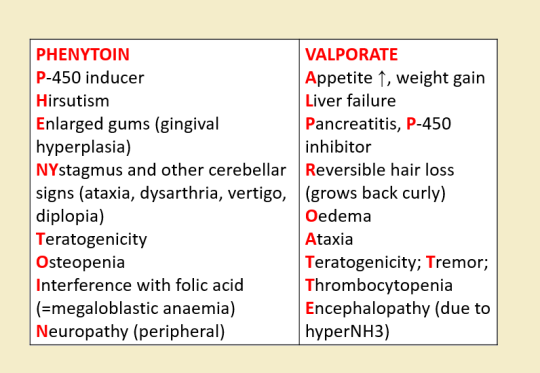
Anti-epileptics/Anti-convulsants Made Incredibly Easy
TREATMENT STRATEGIES:
Start therapy after the second seizure; first ONLY if recurrence is high = MRI abnormal, EEG abnormal, or status epilepticus.
Monotherapy until seizures are controlled.
If failed: titrate up to maximum tolerated dose –> shift to alternative drug –> use drug combination –> VNS, DBS.
Full drug therapy for 2 – 3 years after the last fit.
Gradual withdrawal over at least 6 months.
Rx Profile:
(Drawings are courtesy of @mynotes4usmle)
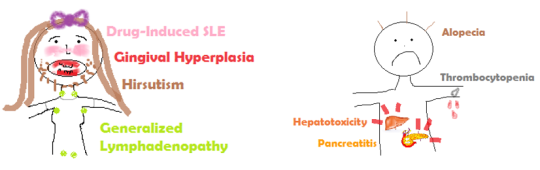
Carbamazepine
Mainly for generalized tonic-clonic seizures
Trigeminal neuralgia
Bipolar disorders (with depressive predomince) - mood stabelizier
NEVER in abscence seizures
SE:
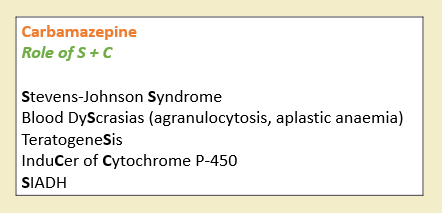
Lamotrigine
Safer profile, with minimal interactions.
Bipolar disorders (with depressive predominance) - mood stabilizer
SE: maculopapular rash; SJS
Topiramate
Broad spectrum anti-seizure; used in migraine.
SE of TopIRamate: enzyme Inhibitor + Renal stones.
TREATMENT PROTOCOL:
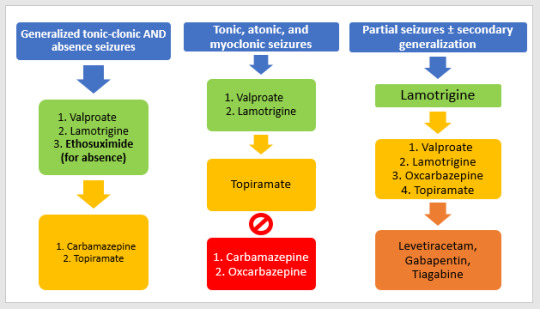
Green: first line; Yellow: second line; Orange: third line; Red: contraindications. (Graph reproduced from Oxford Handbook of Clinical Medicine)
Epilepsy & Pregnancy:
Non-enzyme-inducing AEDS have no effect on the pill. Enzyme inhibitors prolong the half life of OCP (=Valproate) so better for birth control , and vice versa.
Most of AEDs are teratogenic; Category D
Therapy not stopped; uncontrolled seizure is risky to fetus & mother. Give lowest effective dose.
Avoid phenytoin, valproate and barbiturates (use Lamotrigine)
Most AEDs cause folate deficiency …. Folic acid (prior to or early in conception)
Most AEDs are competitive inhibitors of vit. K-dependent clotting factor: Vit. K to mother 10 days before labor & to newborn.
Most except carbamazepine and valproate are present in breast milk. Lamotrigine is safe on infants.
Status Epilepticus:
WHAT? Seizures lasting for >30min, OR repeated seizures without intervening consciousness.
Things to be done:
Bedside glucose, the following tests can be done once Rx has started: lab glucose, ABG, U&E, Ca2+, FBC, ECG.
Consider anticonvulsant levels, toxicology screen, LP, cultures, EEG, CT, CO level.
Pulse oximetry, cardiac monitor.
How to treat?

THE END
1K notes
·
View notes
Photo
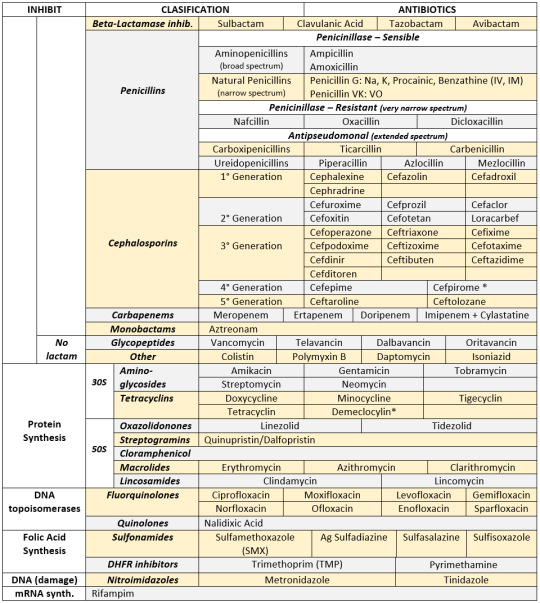
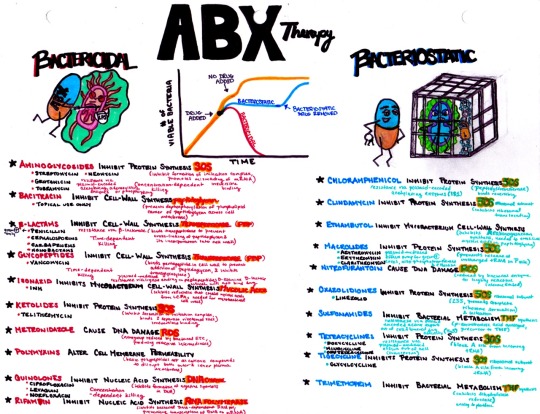
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci
* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines
* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones
10K notes
·
View notes
Quote
If you liked 50 Shades of Grey we have 256 of those in Radiology
MD, Radiologist (via coffeemuggermd)
1K notes
·
View notes