
taku-yamada
Taku Yamada
A general practitioner (Een huisarts) in Japan, 家庭医療専門医
6 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

chumwellness
Chum Wellness

electrifying-elessa
Pkmn Prof. & Ranger🦃🥧

ainsleighgray
Ainsleigh

lalupabianca
LaLupaBianca

feelingkoii
FeelingKoi
Text
Lekker met Nederland! vol.6
(元Dr.コトーの蘭学手記: Blog about life in the Netherlands by a Japanese doctor)
皆さん、2023年になりましたね!
新年初のブログは昨年の第一弾の続きとなるオランダの「ポジティヴヘルス」第二弾の応用編です。今回は前回のポジティヴヘルスの知識をベースに、具体的にどのようにPositive Healthが使用されているのか、オランダの診療所を例にご紹介したいと思います。
Hello everyone! The year 2023 started and time flies so fast.
Thank you for waiting for my update.
In this blog, the first one of this year, I would like to tell you about application of ‘Positive Health’.
Based on the knowledge from my previous blog, which is about ‘Introduction of Positive Health’, I will elaborate how Positive Health is used in practical situations, through the examples of Dutch clinic.
【診療の場におけるポジティヴヘルス】
Part. 1 クモの巣図を作成しよう Let’s make a spider web diagram!
Positive Healthが最初に使用されるようになったのはクリニックなどで患者と医療者が健康について話し合う場面でした。
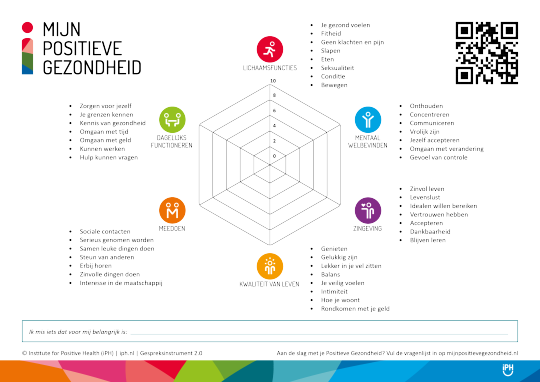
ポジティヴヘルスのクモの巣図をもう一度おさらいすると、①「身体的機能」、②「メンタルウェルビーイング」、③「生きがい」、④「生活の質」、⑤「社会参加」、⑥「日常機能」の6領域があります。
それぞれの領域につき、7問の細かい問いがあり(計42問)、それぞれの質問に対して、0から10点の評価をつけてもらいます(0:全く当てはまらない〜10:完全に当てはなる)。
更に最新版のクモの巣図2.0バージョン(図1:オランダ語)では「身体的機能」にセクシュアリティに関する質問、更に「生活の質」に親密性に関する質問を加えた合計全44項目から構成された質問紙を使用します。
また、どの世代にもわかりやすいようにクモの巣図には「成人用」、「思春期(16-25歳)用」、「小児(8-16歳)用」など年齢別に質問も対応しています。
Positive Health (PH) was originally introduced in clinical practice, where patients and health care providers discussed health.
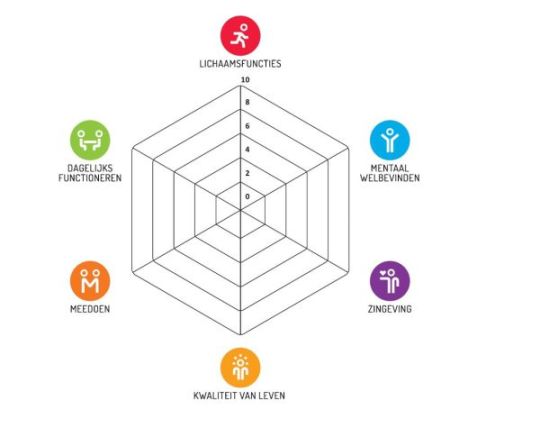
Reviewing the spider web diagram of PH again, there are six domains: (1) "bodily functions", (2) "mental well-being", (3) "meaningfulness", (4) "quality of life", (5) "participation", and (6) "daily functioning".
For each domain, there are 7 detailed questions (42 questions in total), and the participants are asked to rate each question on a scale of 0 to 10 (0: not applicable at all to 10: completely applicable).
In addition, the latest version of the Spider's Web Diagram 2.0 (Figure 1: in Dutch) uses a questionnaire with a total of 44 items, including questions on sexuality in "bodily functions" and questions on intimacy in "quality of life" .
The spider web diagram also differs according to different age groups, such as "adult," "adolescent (16-25 years)," or "child (8-16 years), with different detailed questions in order to make it easier to understand the concept of PH for all generations.
引用(Reference): Institute for Positive Health (iPH) iph.nl Gespreksinstrument2.0
成人用のクモの巣図に関する質問の例をそれぞれ挙げると、
①身体的機能
→「身体・体調について不満や痛みはありますか?」
②メンタルウェルビーイング
→「物事に集中できていますか?」
③生きがい
→「今の生活を受け入れていますか?」
④生活の質
→「幸せと感じていますか?」
⑤社会参加
→「誰か他者からの助けや支援はありますか?」
⑥日常機能
→「日々の生活で時間の管理はできていますか?」
この質問紙を患者に予め自宅もしくはクリニックで記入してもらいます。
クモの巣図にはそれぞれの領域ごとに質問の点数の平均を取って反映されます。
さて、ここからがPHの大事なステップ、クモの巣図の振り返りです。
Examples of detailed questions on the spider web diagram for adults are as follows
1) Bodily functions
→"Do you have any complaints or pain about your body or physical condition?”
(2) Mental well-being
→ "Are you able to concentrate on things?”
3) Meaningfulness
→”Do you accept your life as it is now?”
(4) Quality of life
→”Do you feel happy?”
5) Participation
→”Do you have any help or support from others?”
6) Daily functioning
→”Are you able to manage your time schedule in your daily life?”
Patients are asked to fill out this questionnaire at home or at the clinic.
The spider web diagram will reflect the average of the scores of the questions for each dimention.
Part.2 クモの巣図を振り返ろう Reflection of the spider web diagram
振り返りにあたり、2つの方法を用います。
①問題解決志向型の問いかけ
②アクションウィール法
それぞれについて見ていきましょう。
①問題解決志向型の問いかけ
これは患者自身に変化をもたらすような問いかけの方法です。
具体的には、クモの巣図を作成後、以下のような質問を患者に行います。
あなたが希望している状態はどんなことでしょうか?
それはどんな違いを生みますか?
何が効果的だと思いますか?
次のステップとはどういったものですか?
There are two practical methods for reflection.
(1) Ask solution-oriented questions
(2) Use the Action Wheel
(1) Solution-oriented questions
The aim of the question is to help care providers make patients think differently and to create a context for change. Specifically, after creating a spider web diagram, the following questions are asked to the patient.
- What do you hope for?
- What difference will that make?
- What will be effective?
- What will be the next sign of progress? Or: What will be your next step?
では問題解決志向型の問いかけを用いた具体例を見てみましょう。
Now let's see the example of using solution-oriented questions.
患者は58歳男性、3ヶ月前に心筋梗塞になった方です。
2人の娘と妻と一緒に家庭医を訪問しました。
事前のクモの巣図は全体的に6-7点程度の分布でした。
医師が現在の治療、特にリハビリテーションについて聞かれた際、患者は「リハビリはうんざり、何も改善している気がしない」と答えました。
そこで医師はまず「あなたが希望している状態はどんなことでしょうか?」と質問しました。
すると彼は声を詰まらせながら、「子供ともっと良い関係を作りたい」と回答しました。
医師は患者の思いを汲み取りながら、「この質問はあなたを感情的にさせますか?」と念押しすると患者はいよいよ泣き出しました。
続けて医師は娘に「父の泣いている姿をよくみますか?」と質問すると、娘たちは「父が泣いているのを見るのはこれが人生で2回目です」と答えました。
医師が一回目はいつかと尋ねたところ、娘は「それは3ヶ月前で、父が心筋梗塞で倒れた際に除細動器を装着した時で、父が泣きながら私はもう死んでしまう!!と叫んでいた」と答えました。
患者に対して、医師は「娘さんとの関係は死にたくないという気持ちと同じくらい大切なもので、それがあなたをより感情的にしていますか?」と質問したところ、患者はそっと頷いて、それを聞いた娘たちにも涙が流れました。

次のステップとして、医師は患者に「その側面について誰があなたを助けることができますか?」と質問しました。その時、隣の娘たちが手を上げました。その後さらに患者に話を聞いたところ、患者は「心筋梗塞後特に疲れやすく、落ち着かずイライラが積もり家族に当たることがある」と答えました。そして彼は自分が短気で怒りっぽくなっていることに気づき、それを治してまた家族仲良く過ごしたいと感じました。
それを聞いた医師は「次のステップとして何が大切でしょうか?」と質問しました。
隣にいた妻は「まずは娘たちに対して『ただいつも散らかしてばかりいる』と文句で終わる代わりに優しく部屋をきれいにしてもらうように声かけしたらどう?」と患者に提案したところ、家族の中でちょっとした笑いが起きました。
この話し合いの中で、患者はまずは娘に優しく接するためにベストを尽くすと約束しました。
2週間後のフォローの外来で彼は「家での雰囲気を変えたい、そしてそのために自分のイライラの原因を解明したい」と希望があったため、医師はメンタルヘルス専門の看護師との予約をとりました。
その後、カウンセリングの効果もあり彼のイライラは少しずつ解消され、結果的に家族との関係が良くなることで家族とやりたい目標ができ、リハビリにも自然と精が出るようになりました。
また、後々のクモの巣図では身体機能と生活の質を中心が特に点数に改善を認めました。
ここでのポイントは、医師は決して患者に「〜したほうがよい」と誘導せず、患者が自分の問題について自らリードして考えていくプロセスです。
また、この介入は「身体機能」と「生活の質」のスコアが伸びましたが、当初からクモの巣図をよくするためではなく、あくまで患者自身が自分の健康を見つめ、話し合いの中で問題を明らかにして、それに取り組んだ結果、その点が伸びたということにも着目しましょう。
The patient is a 58-year-old man who had a myocardial infarction three months ago.
He visited his family physician along with his two daughters and wife.
The preliminary spider web diagram showed an overall distribution of about 6-7 points.
When the doctor asked about his current treatment, especially his rehabilitation, the patient replied, "The rehabilitation is disappointing; I don’t seem to make any progress.”
So the doctor first asked, "What are you hoping for?"
He swallowed and says "I want to have a better relationship with my children.”
The doctor listened to him and asked, "Does this question make you emotional? The patient finally began to cry.
The doctor continued to ask her daughters, "Do you often see your father crying?” The daughters replied, "This is only the second time in our lives.”
When the doctor asked when the first time was, the daughters replied, "It was three months ago, when daddy had a myocardial infarction, and he was crying and screaming, 'I'm dying!’ ".
The doctor asked, "Is the relationship with your children as important as not wanting to die, and does it make you more emotional?". The patient nodded softly and tears flowed down his daughters' faces as they heard his answer.
As a next step, the doctor asked the patient, "Who can help you, in this respect?" The daughters both raised their hands. After further questioning, the patient replied that he kept so tired after the myocardial infarction, and he appeared restless and agitated because his recovery was not going well. He realized that he had become short-tempered and angry and he was taking his frustrations out on his family. Therefore, he wanted to fix it and get along with his family again.
Then the doctor asked, "What could be a first step in that direction? “.
His wife said, "How about you start by asking nicely when you want your children to tidy up, instead of ending with the comment that they never clean up after themselves? “. Everyone had to laugh at this heartfelt message.
During this discussion, the patient promised to do his best to treat her daughter kindly first.
At a follow-up outpatient visit two weeks later, he expressed his wish to change the atmosphere at home and figure out the cause of his irritability, so the doctor made an appointment with a mental health nurse.
After a few weeks, his irritability gradually dissipated due to the counseling, and as a result, his relationship with his family improved a lot. Moreover, he came up with some plans with his family, and he eventually became more motivated in his rehabilitation. Later, his spider web diagram showed improvement in scores, especially in bodily functions and quality of life.
The main point in this case is that the doctor didn’t tell the patient to "do something," but the patient took the lead in the process of coping with his or her own problems.
Also, despite that the scores of "bodily functions" and "quality of life" increased lastly, it is important to note that the increase was not due to aiming for the improvement of the spider web diagram from the beginning, but rather because of the patients themselves looking at their own health, identifying problems through discussion, and working on them.
②アクションウィール法
このアプローチ方法((図2:オランダ語)は、5つのステップを追って患者の健康問題について聞いていきます。
ステップ1.今はどうですか? あなたのクモの巣を見て、何か気づくことはありますか?
ステップ2. 何がしたいですか? あなたにとって大切なものは何ですか?
ステップ3.何ができるのか? 自分にとって何が実現可能ですか?
ステップ4.何を決めているのか? 最初の一歩は何ですか?
ステップ5. それをやらないことにした理由は何ですか?
5A:やらないことにした理由は何ですか?
5B:とにかくやるために必要なものは何ですか?

図1(Figure1): Institute for Positive Health (iPH) iph.nl. Applying action
(2) Action Wheels Method
This approach method ((Figure 2: Dutch) follows five steps to ask about the patient's health problems.
Step 1. How do you think about yourself now? What do you notice about your spider web?
STEP 2. What do you want? What is important to you?
STEP 3. What can you do? What is feasible for you?
STEP 4. What have you decided to do? What is your first step?
Step 5. What is the reason you have decided not to do it?
- 5A: What is the reason you have decided not to do it?
- 5B: What do you need to do it anyway?
こちらについても、具体例を見てみましょう。
患者は8歳の女の子で1型糖尿病を持っています。
母親と一緒に腹痛を主訴に家庭医を受診しました。
母は特に娘の腹痛を心配していました。医師はまず、事前に小児科の専門医の診察も受けたのか話を聞くと、母は「小児科の先生にも調べてもらったものの、特にこれ以上加療するような病態は見つからなかった、痛みは我慢するしかないと言われた」と答えました。
実際に医師が行った診察でも腹痛の原因について新しい手がかりは見つからず、機能性の腹痛(特に重大な病気が背景にあるわけではない、原因不明の腹痛の総称)が疑われていましたが、母親はもっと詳しい検査を医師に希望しました。
そこで医師は、女の子に向けて小児用の簡易版ポジティヴヘルスの質問紙を渡し、それを埋めてもらい次回予約で話し合うことにしました。

その後の外来で、医師は女の子に「あなたにとって何をしているときが一番大切ですか?」と質問すると「学校の友達が一番大切」と答えました。
この時の彼女のクモの巣図は「社会参加」と「身体機能」が特に点数が低い状態でした。
医師は続けて「もっと楽しい気分になるにはどんなことができたらいいですか?」と質問。すると患者は「友達の家に行って遊んだり、家に泊まったりしたい」と答えました。
この時母は娘について、糖尿病があることから学校以外の外出を一切許していませんでした。
というのも、母は娘のインスリン注射の管理について常に目の届く範囲に留めておきたいと思っていたためです。
そこで医師は「もっと友達と交流できるようになるにはどんなことがまず必要だと思いますか?また、初めにできることとしてはどんなことがありますか?」と尋ねました。すると女の子は、友達の母親も彼女の糖尿病について管理するのを許すのはどうかと母親に聞きました。母親は「ちょうど新しいパッチ型の糖尿病センサーの装置を受け取ったので、毎回注射を確認しなくてもいいかもしれない。正直、不安はまだ残るけどその装置があれば確かに娘の友達の家に行っても大丈夫かもしれない」と答えました。
まだ納得したような雰囲気ではない母親の様子を感じた医師は、さらに「このプランについてお母さんにとって妨げになっていることはありますか?」と重ねて尋ねました。
すると、母親はしばらく黙った後、涙を流しながら「実はいまだに娘の糖尿病について受け入れることが難しくてそれが辛い」と胸の内を告白しました。
医師は母親に対してこの気持ちと向き合うのを助けるべく、糖尿病専門の看護師に加えて、メンタルヘルス専門看護師との予約も勧めることにしました。
その後、母親は話し合ったプランを元に娘の友達の家でのお泊まりを認め、母親自身もカウンセリングを重ねながら少しずつ娘の状態について向き合う時間を作りました。
そして、その後女の子は腹痛を主訴に病院を受診することは無くなりました。
この例ではクモの巣図とアクションウィール法の面接を組み合わせることで腹痛だけではなく、友達との遊びができない女の子の苦悩を見つけることができ、さらに女の子の母親が抱えている不安や娘の病気の事実を受け入れられない本当の感情にも向き合うことができました。
また、クモの巣図での「社会参加」と「身体機能」の低値は女の子の本当の悩みを紐解く上での手がかりであり、健康問題の可視化を助けました。
以上、アプローチ別に2つの事例を紹介しました。
このようにクモの巣図をベースにメソッドに準じた振り返りにより実際に患者さんの健康にまつわる問題にアプローチすることができるのです。
Let's look at a specific example here as well.
The patient is an 8-year-old girl with type 1 diabetes.
She and her mother visited the family doctor with abdominal pain as the main complaint.
The mother was particularly concerned about her daughter's abdominal pain. The doctor first asked the mother if she had been examined by a pediatrician. The mother replied that she had been examined by the pediatrician, but he had found no particular condition that warranted further treatment, and that she would have to tolerate the pain.
The doctor's examination did not reveal any new clues as to the cause of the abdominal pain, and he suspected functional abdominal pain (a general term for abdominal pain of unknown cause that does not have any serious underlying disease), but the mother wanted the doctor to perform a more detailed examination.
The doctor gave the girl a simple pediatric version of the Positive Health Questionnaire, which she was asked to fill out and discuss at her next appointment.
In a subsequent outpatient visit, the doctor asked the girl, "What is most important to you in your life?". She replied, "My friends at school are the most important”.

Her spider web chart at this time showed particularly low scores for "participation" and " bodily functions”.
The doctor continued, "What would make you feel happier?" The doctor continued, "What could you do to feel more comfortable?”. The patient replied, "I would like to go to my friend's house to play and stay at home”.
At this time, the mother did not allow her daughter to go out outside of school at all because of her diabetes.
She wanted to keep her daughter's insulin injections under control at all times.
So the doctor asked, "What do you think is the first thing she needs to do to be able to interact more with her friends? And what are things we can do first?". The girl then asked her mother if she would allow her friend's mother to check her insulin. The mother replied, "I just received a new patch-type diabetes sensor device, so I may not have to check it by myself every time. To be honest, I still have some concerns, but with that device, she may indeed be able to go to her friend's house".
Since the mother still did not seem convinced, the doctor asked again, "Are there any obstacles for you with this plan?" . The mother was silent for a moment and then, with tears streaming down her face, confessed that she still had difficulty accepting her daughter's diabetes and that it was painful for her.
The doctor recommended that the mother make an appointment with a mental health nurse in addition to the diabetes nurse to help her deal with these feelings.
The mother then allowed her daughter to stay over at a friend's house based on the plan we discussed, and the mother herself gradually made time to confront her daughter's condition through a series of counseling sessions.
After that, the girl no longer visited the hospital with abdominal pain as her main complaint.
In this case, the combination of the spider web diagram and the Action Wheels interview enabled us to find not only the abdominal pain, but also the girl's distress at not being able to play with her friends, as well as the girl's mother's anxiety and true feelings of not being able to accept the fact that her daughter was ill.
In addition, the low values of "participation" and "bodily functions" in the spider web diagram were clues in unraveling the girls' real distress and helped visualize their health problems.
In this way, we can actually approach patients' health-related problems by reflecting on them according to the method based on the spider web diagram.
【今後のポジティヴヘルスの展望】
今回は主に診療所の場面においてポジティヴヘルスの使用についてご紹介しました。
オランダでは将来の診療の場において、ポジティヴヘルスを用いたアプローチはとりわけ健康に関して多様で複雑な背景のある患者(ホットスポッター)に対して効果的であるという期待があります。ホットスポッターとは具体的には以下のような因子を持つ方を指します。
1. 慢性・反復性の精神疾患がある、精神科への入院を繰り返す
2. 年間複数回の入院歴がある
3. 30日以内の再入院回数が多い
4. 一つ以上の慢性疾患がある
5. 3人以上の専門医による治療を受けている
6. 腫瘍病変があり、多くの検査、高次医療機関で治療を受けている
7. 緩和ケアを受けている
8. ポリファーマシー(多くの薬剤を内服している状態)がある
9. 薬物乱用歴がある
10. ホームレスである
11. ぜい弱性がある (フレイルがある)
12. 孤独である
13. 高齢である
In this blog I introduced some practical ways of Positive Health mainly in the clinic setting.
In future practice settings in the Netherlands, it is said that the Positive Health approach will be particularly effective for patients with diverse and complex health backgrounds (called ‘hot spotters’). Specifically, hot spotters are those with the following factors.
1. chronic or recurrent psychiatric illness, repeated psychiatric hospitalizations
2. a history of multiple hospitalizations per year
3. frequent readmissions within 30 days
4. one or more chronic illnesses
5. treated by more than 3 specialists
6. has a tumor lesion and is undergoing many tests and treatment at a higher level of care
7. receiving palliative care
8. has polypharmacy (taking many drugs)
9. has a history of substance abuse
10. homeless
11. has frailty (frail)
12. lonely
13. old age
ある家庭医のクリニックでの40名のホットスポッターを対象とした研究では、ポジティヴヘルスのアプローチを用いた面接により、患者の健康問題の改善やクモの巣図の点数の上昇、そして医療費の削減にもなるという結果が出ました。
また、更に診療現場以外の場面の例としては、カナダ在住のコロンビア人医師でかつ研究者のAlex Jadad氏が、ポジティヴヘルスのコンセプトをベースに様々なITテクノロジーを用いて地域住民、政府、医療、保険会社などがつながるネットワークサービスを作成しています。
具体的にはユーザーそれぞれに個別化されたウェルビーイングの評価や、最適な健康状態の実現を助けるインキュベーター(サポート役)として機能する健康アプリの開発を行い、そこに政府の医療サービス、医療機関、保険会社などの各種ステークホルダーが連携することでテイラーメイドなサービスを提供できる���制にしています。これにより実に9万5千ヶ所組織に所属する400万人以上の人々に健康にまつわる意思決定支援やネットワーク構築を行い、サービスユーザーの医療費をOECD諸国全体の平均支出額のわずか25%までコストダウンしたとされています。
このように今後ポジティヴヘルスは組織のネットワーク作りやプロジェクトの運営などにも利用されていくことが期待されます。
There was a study with 40 hot spotters at a family physician's clinic in the Netherlands, and it indicated that interviews using the Positive Health approach improved patients' health problems, increased spider web chart scores, and reduced health care costs.
As a further example of an off-site application, Alex Jadad, a Colombian physician and researcher in Canada, has created a network service that connects local residents, government, healthcare, and insurance companies using various IT technologies based on the concept of Positive Health.
Specifically, he has developed a health care app that will act as an incubator to help each user achieve an individualized wellbeing assessment and optimal health status, and by linking various stakeholders such as governmental medical services, medical institutions, and insurance companies to the app. Thus, the app can provide tailor-made services, health-related decision support and networking to more than 4 million people in 95,000 organizations. Moreover, it is said to have reduced the cost of health care for service users to only 25% of the average spending in the OECD countries as a whole.
Therefore, it is expected that Positive Health will be used for organizational networking and project management in the future.
更に2021年11月11日にはポジティブヘルス生誕10周年記念式典もあり、開発者のMachteld Huber医師をはじめとした基調講演、そして医療、教育、都市開発、健康管理サービスなど各分野の第一線で活躍するスピーカーによりそれぞれの分野でのポジティヴヘルスの活用についての紹介やワークショップがありました。会場には日本に初めてポジティヴヘルスを紹介した翻訳家のシャボットあかね氏をはじめ、多くの方々が来場していました。

写真1 : 筆者 (左)とHuber医師 (中央)、シャボット氏 (右)
Picture 1: author (left), Dr. Huber (center), Ms. A Chabot (right)

写真2 : 筆者 (左)とJadad氏 (右)
Picture 2: author (left), Dr. Jadad (right)
The 10th anniversary of Positive Health was celebrated on November 11, 2021, with keynote speeches by Dr. Machteld Huber, the developer of Positive Health, and speakers from the front lines of medicine, education, urban development, and health care services, who introduced the use of Positive Health in their respective fields. The event also featured workshops and introductions to the use of Positive Health in various fields, including medicine, education, urban development, and health care services. Many people attended the event, including Ms. Jeanette Akane Chabot, a translator who first introduced Positive Health to Japan.
今後の様々な可能性を秘めているポジティヴヘルスは、少子高齢化をはじめとした健康を取り巻く環境がより複雑化した日本でも活躍する場面があるかと私は思います。
本ブログを契機に読者の皆さん、一人一人が健康について見つめ直して、もっと考えを深める助けになれば幸いです。そしてもし興味があれば、是非共にポジティヴヘルスについてもっと学び、実践していきましょう。
今回はポジティヴヘルスの応用編ということで、最後までお読み頂きありがとうございました。
Positive health has many possibilities for the future, and I believe that it will play an active role in Japan, where the environment regarding health has become more complex, including the declining birthrate and aging population.
I hope that this blog will help you to rethink and deepen their thinking about health. And if you are interested, let's learn more about positive health together and put it into practice.
Thank you for reading to the end!
引用文献(Reference)
Huber M et al. Handbook Positive Health in Primary Care -The Dutch Example-.2022 Houten. bohn stafleu van loghum
【オランダ語とオランダのスナップショット(Snapshot of the Netherlands)】
-本日のオランダ語レッスン(Today’s Dutch lesson)-
‘Gefeliciteerd’ (ヘフェリシテード)
これはオランダ語で「おめでとう」という言葉です。
誰かの誕生日や結婚、出産、合格、卒業などのお祝いの場でもよく使われます。
オランダの大学では学期毎に2月、もしくは9月に卒業式があります。
私事ですが、昨年ライデン大学の大学院を無事に卒業できることとなりました。そこで多くのオランダの友人からも‘Gefeliciteerd’という嬉しい言葉を頂きました。日本にいる皆さんの周りでも、誕生日や結婚、出産などはもちろん、これから冬から春にかけて、受験や就職、卒業、など多くのめでたい節目が来るかと思います。ぜひ、いつもの「おめでとう」に加えて、オランダ式の祝辞もいかがでしょうか?
This is the Dutch word for "congratulations.
It is often used to celebrate someone's birthday, marriage, birth, passing exams, graduation, and other happy occasions. In the Netherlands, graduation ceremonies are held every semester in February or September. On a personal note, I am pleased to announce that I graduated from the graduate school, university of Leiden successfully. I was very happy to hear the word 'Gefeliciteerd' from many of my friends. I am sure that many of you in Japan will be celebrating birthdays, marriages, births, and other happy milestones from winter to spring, such as entrance exams, employment, graduation, and so on. In addition to the usual "congratulations," how about giving a congratulatory message in Dutch?
Photo(1): ライデン大学アカデミック校舎(大学最古の建物。400年以上の歴史がある)
ライデン大学の全学部の学士、修士、PhDなどの卒業式が行われる会場でもある
Leiden University Academic Building (oldest building at the university, with a history of more than 400 years). It is also the venue for Leiden University's graduation ceremonies for Bachelor, Master, and PhD.

Photo (2): 校舎に併設されたチャペル。ここで卒業証書授与を行います。
Photo (2): The chapel attached to the school building. Diplomas are conferred here.

Photo (3): 大学院卒業証書授与式にて筆者と学友との写真(この日に合わせて袴を着ました)
Photo (3): Photo of author with his classmates at the graduation ceremony (I wore ‘Hakama’ Japanese traditional cloths for ceremony).

Photo (3): ライトアップされた夜のライデンの街。クリスマスから冬の間は続く
Photo (3): The city of Leiden at night with light up. It lasts from Christmas holidays to whole winter times.

Photo (4): 冬晴れの太陽が照らすKatwijkのビーチ。北海に面し、海の向こうにはイギリスがある。
Photo (4): The beach in Katwijk lit by the winter sun. The beach faces the North Sea, with UK on the other side.

それでは、また次回のブログでお会いしましょう!
Tot zien in de volgende blog (See you in the next blog) !
1 note
·
View note
Text
Lekker met Nederland! vol.5 (元Dr.コトーの蘭学手記)
皆さん、大変大変、ご無沙汰しています。
お待たせしました!
新年最初のブログは、前回の予告通り、オランダの「ポジティヴヘルス」についてご紹介します。
Hi everyone, it's been a very long time. Sorry for my delay!
For my first blog of this year, I would like to introduce "Positiv Health" as previously announced.
【ポジティヴヘルスとは?What is “positive health” ?】
まず初めに「健康」と聞くと皆さんどんなことを思い浮かべますか?
きっと「病気や怪我がないこと」がまず思い浮かぶのではないでしょうか。また、「悩みやストレスがないこと」、「気持ちが充実していること」、「仕事があって生活ができること」、「家族や友人がいること」等々人によって様々な答えがあるかもしれません。
一方で医療の世界ではどうでしょうか。今COVID19(新型コロナウイルス)でも話題の世界保健機関(WHO)が1948年に定めた定義では、健康とは「単に疾患がないとか虚弱でない状態ではなく、身体的・心理的・社会的に完全に良い状態」というものと定義されています。
しかし医療の進歩や平均寿命の延長に伴い、定義が提唱された当時のような致死率の高い急性疾患(結核や下痢合併の胃腸炎など)を持つ人よりも、治癒が困難な難病を抱えて生きる人や慢性疾患や加齢に伴う身体機能の低下を抱える人、精神疾患を抱える人など現代における疾病の内訳はこの70年ほどで大きく変化しています。
First of all, what do you think of or imagine by “health” when you hear the word?
I'm sure that the first thing that comes to your mind is "no illness or injury. The answer may differ from person to person, such as "no worries or stress," "feeling content," "having a job and being able to make a living," or "having family and friends.
On the other hand, how is it understood in the medical field?
In 1948, the World Health Organization (WHO) defined health as "a state of complete physical, psychological, and social well-being, not merely the absence of disease or infirmity. However, with the healthcare has developed, and the average life expectancy has also increased. The environment of healthcare has changed dramatically over the past 70 years. There are now more people living with diseases that are difficult to cure, chronic diseases, age-related decline in physical function rather than the people with acute diseases (such as tuberculosis and gastroenteritis complicated by diarrhea).
そんな中で、このWHOの定義を忠実に守った場合、身体的・心理的・社会的に「完全に良い状態」というのがいかに限定された状態であるかがわかり、逆を返せばそれに当てはまらない人は「健康ではない=不健康」の烙印を押されかねないことにもなります。
実際、現在の医療の目的の多くはこのWHOの指す「健康」を目指して積極的に患者へ治療介入していく流れとなっています。
In such a situation, if we namely follow the WHO definition, we can see how difficult the state of "perfectly good health" is and in other words, people who do not fit this definition may be regarded as "unhealthy.
In fact, many of the current objectives of healthcare are active interventions or treatments of patients in order to achieve "health" as defined by the WHO.
具体的には血圧、血糖値、脂質、BMIなどのパラメータを「健康」と見なされる正常値へ持っていくために薬剤をはじめとして様々な治療介入をしています。それに加えて最近では人間ドックなどで予め身体に「異常=不健康な状態」がないか検査する人も増えています。
もちろん、誰しもが「健康」でありたいのは事実ですが、その「健康」が絶対的な目標で誰しもが「完全に良い状態」を目指す結果、私たちは現在の自身の状態について常に「健康」かどうか不安を抱えたり満足に至らず、また本来必要な対象の患者を超えてのスクリーニング検査や様々な精密検査・治療への要望が増加し、医療現場での業務負担や医療費が年々膨れ上がっているのも実情です。
Specifically, various therapeutic interventions are oriented by biomedical parameters such as blood pressure, blood sugar, lipids, and BMI and they are prone to be corrected to normal values that are considered "healthy. In addition to this, more and more people are having their bodies checked for "abnormalities" (i.e. unhealthy conditions) beforehand through physical examinations.
Of course, everyone wants to be "healthy," but as a result of the fact that "perfect health" is an absolute goal, we are constantly worried or unsatisfied with our current state of "health”. Therefore, the workload and the costs in the medical field are increasing year by year.
そんな従来の「健康」について新しい定式を提案したのがオランダ人の元家庭医、Machteld Huber (マフトルド・ヒューバー)です。ヒューバー医師は健康に対してWHOの定めたような定義ではなく、新しいコンセプト(概念)として「社会的・身体的・感情的問題に直面したときに適応し、みずから管理する能力としての健康」という定式を打ち出しました。
この2011年に初めて打ち出された定式こそが、今回お話しする「ポジティヴヘルス」となります。
A Dutch family physician, Dr. Machteld Huber, has proposed a new definition of health. Instead of the WHO definition of health, Dr. Huber proposed a new concept: "health as the ability to adapt and manage oneself in the face of social, physical, and emotional problems.
This concept, which was first formulated in 2011, is indeed the "positive health".
ヒューバーによると健康とは、自分が抱えているチャレンジに対応することを学ぶプロセスであり、ある一定の状態を示すのではなく、常に状況によって変化し得るものという捉え方です。そして誰かから与えられるものではなく、患者自らの観点を基に本人が主導権をもて自分自身の状態を決めるプロセスとしています。
According to Dr. Huber, health is a process of learning to cope with one's own challenges, and is not a fixed state of being, but one that can always change depending on circumstances. It is not something that is given to you by someone else, but rather a process in which you take the initiative to determine your own condition based on your own perspective.
とりわけポジティヴヘルスにおいては、その構成要素を大きく6つの次元に分けています。
その6つの次元とは、
①「身体的機能(Lichaamsfuncties)」:身体に対する不安、痛みや苦痛の程度、睡眠、食事、運動etc…
②「メンタルウェルビーイング(Mentaal welbevinden)」:集中力、自己肯定感、感情制御、不安etc…
③「生きがい(Zingeving)」:意味のある人生、理想や目標、感謝の気持ち、結婚・交際etc...
④「生活の質(Kwaliteit van leven)」: 娯楽、幸福感、バランス、自由、住宅環境、経済状態etc…
⑤「社会参加(Meedoen)」:社会との接触、共同作業、会話・コミュニケーション、交流etc…
⑥「日常機能(Dagelijks functioneren)」:自律心、健康への知識、就労可能性、限度を知るetc…
です。
このモデルをいわゆる「クモの巣図」として以下のように提示しています。
In particular, positive health is divided into six major dimensions.
The six dimensions are
1) Physical functioning (Lichaamsfuncties): anxiety about the body, degree of pain and suffering, sleep, diet, exercise, etc.
2) Mental wellbeing (Mentaal welbevinden): concentration, self-esteem, emotional control, anxiety, etc.
3) "Zingeving": meaningful life, ideals and goals, gratitude, marriage/relationship, etc...
4) "Quality of life (Kwaliteit van leven)": entertainment, happiness, balance, freedom, housing conditions, economic conditions, etc...
5) "Social Participation (Meedoen)": Social contact, collaboration, conversation/communication, interaction, etc...
6) "Dagelijks functioneren": autonomy, knowledge of health, possibility of employment, recognition of own limitations, etc.
This model is presented as a so-called "spider web diagram" as follows.
ここで大事なのは、この6次元の要素が新しい「健康」の定義ではなく、あくまで健康について考える上で助けとなるコンセプトであるということです。
医療者と患者さんはこのモデルをもとに話し合い、各項目についてどれくらい満たされているのか点数をつけていきます。
それぞれの項目を可視化して、定量化することで自分は今後どのような「健康」の状態でありたいか、自分の状態を把握する上で大事な資料となります。
The health care provider and the patient discuss the model, and score the grade to which dimension is met each other. By visualizing and quantifying each dimension, it becomes an important tool for understanding what type of "health" you want to increase for the next step.
しかしここで大事なポイントがあります。これはあくまで自分が考える健康を可視化するためのツールであって、このクモの巣図を満点に埋めることが目標ではありません。
人間毎日色々なことがあります。仕事や勉強がうまくいかなくて自信ややる気が出ない、そうなると「メンタルウェルビーング」の項目は下がるでしょう。一方でそんな時にそばにいる友人や家族と食事しながら励まされて明日も頑張れる、と思うようであれば「社会参加」の項目が上がります。このように健康はそれ自体が目標なのではなく、自分の日々を様々な視点から分析してみて今、何が満ち足りていて何が足りていないのか、そういうナラティブな目線で見ていくという考えで成り立っています。
But You should be careful. This is just a tool to help you visualize your own health, and not a goal to fill this spiderweb chart to the fullest. Every single day is actually different.
For example, if your work or study doesn't go well, then you may feel less confident or motivated. Therefore, the "mental wellbeing" item will probably go down. On the other hand, if you feel better after being encouraged by your friends and family over a meal, the "social participation" item will go up.
Health is not a goal in itself, but rather a narrative concept that allows us to analyze our own days from various perspectives and see what we are and are not satisfied with.
【オランダの医療環境との関連-Relationship with the Dutch healthcare envrionment-】
では、このポジティヴヘルスはどのように医療に反映されているのだろうか?
2011年にBMJの論文で初めてポジティヴヘルスを紹介して以来、ヒューバー医師の精力的な研究と普及に向けた宣伝、そして最終的にはオランダ政府の健康・福祉・スポーツ省(日本でいう、厚生労働省)の諮問機関(ZiNL)の「ケア専門職と教育におけるイノヴェーション委員会」のメンバーとして医療政策に取り入れる活動をしています。
実際の現場としては、家庭医など医師が患者とのコミュニケーションツールとしての使用以外にも、例えばビュートゾルフと呼ばれるオランダ最大の民間の訪問看護グループにおける利用者のためのケアプラン作成への活用や、アムステルダム市などオランダ国内にある各自治体の主導の下、健康センターでの医療・福祉サービスに向けた多職種連携での支援の指針に使用するなど、多岐にわたってポジティブヘルスは受け入れられています。
これによりこれまで制度として一律に行われてきたケアサービスの見直しを行い、個人個人の健康やwell-being(幸福な状態)に対する要望に合わせたサービス提供ができるようになりました。
So how is this positive health reflected in the Dutch healthcare system?
Since her first introduction of positive health in a BMJ article in 2011, Dr. Huber has been actively researching, promoting, and eventually incorporating it into health care policy as a member of the Innovation in Care Professions and Education Committee of the ZiNL, an advisory body to the Dutch Ministry of Health, Welfare and Sport (in Japan, the Ministry of Health, Labour and Welfare). As a member of the "Innovations in Care Professions and Education Committee" of ZiNL, she is currently working to incorporate this into healthcare policy.
In practice, in addition to being used as a concept for general practitioners to communicate with their patients, the system is also being used to create care in some home-visit nursing services in the Netherlands, such as Buurtzorg. In the Netherlands, positive health is widely accepted and relfected in the part of protocols for the healthcare servies by the local municipalities.
As a result, many of systemic care services are arranged in accordance with the individual health and well-being status.
それではなぜオランダではこのようにポジティヴヘルスが広く浸透するようになったのでしょうか?それにはオランダの歴史と医療制度の特性が関係しています。
オランダの福祉の歴史は長く、遡ること中世の頃から「ホッフェ(hofje)」と呼ばれる貧困層向けの共同住宅を作り人々が助け合っていました。その後19世紀には民間団体や教会が社会的弱者への支援を積極的に担い、20世紀以降の福祉国家樹立への礎となりました。
やがて1950年代になるとオランダ社会では様々なイデオロギー、宗教、人種の人々がお互いのコミュニティを形成するいわゆる「柱状社会(verzuiling)」になります。
この柱状社会においてはそれぞれのコミュニティで独自の学校、新聞、そして地区ナースや地域のインフォーマルケアのボランティアなどが存在してそれぞれ近所の人々が助け合うという構図が出来上がりました。1960年以降からは徐々に中央集権型の社会構造へ移行して現在のオランダ政府が中心となる社会になりました。
このような歴史的経緯からボランティア精神は古くからオランダ国民に染み渡っています。
そしてこのポジティヴヘルスを実践するには本人と医療者はもちろん、地域住民や友人、家族など本人を取り巻く多くの人々が重要な存在となります。というのも、ポジティヴヘルスは��りの人と一緒に関わりながら、お互いの健康を考えるツールだからです。
医療の現場では医師や看護師がこのコンセプトに沿って、医学生物学的な観点によるケアによらず様々な生活項目を考えながら健康について分析します。すると患者さんが望む「健康」のあり方が更に理想に近づくには医療による介入より、むしろ患者さんの日々の生活状況や考えの変化に答えがあることに気づき、それを実践するには医療・介護従事者だけではなく家族や友人、近隣住民など多くの人の助けも重要であることがわかります。
So why has positive health become accepted widely in the Netherlands? There are some clues in the history of Dutch welfare system.
The origin of Dutch welfare system can trace back to the Medieval Ages, when people helped each other by building community apartments called "hofje" for poor people. In the 19th century, private organizations and churches took a main role in supporting the socially welfare, which became the foundation for the establishment of the welfare state in the 20th century and beyond.
In the 1950s, Dutch society became a"pillar (“verzuiling") society, where people with various ideologies, religions, and races formed communities with each other. From 1960 onwards, it had shifted to the more centralized social structure.
Because of this historical background, the spirit of hospitality has been rooted in the Dutch culture.
In order to carry out positive health, not only the patient and the medical staff, but also many stakeholders, such as neighbors, friends, and family, are important. This is because positive health is a tool to think about one’s own health with the process of interaction between all those stakeholders.
In the medical field, doctors and nurses follow this concept and clarify patients’ health by considering various dimensions of their lives, not just from a medical-biological perspective. Then, you realize that patient's desired health lies not in medical intervention, but rather in changes of daily living conditions in the interactive way.
【これからの展望について-Future perspectives-】
ご存知の通り、現在世界中でCOVID-19の流行が広まっており、多くの方々が健康不安を抱えたり、命について考えたり、そして社会の感染制御に伴う様々な制限によって自由や仕事、幸せのあり方について考えたりと、かつてない困難に直面しています。
健康についても正にこのような様々な因子が関係しており、これまでの「身体的・心理的・社会的に完全に良い状態」を目指すのはほぼ全員にとって難しい状態であり、むしろポジティヴヘルスのような「自分にとっての「健康」を考える」視点がより大事な時代になったと個人的に感じています。
このように健康について考える視点を持つポジティヴヘルスは非常に興味深い分野である一方で、個人による解釈が大きく関わってくるため医学における学術研究としての分析、特に質問紙票など具体的なスケール化やそれに科学的妥当性を求めるというようなアプローチは難しく、実際にポジティヴヘルスを導入するにはまずは医療・介護従事者が上記に話したようなコンセプトの意味を十分に知る必要があります。
そしてまずは医療・介護従事者自身が自分の健康について考えることも大事かと思います。
日本でも最近は徐々に広まりつつある「ポジティヴヘルス」、この流れがより進み多くの人が「健康」について自由に誰かと一緒に考えたり分析できるだけで、その人の幸福感や人生観が変わるでしょう。
最後までお読みいただきありがとうございます。
As you know quite well, the COVID-19 pandemic is now spreading all over the world, and many people are faced with multiple challenges about value of life, such as health concerns, meaning of life, freedom, working, and happiness. There seems to be no one who meet the definition of “the perfect health” according to WHO any longer. It implies we are living in the period where we have to think about our own "health" from our perspective, like the way of positive health.
Although positive health may be a crucial concept for the new era, it is still difficult to discuss in an academic field because the concept consists of a lot of interpretation and bias by individuals. Therefore, it is hard to make specific questionnaires for scaling positive health or to validate it as an uiversal tool.
In order to proceed positive health in practice, first of all, health caregivers need to fully understand the meaning of positive health and try it for themselves.
Positivistic health is gradually spreading in Japan, and it is likely that this trend will continue. I hope more and more people are aware of "health" as their own choices or discussable topics, and it will change their outlook on life to be much happier.
Thank you for reading to the end.
-Today’s Dutch Lesson-
‘Mooi’ (モーイ)
This is also one of the most common Dutch words you hear in your daily life. The original meaning is “cute” or “beautiful”, but you can also use it as “nice” in different situations such as `Lekker` (check my blog vol.3!).
Example(1): night view of the old city Leiden

Nederland: De straat is heel mooi met de sneeuw !
English: The street is so cute with snow!
日本語:街通りは雪でとてもきれい!
Example(2): the canal in Leiden

Nederland: Hij is een echt mooie eend!
English: He is a very cute duck!
日本語:とても可愛いアヒルだ!
Example(3): the ceremony of “Seijinsiki(成人式)*” at my friend’s place
*Seijinsiki: It is translated into “Coming of Age Day” in English. It is a Japanese holiday to congratulate people who became 20 years old at the ceremony. Men usually wear suits or kimono (traditional clothes) and women wear kimono, and they look so “mooi”! I celebrated my friends who turned 20 y.o. as “the substitute of the mayor of Leiden” lol.

Nederland: Het staat jullie zo mooi!
English: You guys looks so nice!
日本語:とても(着物)が似合っているよ!
Okay, now you know `Gezellig`, `Lekker` and `Mooi`. They’re all very positive expression and stand for Dutch people’s mind. Here in Leiden, the weather is getting so warm and it already sounds like coming of Spring.
`Wat mooi weer! Het is perfect voor lopen (What a nice day! It’s perfect for walking)’. See you on the next blog!!!

0 notes
Text
Lekker met Nederland! vol.4 (元Dr.コトーの蘭学手記)
Lekker met Nederland! vol.4
(元Dr.コトーの蘭学手記)
皆さん、こんにちは!
前回のブログでは次回は「ポジティブヘルス」についてお話しする予定でしたが、その前に今回はCOVID-19(新型コロナウイルス )感染症について少しオランダ国内の状況についてお話ししたいと思います。 (2020/5/31現在)
※ I did not make English version this time because of too many contents about corona virus. I’m sorry for this inconvenience but I will for the next blog!
<目次>
・時系列
・社会情勢
・医療体制
・社会保障
【時系列:2020/1/31-5/31】
2020/1/31: WHOが非常事態宣言(国際的に懸念される公衆衛生上の緊急事態 (PHEIC))発動
その頃オランダ国内ではまだ感染例は一例もなし。
RIVM(オランダ政府の厚生労働省)の発表ではオランダでは大規模なパニックは起こらない。仮にOutbreakが生じてもコントロール可能と話していた。
https://www.nu.nl/weekend/6027173/dit-gebeurt-er-in-nederland-als-het-coronavirus-zou-worden-aangetroffen.html
2020/2/2: 中国武漢から帰国したオランダ人15名が全員到着後14日間自宅隔離となったがこの際は特に他に感染は広がらなかった。
オランダの国際空港はアムステルダム近郊にあるスキポールSchiphol空港が最大だが、武漢とオランダとの直行便はなく、中国からの乗客についても特に空港到着時に体温測定などは行わなかった。
2020/2/27:オランダ南部のブラバント州(Brabant)にて国内初となるCOVID-19陽性の感染者が発生(56歳男性)。この男性は2月21日出張先のイタリアから帰国。
ちょうどその際ブラバント州ではカーニバルイベントが行われていた。
元々カトリック教徒の多い州でカーニバルはこの地方では盛んに行われており、この男性も参加していた。オランダ最初のクラスター発生事例。
また、遡ること2月15日に同州の病院を受診した49歳女性がウイルス検査で、後に陽性であったことが判明。
政府は後に2月15日にはオランダ国内にウイルスが持ち込まれたと発表している。
その後ブランバント州の病院などで複数の医療関係者の感染の報告があった。
感染した医療者の大半は患者に直接接していない一方で、最初の患者がいたカーニバルに居合わせていた人も何名かいた。
2020/2/28:オランダで国内二例目の感染者が発生。
首都アムステルダムの隣町ディーメン(Diemen)に住む女性が2月23日に北イタリアロンバルディア州のスキー旅行から戻った後に体調不良となりアムステルダム市内の病院を受診して発覚。すぐに自宅隔離となった。
2020/3/1: アムステルダム市内の病院で10日に入院歴のある患者が外来受診し、ウイルス陽性反応。しかし明らかな感染経路は不明。その後もSchiphol空港や周辺都市のホーフトドロープHoofddorpなどで計10名の感染者が発覚。
2020/3/6: ロッテルダムRotterdamで国内初のウイルスによる死者が発生。86歳男性であった。
2020/3/8: オランダ政府がコロナウイルスの正式な感染者を発表。
その時点で感染者72名、うち14名が入院、2名が死亡
2020/3/9: ルッテRutte首相が記者会見を行い、衛生政策について発表。
「咳エチケット」、「手洗い」、「握手」の自粛をお願いする内容だった。
また感染の広がるブラバント州では自宅勤務が推奨された。
同時期に南オランダ州のフーレー・オーバーフラッキ島と呼ばれる小さな島の教会で礼拝後に次々と住民が体調不良となり、ウイルス感染と判明。最終的に19人もの住民が亡くなった。
オランダ国内初、離島でのクラスター発生。そこの教会の牧師はその前の週にレバノンに旅行しており、その際に持ち込まれた可能性も指摘されるも感染経路は明らかではない。
2020/3/11 オランダ国内の感染者は500名を超えて503名、62名の入院、5名の死亡となり。
この頃オーストリアやアイスランドのスキー旅行から戻ったオランダ人旅行者が国内各地に散らばりそれぞれの場所でウイルス陽性となる(感染者の分散)。
同時期にオランダ北部のフリースランドFrieslandやフローニンゲンGroningenなどでも感染者が発生。これでオランダ国内全域に感染者が発生したこととなった。
3月11日を境にオランダではパンデミックになったと認識されております。
2月15日〜3月11日までの動向をまとめると、
① はじめのウイルスの持ち込みは北イタリアロンバルディア州を旅行した人から発生。
カーニバルや宗教行事を通してブラバント州を中心にオランダ南部で感染が拡大。
② 3月初めには首都アムステルダムで患者が発生。感染経路は不明。
③ 3月からオーストリアやアイスランドなど周辺ヨーロッパへスキー旅行へ行った人が感染。
その後オランダ国内全土へと広がる。
その後の経過
2020/3/12: 政府より社会的接触の禁止処置の発表。
内容は100人以上の会合の中止
博物館、コンサートホール、劇場、スポーツクラブ、大会などのイベント中止。
また自宅勤務をオランダ全国に推奨、また海外旅行の自粛要請などが施行。
2020/3/15: オランダ国内でトイレットペーパーやパスタ類などの物品・食材の買い占めが続出。
またオランダ国内で死者が1000名を超えた。
18時にロックダウンの発表(飲食・スポーツ・理容・学校・風俗)全ての営業の停止
人との間を1.5m以上間隔を空けて行動。
一部の外食店はテイクアウト許可。合法麻薬販売店も不正取引防止のために一部許可
2020/3/16: 首相の緊急演説。感染拡大は止められず、集団免疫戦略を講じると説明。
全ての病院は入院患者への面会を中止
38度以上の発熱や風邪様症状のある人は自宅待機を命じられる。
呼吸困難など重篤な症状が現れた際にGP(Huisarts)に連絡する構図となった。
2020/3/17: 事業主が従業員に支払う賃金を補償する「自営業者のための臨時架け橋制度de Tijdelijke Overbruggingsregeling Zelfstandige Ondernemers (Tozo)」が創設。
2020/3/20: 老人ホームや小希望高齢者向け住宅は介護を必要としない利用者を対象に閉鎖。
オランダ国王が国民に向けてスピーチ「警戒心、連帯感、暖かさAlertheid, solidariteit en warmte」を強調
2020/3/23: 感染防御措置としてより厳粛な閣議決定が首相より発表。
公共空間では家族を除く3人以上の集団行動を禁止。1.5m以上の距離を保つ
キャンプ場、公園、ビーチなどは禁止措置が保たれない場合は閉鎖の方針。
また違反者には€390の罰金が科せられる様になった。
2020/4/6: コロナウイルス感染症の重症化リスクが高い患者に対して検査が義務化。
開業医、介護福祉士、障害者介護福祉士、在宅介護福祉士などの医療従事者が対象。
2020/4/7: COVID-19を受けた人が近くにいたかどうかを示すアプリが登場。
アプリはGPとの連絡もできる様な仕様だが追跡調査アプリで義務化には至らず
2020/4/10: オランダ国内での死者数が2500人を超える。
2020/4/21: 全国の児童保育・小学校を5月11日から再開することを閣議決定。
一方で9月1日まで全ての国内のイベントがキャンセルとなる。
入院登録患者は1万人超え、累計死者は4000人を超えた。
2020/4/26: オランダの毛皮農場でミンクからCOVID-19が検出される
2020/5/6: 5月11日から美容院や理容室などの「接触型の職種」の営業の再開を決定
6月1日よりバーの日中営業の再開を決定。
2020/5/19: 政府より6月1日(月)以降のロックダウン措置の緩和について発表
2020/5/30: 5月30日現在のオランダの累計感染者数は46,257名
累計入院者数11,727名、累計死者数5,951名
【オランダ国内の社会情勢】
(1)グループ
〇1.5m間隔を空ければ人々は屋外で集まることができる。(人数制限は撤廃された。)
〇一般の人々が入ることのできる全ての建物で、職員を含めず30人を上限として人々が集まることができる。その場合、1.5m間隔を空ける。(注:最大人数の100名、あるいは100名以上への拡大の可能性については、現時点では確定せず、6月中は最大30名まで可能というルールに基づき、実施してみて、その結果を踏まえて、拡大の是非を決定するとのこと。特に、教会での集会について、希望は多いが、教会の構造上、座席が1.5mの距離を維持しにくいこと、参加者が合唱等を行うことが想定されていること、容易にハグあるいは接触する雰囲気が醸成されることが想定されること、等を理由に、否定的な見解が示された。)
〇各家庭では、屋内、庭及びバルコニーで、来訪者と1.5mの間隔を空けることが強く要請される。
(2)飲食業は12時以降で営業
〇レストラン及びカフェは以下の条件の下に開業できる。
・客数は最大30人まで(職員を除く)。
・予約制とする。
・同一世帯の者以外は、皆1.5m間隔を空ける。
・店員と客は事前に来店によるリスクの有無について話し合う。
〇テラスの客数に上限は設けないが、客はみな着席し、(同一世帯の者以外は)1.5mの間隔を空けなければならない。
(3)教育
〇中・高等学校は6月2日(火)から再開する。学校は1.5m間隔を空けるための措置をとる。これは全ての生徒が同時に登校できないことを意味する。
〇小学校は、現在実施中の調査の結果により望ましくないとの判断が下されないかぎり、6月8日(月)から100%再開する。
〇校外託児所も同様に6月8日(月)から再開する。子供達は再び契約で決められた日に受け入れられることとなる。
(4)文化施設は12時以降で営業
〇映画館、劇場、コンサートホールは、以下の条件の下に再開できる。
・観客は最大30人。
・予約制とする。
・事前に来場によるリスクの有無について話し合う。
・皆が1.5mの間隔を空ける。
〇博物館及び文化遺産施設は、来訪者が事前にチケットを購入し、リスクの有無について事前の話し合いを行うのであれば、再開できる。来訪者数の上限は建物次第。1.5mの間隔を空ける。
〇音楽学校及び美術センターは、建物毎に30人を上限とし、1.5mの間隔を空けるのであれば、再開できる。
〇フェスティバルは、観客数の上限を30人とし、1.5m間隔を空けるのであれば、開催することができる。(注:大型のコンサート、イベント、スポーツ大会については、9月1日(火)以降の解禁には否定的な見解が示され、年内は難しいのではないか、とのコメントがあった。)
(5)公共交通機関
〇公共交通機関は必要な場合にのみ利用すること。
〇市電、(水上)バス、地下鉄及び電車では、6月1日(月)から、13歳以上の乗客に、非医療用マスクの着用を義務づける。駅構内及び停留所での着用は義務づけないが、1.5m間隔を空けること。
〇6月1日(月)以降、マスクを着用していない乗客には、95ユーロの罰金が科される。
(6)老人ホーム
現在、保健所(GGD)の管轄地域毎に一か所の老人ホームで、限定的かつ厳しい条件の下、来訪が許可されている。5月25日(月)からは、その措置をより多くの老人ホームに拡大する。6月15日(月)からは全ての老人ホームについてこの訪問規則が適用される見込みである。
【医療体制の現状】
(1) 医療機関へのアクセス
有症状の場合は原則自宅待機。70歳以上、体調不良の進行や呼吸困難、高熱(38℃以上)など医療ケアの必要性がある場合は家庭医(Huisarts)へまず電話連絡する。原則クリニックの来院は禁止。
医療機関への入院は原則家庭医からの紹介もしくは112通報による救急搬送を経て行う。
(2) COVID-19の検査状況
以前は家庭医の判断で症状発症から24時間以降経過した人を対象に家庭医クリニックもしくは保健所で検査が行われていた。
また、感染リスクの高い医療従事者や介護職員などは保健所で原則検査する方針とした。
6月1日よりCOVID-19の症状が一つ以上当てはまる人は誰でも保健所で検査が受けられる方針。
現在一日17,500件のペースでPCR検査が可能な状況とされている。
(3) 感染予防策について
市民への推奨予防策としては
① 石鹸と流水によるこまめな手洗い
② 咳やくしゃみは肘の内側で隠して飛沫を防止する
③ 紙のハンカチを使用する
④ 握手やハグの禁止
⑤ 人混みを避けて人との間隔を1.5m以上保つ
また、オランダ政府はマスクの着用は科学的根拠の不足から原則推奨していない。
例外は密閉空間である電車やトラム、バスなどを利用する公共交通機関のみマスクの着用を義務化した。
(4) 感染者への対応
① 医療機関・介護施設内の患者および医療従事者の場合:
症状寛解後24時間以上経過した後かつ、最低14日以上経つまでは隔離を行う。
② 自宅内の患者の場合:
症状寛解後24時間以上経過した後かつ、最低7日以上経つまでは隔離を行う。
(5)感染者の死亡時への対応
家庭医の許可の下でマスク着用など一定の措置を経れば自宅内でのお別れ・付き添いも可能。
【社会保障制度について】
オランダには日本のような国民向けの一律型給付金制度はないが、様々な政策により企業や国民に対して経済保障を行なっている。
① Noodmaatregel Overbrugging Werkgelegenheid (NOW)
(雇用主向けの臨時架け橋対策)
雇用主が従業員に継続して給与を支払うことができるようにするため、3ヶ月分の賃金費用を補償する制度。4月6日(月)に発効。最大90%の賃金費用を償還することが可能。
雇い主は申請後3ヶ月間は従業員向けの手当を貰うことが可能。
② Tijdelijke Overbruggingsregeling Zelfstandige Ondernemers (Tozo)
(個人雇用主・独立起業家向けの臨時架け橋対策)
コロナ危機で収入が社会的な最低限度を下回った場合、生活費を補填する制度。
収入と世帯に応じて最大で月額約1,500ユーロ(純額)までの給付型の所得支援。
更に企業向けの最大€10,157までの運転資金のための融資も開始。
返済期限の延長が可能な他、通常よりも低い金利での融資が可能。
③ Garantie Ondernemersfinanciering (GO-C)
(起業家向け融資保証スキーム)
国の保証により銀行から会社・企業家へ融資を促す制度。
1社あたり1.5~1.5億ユーロの間で最長6年間の融資で国が80%(大企業)、90%(中小企業)の金額を保証する。
その他にも外食産業向けの保障、農林水産業従事者への保障、所得税の一時的な税率引き下げや法人税の引き下げなど保障内容は多岐に渡る。
【オランダに在住して思うこと】
1月31日のWHO宣言から瞬く間に4ヶ月が過ぎましたが、感染予防策について他のヨーロッパ同様に国全体のロックダウンや罰金付きの外出制限やソーシャルディスタンスを設ける中でも、不要なマスク着用は頑なに拒否している点や、元々病院にすぐにかかる国民性ではないため家庭医の指示の下、病院への殺到を起こさず自宅待機を続ける点、状況に応じた様々な社会保障を早急に行う点など、COVID-19に対するオランダ国民や政府の反応から、一重にオランダの合理主義的な国民性を感じました。
個人的に面白かったのは、オランダ国内で合法となっているマリファナを取り扱うお店(通称「coffee shop」)がロックダウン発令時に数日だけ営業を延長許可されていた点です。
それによりマリファナを切らすまいとする人々が殺到してお店に長い行列ができました。これはロックダウンに伴うマリファナ販売禁止により、マリファナの不正取引の蔓延を防ぐための処置とされています。
また、オランダの首相が3月の記者会見で握手の禁止を発表した直後に司会者と握手してしまい笑いながら謝罪している様子や、オランダ国内でスーパーなどでのトイレットペーパーや食料品の買い占めがあった時は、買い占めをする人々を「ハムスター」と例えて(ハムスターが口に食料をありったけ頬張る様子から)自国民を皮肉る様子が、大らかで冗談好きのオランダの国民性を反映している気がしました。
オランダは6月より本格的な規制緩和に入ります。
既に外ではランニングや運河でボートを楽しむ人、公園で日光浴や道端のテラスで飲食を楽しむ人などいつもの日常が戻りつつあります。
日本でもいち早く緊急事態宣言が解除されていますが、早速クラスターが発生している地域もあります。
こちらも今後どのような状況になるかまだ不透明ですが、また変化や思うことがあればUpdateしていきたいと思います。
今回もお読みいただきありがとうございました。
【参考URL】
1. https://www.ad.nl/binnenland/het-coronavirus-was-al-veel-langer-in-nederland~af840f5b/?referrer=https://www.google.com/
2. file:///Users/takuyamada/Downloads/COVID-19_WebSite_rapport_dagelijks20200530_1021.pdf
3. https://www.rivm.nl/coronavirus-covid-19
4. https://www.rijksoverheid.nl/onderwerpen/coronavirus-financiele-regelingen
5. https://www.nl.emb-japan.go.jp/itprtop_ja/index.html
0 notes
Text
Lekker met Nederland! vol.3 (元Dr.コトーの蘭学手記)
English:italic
更新が1ヶ月遅くなり申し訳ございません。
言わずもがな、COVID-19(新型コロナウイルス )感染症で世界は混沌としているタイミングでのブログ更新となります。
ここオランダでも引き続き厳戒態勢が続いています(オランダの現在の状況についてはまた別途記事で書かせて頂きます)。
Here I update my third blog, even under the chaotic situation due to COVID-19 (corona virus) in the world. I will write about the quarantine in the Netherlands in another article.
今回のテーマは「オランダの家庭医」です!
The topic of this blog is about ‘General practitioner in the Netherlands’(‘Huisarts in Nederland’).
-そもそも家庭医とは?- What is General practitioner?
「家庭医」という言葉はまだあまり馴染みのない言葉だと思います。例えば、内科は体の各臓器にまつわる病気、小児科は子供の病気、外科は怪我や手術、など一般的には疾患の種類や体の部位、年齢や性別などで専門科目を分類します。
しかし家庭医の場合、ある地域やコミュニティの場において、年齢や性別は勿論のこと、疾患の種類やその有無に関わらず、健康についてのあらゆる相談に気軽に乗れる、持続的に患者(やその家族など)と関わりながら健康を支えていく、日々の「健康の相談役」です。勿論、相談だけではなく診察や検査、治療も行い、より専門性の高い検査や治療が必要な際は適切な専門医療機関への紹介や連携を行います。
言わば、地域住民が何か困ったらまず相談できる「かかりつけ」の医療専門家として家庭医は存在しています。私も日本では実はそんな一介の家庭医です。
I think the word "general practitioners (or family physicians)" is still not very familiar to some people. As a general practitioner, I explain their role.
For example, internal medicine is for diseases related to various organs of the body, pediatrics is for children's diseases, and surgery is for injuries and surgeries, etc. In general, specialties are classified according to the type of disease, part of the body, or age & gender.
In the case of a family physician, however, he or she is a daily "health consultant" who is available to consult with patients (and their families) about any kind of health issues, regardless of age, gender, or type of disease.
In addition to consultation, we also provide consultation, examination, and treatment, when more specialized examination or treatment is needed, they refer patients to an appropriate specialized medical institution. They are also in charge of home visits, terminal care. You can also consult with mental or even marriage issues as well.
In other words, general practitioners have a close bond with their patients as the first medical experts.
-オランダの家庭医-
General practitioners in the Netherlands
オランダでも「家庭医」本来の役割は日本と同様で地域の健康の相談役です。但し、こちらでは医療制度の関係上その社会的認知と役割は非常に重要となっています。
前回のブログでもお話しましたが、日本のように診療科を問わず開業医から市中病院や大学病院まで患者の希望で受診ができる「フリーアクセス」とは異なり、オランダの医療アクセスは全て自分の住む地域で登録された「家庭医(Huisarts)」を受診することから始まります。そしてオランダ国民(そしてオランダに在住する者)皆が、自宅から車で15分圏内の家庭医クリニック(Huisartsenpraktijk)に登録する義務があります。
家庭医は1人あたり2500-3500人程の地域住民を対象としており住民も家族単位で同じ家庭医を登録しています。オランダ国内には現在約7000人の家庭医がいます(国民総人口は1700万人)。
また、クリニックには医師の他に電話対応のオペレーター、ナース、プラクティスナース(医師の管理下で慢性疾患などを中心に独立して診察できる看護師)などがいます
家庭医の受診にかかる費用は既に国民が加入した基本医療保険(Blog vol.2参照)でカバーされるのでクリニックでの支払いは原則ありません。
このような家庭医制度の医療システムはヨーロッパでは他にデンマークやイギリスで同様に登録義務制、ドイツでは選択性の登録制となっております。
因みに家庭医になるためには日本と同様に大学医学部で6年間の医学教育の後医師免許を取得し、更に3年間の家庭医療専門医教育やその後の様々な生涯研修を終える必要があります(外国人医師がオランダで働く方法はまた別のブログでお話します)。
In the Netherlands, the role of the "general practitioners(GP)" is the same as in Japan, and they basically provide an advice on the health of the community.
However, its social recognition and role is very important due to the Dutch health care system.
As I mentioned in my previous blog, unlike "free access" in Japan, where patients can visit any department, from GP to city hospitals and university hospitals according to their wishes, all healthcare access in the Netherlands starts with a visit to a general practitioner (Huisarts) registered in the area where you live. And every Dutch citizen (and anyone living in the Netherlands) is obliged to register with a family GP’s clinic (Huisartsenpraktijk) within a 15-minute drive from their home.
Each GP serves about 2,500 to 3,500 local residents, and residents are registered with the same GP on a family basis. There are currently about 7000 GPs in the Netherlands (the total national population is 17 million).
In addition to physicians, the clinic also has a telephone operator, a nurse, and a practice nurse (a nurse who is under the supervision of a physician and who can see patients independently, especially those with chronic diseases).
The cost of visiting GP is covered by the basic medical insurance (see Blog vol.2), so in principle there is no charge at the clinic.
Other European medical systems such as that of Denmark or the United Kingdom have a mandatory registration system, while that of Germany has an elective registration system.
Incidentally, to become a GP, you need to obtain a medical license after 6 years of medical education at a university (department of medicine), followed by 3 years of education specialized in GP and various lifelong training after that (I'll talk about how foreign doctors work in the Netherlands in another blog).
-診療の流れ- Process of medical consultation
・患者は住民登録の時点で住所から担当となる家庭医に登録をします。
・基本的に予約診療制になっており、患者はクリニックに電話もしくはウェブサイトで診療予約を取ります。
・診療は平日の日中8:00-17:00の診療であることが多く、一日の平均患者人数は家庭医一人あたり大体30人前後になります。勿論、家庭医は全ての診療科について担当します。
(※平日時間外(夜間)や土日についての緊急受診はHuisartsenpostと呼ばれる時間外担当の家庭医が勤務する近隣の総合病院が診療を担当します。)
・家庭医から処方薬が出た場合は薬局(Apotheek)に行きます。この時も基本的には自宅住所から最寄りの薬局を家庭医が「かかりつけ薬局」として登録し、患者は登録された薬局で薬を処方してもらいます。

・専門診療科の受診は家庭医の紹介を得て市中病院の各科専門医へ連携します。専門医療機関へ紹介・診療中であっても家庭医は常に専門医と患者の情報共有を行います。
・患者の情報や検査結果については紹介状なども含め、全て電子データのみでのやり取りとなっており、家庭医にその情報の全てが集まります(国が管理する特殊なデータベースソフトを使用。スマートフォンのアプリなどで見ることもできます)。
1.Patients register with their GP from their address at the time of registration.
2.Patients can call the clinic or visit the website to make an appointment.
3.The average number of patients per day is about 30 per GP, and clinic hour is often from 8:00 a.m. to 5:00 p.m. on weekdays. Of course, the GP will be in charge of all medical departments.
(* For emergency consultations after hours on weekdays (at night) and on weekends, a special GP called’ Huisartsenpost’ will be in charge of the treatment at a nearby general hospital.)
4.Go to the pharmacy (Apotheek) if you have a prescription from your GP. Basically, GP registers the nearest pharmacy from the home address as the "family pharmacy", and the patient is asked to prescribe the medicine at the registered pharmacy.
If necessary, Patients will get a referral from a GP to a specialist in each department of the city hospital. GP will always share information about patients between specialists, even while referring to and treating a specialty medical institution.
All information on patients and test results, including referral letters, are exchanged only electronically, and all of the information is collected by GP (certain database software authorized by the government is used. They can also watch it on their mobile devices such as smartphone with app).
-家庭医の実際- My experience in GP clinic
前回のブログでも話しましたがこの度、実際に家庭医クリニックを訪問することができたのでそこでの感想を少しお伝えします!
今回見学したクリニックはオランダのフリスランド(Friesland)と呼ばれる北部の州にあるDrachtenという小さな町にあります。

写真:Leiden(筆者の住む街)とDrachten(クリニックのある町)
Photo: Leiden (the city where I live) and Drachten (the town where the clinic is located)
今回受けれて下さったWim Brunninkhuis医師は地元で30年近く家庭医をされておりFrieslandのBest doctorにも選ばれたことのある地域住民からの信頼も厚い大御所のドクターです。北部訛りのオランダ語と笑顔が印象的で、あとオランダ人らしく身長も非常に高い(2m!)方です。笑
診療スタイルですが、患者が部屋に入るや否や、Wim先生が握手やハグをしてまるで友人に会うかのような非常にフレンドリーな雰囲気で始まります。
どの患者も医師とは10年単位での長い付き合いため、先生から問診すると言うよりも患者のストーリー(受診に至るまでの話)をじっくり聞き、それに先生がコメントするような流れでした。患者もWim先生に信頼を置いているためか、全く緊張はしておらず寧ろ感情に素直で、気前よく話す人もいれば、途中で涙したり興奮する患者さんもいました。しかしながらそれぞれの患者のペースに合わせながら対話を続け、最後はまたお互い笑顔で握手やハグをして帰るという和やかな雰囲気が終始漂っていました。
午後はWim先生とともに訪問診療に同行し、認知症のある高齢者の方や怪我で足を痛め自宅療養中の患者さんなどの診療を行いました。その際も患者さんと目線の高さを合わせながら時に手を握るなど家族や友人のような接し方が印象的でした。
As I mentioned in previous blogs, I visited a GP's clinic, so I'll tell you a little bit about my impressions there!
The clinic is located in a small town called Drachten in a northern province called Friesland in the Netherlands.
Dr. Wim Brunninkhuis has been a GP in his hometown for nearly 30 years and has been voted the best doctor in Friesland. He always smiled, was so kind, and he is very tall (2m!) like a typical Dutchman.
In his practice, every time as soon as patients entered the room, he began to shake hands and gave hugs in a very friendly way, as if he were meeting a friend.
Every patient has a long relationship with the doctor for decades, so patients were not nervous at all, perhaps because they put their trust in Dr. Brunninkhuis. He also listened carefully to the patient's story (the reason that brought them to his consultation) and commented on it, rather than asking them as medical interviews.In his consultation, patientes were open to their emotions, and some of them spoke generously, while others cried or got upset in the middle. At the end of the day, each patient smiled, shook hands, gave hugs, and left.
In the afternoon, I accompanied on his home visits to treat elderly woman with dementia and a patient who stayed home due to injuries to his leg. I was impressed by the way he treated patients like family and friends at their home, sometimes holding their hands while keeping his eye level with them.

写真:Wim先生との一枚
Photo: author with Dr. Wim Brunninkhuis
-沖縄での経験との共通点-
Common characteristics between clinical experiences in Okinawa
今回の家庭医クリニックの見学を通して感じたのは、自分が離島で行なっていた診療の記憶の強いフラッシュバックでした。
オランダの家庭医が一つの地域で3000人前後を一人で担当するように、振り返れば私も2年間、沖縄の八重山諸島にある小浜島(人口約700人)で一人医師(Dr.コトー)として診療所で働かせてもらいました。
その時に経験した島民の皆さんと同じ島で暮らし、同じ行事で喜怒哀楽を共有し、診察室やご自宅でじっくり話を聞きながら診療した非常に緊密な距離感をふと思い出し、訪問診療で長身のWim先生がしゃがみながらベッド脇に座る認知症のおばあちゃんに冗談を交えながら笑顔で語りかけているシーンでは思わず、自分が島で診ていた認知症のオバァ(おばあちゃん)と話す瞬間と重なり、何とも言えない既視感を抱きました。
オランダの家庭医と沖縄の離島診療・・国や人種や文化、そして医療制度も全く異なりますが、一つの地域で同じ住民を見守り、気軽に何でも相談できるような深い信頼関係があるという点では見事に両者は一致しており、何か「医療」の本質のようなものを感じることができました。
What I felt throughout my visit to the GP clinic was a strong flashback to my own experiences of the clinic on a remote island.
I used to work as a lone doctor in a clinic on Kohama Island (with population about 700 people) in the Yaeyama Islands of Okinawa for two years, just as a Dutch family doctor is in charge of about 3,000 people in one area by himself.
In the scene where Dr. Brunninkhuis was talking to an old lady with dementia with a smile and a joke while squatting down and sitting by the bedside, it overlapped in my mind with the moment I was talking to an old lady with dementia on the island, just like “déjà vu”.
General practitioner in the Netherlands and the remote island doctor in Okinawa... The country, race, culture, and medical system are completely different from each other, but there is a deep relationship in terms of a close bond and trust between local people, and a clinical style to look after the same residents in one area with casual consult.
I felt something “fundamental” in medicine, from this similarity.

写真:小浜診療所勤務の頃(看護師さんと事務さんと一緒に)
Photo: the period when I worked in Kohama island, with my nurse and clerk.
もう一つ、Wim先生と話したオランダの家庭医診療の特徴として、「患者さんの健康をどのように捉えるか」という視点が挙がりました。
今までの「健康」の考え方といえば、病気や怪我にならないことであったり、医療者から言われて「皆が目指すべき状態」ということで治療の目標だったりしました。
しかしその「健康」の定義自体をもっと患者本位で一緒に考えよう、という考えがあるオランダ人家庭医から始まり、この健康に対する新しい捉え方は「ポジティブヘルス(positieve gezondheid)」と名付けられ、後にオランダ中の家庭医に広がりました。
さて、日本でも最近では少しずつ名が知られてきたこの「ポジティブヘルス」について、次回のブログで詳しく述べたいと思います。
Another characteristic of GP in the Netherlands that I discussed with Dr. Brunninkhuis was a perspective of "how we view the patient's health".
Usually, the idea of "health" has been often regarded as “neither sickness nor injury”, but one Dutch GP started to claim that health should be defined in more patient-centered way.
This new view of health was named "positive health" (positieve gezondheid) and later spread to many GP throughout this country.
I'll talk more about the "positive health" in my next blog.
今回も皆さん、最後までお読み頂きありがとうございました。
Thank you for your reading all !
-School life in Leiden-
I will report it in the blog of “quarantine time”. Lol
-Today’s Dutch Lesson-
‘Lekker’
This word has actually lots of meanings. The most used meaning is “delicious/tasty” in English, or “美味しい” in Japanese, but you can also use it for “pleasant feeling” or “comfortableness”, or “気持ちいい/快適な” in Japanese.
Example (1):

Nederland: De Nederlandse pannenkoeken is heel lekker!
English: The Dutch pancake is very tasty!
日本語:オランダのパンケーキはとても美味しい!
Example (2)

Nederland: Het is vandaag lekker weertje!
English: It is (sunny) warm weather today!
日本語:今日は天気がいい(日が当たって暖かい)!
There are too many kind of cases for using “Lekker” according to situations in Dutch, but it reflects how Dutch people love this word at the same time.
The title of my blog is “Lekker met Nederland” and it comes from the title of the Dutch song called “Lekker met meiden”, which means “something typical(familiar) to woman”.
I like the flexibility of “Lekker” and I put the word in the title with a wish of introducing something fun about the Netherlands in my blog.
When you travel to the Netherlands, why don’t you use “lekker” for good foods, or good mood, then people would reply to you with saying “Ja, lekker!”
0 notes
Text
Lekker met Nederland! vol.2 (元Dr.コトーの蘭学手記)
Goedavond! 皆さんこんにちは!
ここオランダの冬も本格的になり最近も日中の気温も5℃を切るような日々が続いていました。雪はありませんが長年沖縄で暮らしていたせいか寒さがすごく身体に染みます。 Here in the Netherlands it is getting colder and colder, especially for me and it makes me miss the sunshine of Okinawa, the place where I used to live with tropical climate.
ブログ第2回目の今回は「オランダの医療制度」について少しお話をしたいと思います。正直ちょっと複雑で分かりにくいかもしれませんがどうぞお付き合い下さい。
後半にはオランダでの学生生活についてツラツラと述べたいと思います。正直ただの日記ですが、色々な人に読んでもらいたいのでオランダの生活については敢えて英語で書こうと思います。「はー、英語かよ!」と思った方はすみません。でもGoogle翻訳などでコピペで気軽に翻訳できる時代なのでご容赦ください。
そして今回からブログの最後にオランダ語ミニレッスンを入れることにしました!せっかくオランダ語を勉強しているので少しでも皆さんの豆知識になれば嬉しいです!
First, I explain the Dutch medical system in Japanese, which is a bit complicated and confusing, but later I report my school life here with a short Dutch lesson! So here we go!
-オランダの医療保険-
オランダの医療保険制度は日本と同様に国民皆保険制度で民間保険会社が国の規制を受けて定められた水準の保険を提供しています。しかしその種類は多岐にわたりかつ複雑です。
まず保険法の種類だけでも長期ケア法(WLZ: Wet langdurige zorg)、健康保険法(ZVW: Zorgverzekeringswet)、青少年法(JW:Jeugdwet)、社会支援法(WMO: Wet maatschappelijke ondersteuning)などがありますが、非常に細かい話になるので今回はそのうちで主な二本柱の保険となるのが長期ケア(WLZ)と健康保険(ZVW)の話をしたいと思います。

WLZは強制保険の一つで入院治療などで24時間ケアが必要とされている人が対象で国が直接保険者となります。実際は要介護度の高い高齢者や障害者が対象になることが多く、高齢化に伴い利用者が増加し、医療費の60%ほどを占めるようになっています。
(因みに高齢化について、オランダでは65歳以上の高齢化率は2017年現在で18.5%で2035年には26%に達すると言われており既に国が危機感を持ち年金受給年齢の段階的引き上げなどを始めています。日本と言えば、2017年時点で高齢化率は27.7%と既にオランダよりも20年先に高齢化が進んでいます。。)
一方でZVWはいわゆる基本医療保険となります。同じく強制保険ですが民間保険会社が保険者となります。保険による保障範囲は国の規制範囲内で保険会社と医療提供者(病院や医師)が交渉することで決めます。なのでそこでサービスの価格と品質について国の管理下で会社間での競争が生じます。また病院や医師(主に家庭医)��保険会社と保険範囲について度々交渉する必要があります。いかにもディスカッションが大好きなオランダ人らしい制度だと思います。
基本保険料は誰に対しても保険会社に関わらず年間約€1300(毎月€110)前後ほどで一定となります。また予め医療費について年間の自己負担額(Eigen risico)を設定することもでき、自己負担額を高く設定するほど毎月の支払い保険料が安く抑えられたり保険の選択種類が増えたりします。自己負担また実際にかかる医療費は全て保険会社で支払われ、後から被保険者へ請求されます。なので基本的に病院受診や薬局での処方薬に対する患者のその場での実質負担額はありません。
一方で保険サービスとしての財源ではリスク均等化基金という形で被保険者からの基本保険料と、被保険者の雇用主から支払われる給与税(所得に応じる)、国税を受け取りながら、それを被保険者の年齢、性別、基礎疾患の有無などリスクプロフィールに応じて保険者である保険会社が調整額を受け取るという流れのようです。
先に挙げた保険法以外にも、更に各民間保険会社が定めた補完保険(Aanvullende verzekering)と呼ばれる任意保険もあり、保険会社が強制保険のZVWと一緒にサービスを提供していることもあります。オランダ国民の84%ほどが補完保険に加入しており、通常の医療保険ではカバーされない歯科矯正や代替医療、メガネ・コンタクトの処方、理学療法などを保障しています。例えば欧米では歯科矯正は非常にpopularなのである意味オランダ人にも必須なのかもしれません。
その他にもオランダでは18歳未満での医療費は親の保険でカバーされるので実質無料のほか、自己負担金制度により年ごとに定められた控除額(2020年は€385)を超えた医療費が全て患者へ自動的に返還されます。つまり手術や化学療法や放射線治療、不妊治療など高額医療についても特別な請求手続きは必要ないことになります。
以上がざっとですがオランダの医療制度についてでした。
同じ国民皆保険制度の日本と比べてみると、日本では全員が公的医療保険に加入することになっており保険者は国民健康保険や全国健保協会、共済組合などが担当し、民間保険会社はあくまで任意保険のみ状態となっています。
また、保険診療の範囲も健康保険法に基づくためオランダのように保険者と医療者(病院、医師)が直接交渉することもありません。一方で被保険者の医療費の実質負担額も未就学児や75歳未満の高齢者を除けば医療費の3割負担であるものの病院でも薬局でも患者のお金の支払いはありますね。オランダは受診後の窓口や薬局支払いがないのが羨ましい。。
とは言え、日本では国民皆保険の下で医療機関を自由に選べ(フリーアクセス)、少ない自己負担額で高度な医療を受けられますよね。
オランダでは医療機関の受診は基本的にフリーアクセスではなく、登録されたその地域の指定医=家庭医(Huisarts)の受診がまず必須となります。因みに私の医師としての専門領域も家庭医療なので個人的にも業務内容が気になります。
ということで、オランダの家庭医のクリニックに実はこの前見学に行ってきました。本当はその話もする予定でしたが思いの外、保険の話が長くなったので次回はオランダの家庭医の仕事について少しお話ししたいと思います。
-School life in Leiden-
As I reported in the previous blog, I am currently studying Dutch at Leiden university. It is located in the old city of Leiden ,and surrounded by beautiful canal(photo). The university is really open for international students and lots of students from all over the world come to study here every year.

In my class, there are less than 20 people but full of diversity of national background. We are such a good company and sometimes hang out together (photo). Lectures in university are very interactive compared with those in Japan, and the relationship between students and teachers also seems to be closer, so I feel just comfortable for asking any question to my teachers during lectures. About exams, since they are in either Dutch ore English, I sometimes feel even more difficult than some exams I took when I was a medical student, still I love all the subjects I had in the first semester; Dutch language(text, grammer, listening, speaking), Dutch painting, and Dutch debate. I would like to tell you the details of each class next time!

Besides my studying, I am also participating as a volunteer in speaking class of Japan Studies course, the course for Dutch students who study Japanese language and culture. I got to know many Dutch friends there and they are all nice people, and just made my day every time! We started Japanese-Dutch cultural exchange club activity (Kaiwa club) among Dutch students and Japanese students, and sometimes have fun events such as introduction of Japanese culture or potluck too(photo).

-Today’s Dutch Lesson-
“Gezellig“
According to dictionary, it means “enjoyable” or “cozy” in English, or “居心地の良い” in Japanese, but many of my Dutch friends say there is no exact translation for this term. In my impression, “gezellig” is the certain moment or atmosphere with full of warmness, joy and fun with people. It does not mean that we just do something together like hang out or drink, but that we are covered with “comfortable mood”.
It is one of the most important concepts for Dutch people to cherish in their lives. Even in medical field, some general practitioners (huisarts) are taking account of “gezellig” time for patient life when they make plans for management.
In addition, I also found that “Gezellig” is very similar to “ユンタク(Untaku)” one of the traditional cultures of Okinawa. It also means the certain time with relax, joy and fun with people.
If you go to the Netherlands, you may hear “Gezellig” in many occasions and you will understand completely what it means, because this feeling of “gezellig” can be everywhere in your life!


That’s all today, tot ziens!
1 note
·
View note
Text
Lekker met Nederland! vol.1 (元Dr.コトーの蘭学手記)
Goedemorgen!
皆さん、突然ですが「オランダ」と聞くとまず何を思い浮かべるでしょうか?
風車とチューリップ畑が広がる優雅な田園風景、中世から続く運河と街が一体化した歴史的街並、チーズや牛乳などの酪農、世界一平均身長が高い国、レンブラントやフェルメール、ゴッホといった芸術、もしくは違う視点で考えると合法ドラッグや合法売春(飾り窓)などの寛容性、そして安楽死…今挙げたものは確かに全てオランダを現す「一部」です。
この手記ではオランダでの暮らしを通して日本人、そして医師としての私の「視点」で感じた、或いは学んだ事をリアルな声として皆さんにお届けしていきたいと思います。
オランダの話をする前にまず私の経歴を端的にお話しします。私(山田 拓)は神奈川県出身で沖縄県の琉球大学医学部を卒業後、県内での初期臨床研修及び専攻医研修を得て2017年4月から2019年3月までの2年間を沖縄県八重山諸島中央に位置する小浜島(人口700人程度)の離島の診療所にて「一人医師(Dr.コトー)」として勤務しておりました。その後関東での一時勤務を経て家庭医療専門医を取得、2019年8月よりオランダのライデン大学に在籍しております(私がオランダへ来た理由は後程、詳しくお話し致します)。
オランダの概要ですが、ヨーロッパ北西部に位置する人口約1700万人、九州全土程の面積を有する国です。公用語はオランダ語ですが国民の殆どが英語を理解し、話すことができます。またオランダの国民は総人口の約80%がゲルマン系オランダ人、その他トルコ人、モロッコ人、スリナム人などがそれぞれ総人口の2%近くを占める多民族国家です。歴史的にはライン川を始めとしたヨーロッパの主要河川が合流する地理性から古くよりヨーロッパの貿易・商業の拠点として栄え、17世紀の大航海時代には南アフリカ、スリナム、インドネシアと植民地を広げ当時の世界の覇権の一端を担いました。また日本とは江戸幕府の鎖国政策下において長崎出島を通じて貿易を行い、西洋文明(所謂「蘭学」)を伝えた非常に所縁のある国であります。
私の暮らすライデン(Leiden)は19世紀始めに日本に西洋医学を広めたシーボルト博士が滞在していた街ということもあり、街中にはシーボルト博物館(Japanmuseum SieboldHuis)や日本庭園を有する植物園(Hortus botanicus Leiden)などの名所があります。そんなライデンで現在、私は学部生としてオランダ語とオランダ文化を学んでいます。
私とオランダとの出逢いは私が小浜島の診療所で医師をしていた頃に遡ります。当時離島でのがん患者さんの看取り診療や身体的には健康でも生きることに悩む患者さんとの診療を通して健康とは何か、医師の役割とは何か、そしてより良い死と何か、とこれまでになく強く自問自答するようになりました。今の日本の現状と言えば、総人口に占める高齢化率が28.4%(2019年9月現在)と3人に1人の割合で進む一方で、毎年の自殺者も2万人を超える(特に未成年で増加傾向)という状況です。誰もが「健康」そして「死」を意識する時代となった中で既存の健康観や生死の価値観で果たして我々はずっと幸せに暮らせるのか、新しい視点での健康観や死生観もあってもいいのではないかと考えていた最中、偶々読んだ本や参加した講演会からオランダの安楽死制度(英/蘭:Euthanasia)やポジティヴ ヘルス(英:Positive Health, 蘭: Positie Gezondheid)を知る機会を得ました。また後の手記で詳しく解説しますが、オランダは世界に先駆けて安楽死制度を合法化しました。今ではオランダでは年間6000人以上が「安楽死」を選んで亡くなっています。またPositive Healthはオランダ発の新しい健康観で健康を様々なバロメータから捉え、自分自身で決めていく手法でオランダの家庭医の中で徐々に広まっているコンセプトです。いずれも私にとっては真新しい考えでありかつ、先述した自分の診療上の疑問と非常にリンクしており、オランダの医療について強く興味を抱くようになりました。また、同時にこのようなユニークな制度や価値観が生まれるオランダの国民性とその文化にも関心を持つようになり、離島診療の任期が終わる過渡期に際し、新しい知見を求めるべく満を辞してオランダ行きを決意しました。
次回以降の手記ではそんな決意の下、飛び立ったオランダでの生活、学生としての生活、そして医療・福祉制度などについて私の感じたまま、少しずつお話ししたいと思います。
Tot volgende keer! (また次回にお会いしましょう!)


5 notes
·
View notes