
Last Seen Blogs





Text
Working towards developing our community.
For the past weeks, working in the vibrant yet challenging community of Kenville has been a journey of profound discovery and transformation. The bustling streets, rich with stories, stand as a testament to the perseverance and struggles of the community members. Working on this blog, I have realised the importance of sustainable development goals and how they can bring hope and progress to communities. Sustainable development is not just a global agenda; it is a lifeline for communities striving to break the cycle of poverty and inequality (Mahlatsi, 2021).
Nelson Mandela's words, "It always seems impossible until it is done," and Chantal Christopher's, "We cannot do everything at once for our communities, just try to tackle the web," resonate deeply as I witness the everyday challenges faced by Kenville residents—limited access to clean water, inadequate healthcare facilities, and economic instability. Despite these challenges, there is potential for impactful change driven by sustainable development principles.
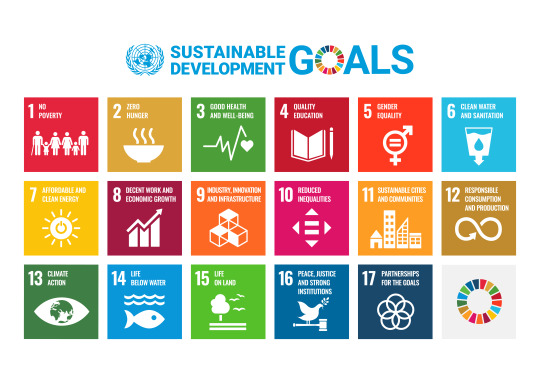
(17 SDGs | ClimatePartner, n.d.)
The World Health Organization (2021) defines health as "a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity." This implies that mental health is more than just the absence of mental disorders. In Kenville, health disparities are stark due to limited access to health care, high rates of communicable diseases, and inadequate nutrition (De Villiers, 2021). Poor living conditions exacerbate these issues. As an occupational therapy (OT) student, I work towards universal health coverage by providing comprehensive information during health promotions about OT services, offering preventative care, mental health support, and chronic condition management. Collaborating with nurses ensures timely and appropriate healthcare interventions. Addressing health inequalities is crucial for improving health outcomes.
Education is a cornerstone of national progress. An educated population drives innovation, economic growth, and social cohesion. Educated individuals are better equipped to make informed health decisions, improving overall community health (Hahn & Truman, 2015). In Kenville, overcrowded classrooms, limited resources, and teacher burnout hinder education. To facilitate quality education, I work with local schools to develop inclusive strategies for learners with learning difficulties and literacy gaps, providing learning materials for home use. These programs offer educational support and life skills training.
Unemployment and underemployment are rampant in Kenville, limiting economic stability and growth. Prof. Alfred Ramukumba notes the impact of unemployment on South Africans: "The inner world of the majority of the population in South Africa is clouded by poverty and poor socioeconomic conditions, and income generation is viewed as a priority" (Monareng et al., 2018). As a student OT, I facilitate vocational training programs and small business development initiatives, such as making doughnuts and amagwinya. Supporting local entrepreneurs through workshops on financial literacy and business management increases self-employment, improving local economic growth and stability.
South Africa has made strides towards gender equality, but challenges remain. Policies like South Africa's National Policy Framework for Women's Empowerment and Gender Equality aim to ensure equal rights and opportunities for all. However, in Kenville, women and girls often face socioeconomic inequalities due to gender-based violence, discrimination, and cultural stereotypes, limiting their access to education, employment, and healthcare. As a community-based student therapist, my role extends beyond clinical interventions. I work with the youth to build their voices within the community and with individuals to address trauma and develop skills. Creating an environment where women and girls can thrive helps break the cycle of poverty and inequality.
South Africa's history of apartheid, a system of racial segregation, neglected environmental issues. Policies from that era lacked environmental inclusiveness, failing to promote sustainable community development (Vyas-Doorgapersad, 2023). Kenville faces poor housing and sanitation due to inadequate service delivery. Addressing SDG 11 for safe housing involves working closely with the community to implement home adaptations for individuals with disabilities and adapting classrooms for children struggling with schoolwork.
Understanding the social determinants of health and adopting a holistic approach to care has transformed my practice, making me a more empathetic and effective occupational therapist. We can make meaningful progress by listening to the community, understanding their needs, and co-creating sustainable, culturally relevant solutions.
The principles of sustainable development provide a framework for addressing Kenville's challenges. Applying these principles highlights our world's interconnectedness and shows how local actions can contribute to global goals. By standing up for what is right, pushing for policies prioritising marginalised communities, and ensuring their voices are heard, we can drive sustainable development and improve lives in Kenville.
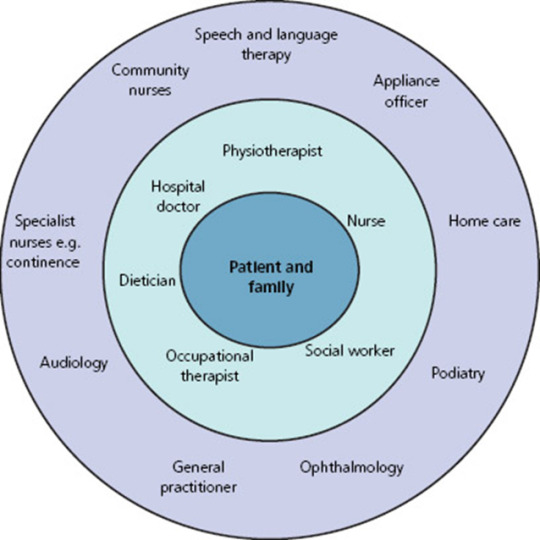
The diagram below shows how environmental, social, and economic factors contribute to community sustainability. Each of the factors aligns with one of the 17 SGDs.

Żak (2015)
References
17 SDGs | ClimatePartner. (n.d.). ClimatePartner. https://www.climatepartner.com/en/knowledge/glossary/sustainable-development-goals-sdgs
De Villiers, K. (2021). Bridging the health inequality gap: an examination of South Africa’s social innovation in health landscape. Infectious Diseases of Poverty, 10(1). https://doi.org/10.1186/s40249-021-00804-9
Hahn, R. A., & Truman, B. I. (2015). Education improves public health and promotes health equity. International Journal of Health Services, 45(4), 657–678. https://doi.org/10.1177/0020731415585986
Mahlatsi, K. M. (2021). Achieving Sustainable Development Goals (SDGs) in Africa. UJ Press Journals, 86, 2.
Monareng, L. L., Franzsen, D., & Van Biljon, H. (2018b). A survey of occupational therapists’ involvement in facilitating self-employment for people with disabilities. South African Journal of Occupational Therapy, 48(3). https://doi.org/10.17159/2310-3833/2017/vol48n3a8
Vyas-Doorgapersad, S. (2023). Assesinng Sustainable Development Goal 11 in South African context. Journal of Economic Development, Environment and People, 12(4), 42–54. https://doi.org/10.26458/jedep.v12i4.817
World Health Organisation. (2021). Health and well being. WHO. https://www.who.int/data/gho/data/major-themes/health-and-well-being#:~:text=The%20WHO%20constitution%20states%3A%20%22Health,of%20mental%20disorders%20or%20disabilities.
Żak, A. (2015). Triple bottom line concept in theory and practice. Prace Naukowe Uniwersytetu Ekonomicznego We Wrocławiu, 387. https://doi.org/10.15611/pn.2015.387.21
0 notes
Text
Community-based OT practice through the lens of UKZN.
Community practice opens doors for the profession of occupational therapy to grow and to apply occupation in its natural settings. Yet communities are complex and dynamic; addressing health issues in communities is complicated by factors such as reimbursement, community-defined needs and health disparities. The current healthcare systems lack the ability to adequately address community health issues, health disparities, health promotion and health behaviours, which lays the groundwork for occupational therapists to actively explore and define roles in community practice (Hocking, 2011). Because of this the OTs have no recipe for success in this realm of practice, no standard time to perform activities of daily living treatment sessions. Therefore, we need to adopt a client-centred community approach that requires practitioners to have the skills to work effectively with individuals and groups and restore community interactions, as well as prevention and health maintenance programs that enhance function and well-being. To be the crème de le crème needed in community practice, one needs to have a journey with UKZN.
Occupational Therapy is a hands-on profession that ensures professional-specific knowledge and skills are achieved (Ndaba et al., 2023). Hence, fieldwork commences in the first year to expose the students to a supervised fieldwork practical where they make contact with patients for the first time and get a general idea of what fieldwork entails. This is when students are exposed to different communities within KZN to learn about the programs that run in communities, the socio-economic status, and the quality of healthcare that affects the communities. The module is not OT-related as it doesn’t indicate the OT role. Specifically, this is a challenge with the OT curriculum because most students in their first year don’t understand the occupational therapist roles generally; therefore, understanding it within a community context during those times makes it even harder. Due to this, the fundamentals of being a community-based OT are lost.
It was observed by Hammell (2015) that the most influential theories and models informing the international occupational therapy profession have been formulated by theorists who all reside in the Western/Northern world. These models include the PEO, KAWA, MOHO, etc., which are taught from the second year and are based on understanding our clients, making it easier to down our intervention. The early introduction of these theories narrows our intervention to be client-specific, resulting in well-being for our client. The use of models such as the ecological system is introduced in the third year; however, due to limited exposure to communities, it is not used.
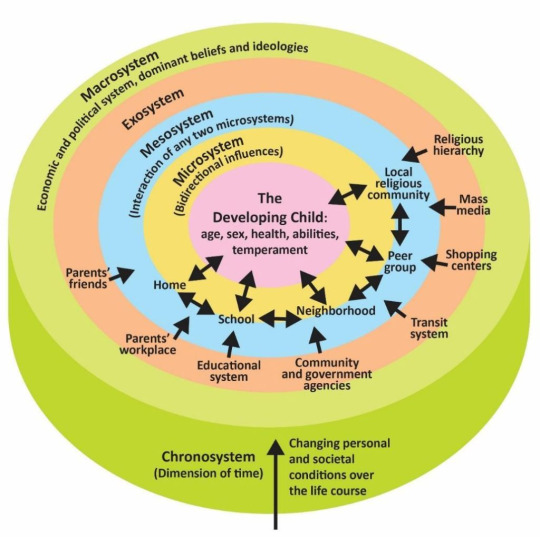
Giovannini, J. (2023, May 23). Bioecological Systems Theory. Pressbooks. https://rotel.pressbooks.pub/children-families-schools-communities/chapter/bioecological-systems-theory/
Though Western theories guide our profession, the presentation of the content and cases discussed on the theories are made to be South African suited; this is inspiring and promotes a vision and an aspiration towards a more culturally inclusive and globally relevant profession. It is a profession that addresses the occupational rights of diverse people in different communities, not solely those experiencing ill health in the privileged corners of the country. Even though, as students, we are taught this way, the assessment forms we used on our clients in communities are Westernised, making it challenging to assess them within that setting as most assessments are standardized.
The curriculum of UKZN is structured in the sense that in the second and third years, each semester focuses on one component of an OT, whether psychosocial or physical (University of KwaZulu-Natal, 2024). This narrows the scope of OT within the communities to only viewing our clients using the medical model. Being a community-based OT is not only practice-based but includes being able to advocate for clients, assessment skills, capacity-building skills and applying principles of occupation in a community context. Students are placed in an acute hospital or non-governmental organization setting during these times to foster learning (Naidoo et al., 2017). This limits students' ability to think critically when working in communities because they are exposed to seeing clients with particular presentations at a time.

Picture of me, working with a group of girls during a expressive group
In conclusion, the UKZN Occupational Therapy (OT) curriculum provides a robust foundation for preparing students to engage in community practice, emphasizing hands-on experience and early exposure to diverse communities. However, the complexity of community health, coupled with systemic health disparities and the reliance on Western theories and standardized assessments, poses significant challenges. While the curriculum's structure fosters a deep understanding of various OT components and client-centred care, it tends to limit the holistic, advocacy-based approach essential for effective community practice. To truly excel in community settings, students must navigate these complexities and develop a versatile skill set that extends beyond the traditional medical model, embracing cultural inclusivity and the unique dynamics of community health. This journey at UKZN, with its strengths and areas for growth, ultimately aims to equip future occupational therapists with the competence and adaptability needed to make a meaningful impact in diverse community contexts.
References
Giovannini, J. (2023, May 23). Bioecological Systems Theory. Pressbooks. https://rotel.pressbooks.pub/children-families-schools-communities/chapter/bioecological-systems-theory/
Hammell, K. W. (2015). Respecting global wisdom: Enhancing the cultural relevance of occupational therapy’s theoretical base. the British Journal of Occupational Therapy/British Journal of Occupational Therapy, 78(11), 718–721. https://doi.org/10.1177/0308022614564170
Hocking, C. (2011). Public Health and Health Promotion. Occupation Analysis in Practice, 246–263. https://doi.org/10.1002/9781118786604.ch17
Naidoo, D., Van Wyk, J., & Waggie, F. (2017). Occupational therapy graduates’ reflections on their ability to cope with primary healthcare and rural practice during community service. South African Journal of Occupational Therapy, 47(3). https://doi.org/10.17159/2310-3833/2017/v47n3a7
Ndaba, N., Naidoo, D., Govender, P., Van Heerden, N., Heaver, J., Rambhuron, S., Khan, F., Shandu, B., & Ndlovu, S. (2023). Experiences of online occupational therapy education during the COVID-19 pandemic at a South African university. South African Journal of Occupational Therapy, 53(2), 55–63. https://doi.org/10.17159/2310-3833/2023/vol53n2a6
University of KwaZulu-Natal. Hands-On Opportunities -Discipline of Occupational Therapy [Internet]. 2024. Available from: https://ot.ukzn.ac.za/hands-onopportunities
0 notes
Text
Title: Mistakes of the past can be corrected today.
Being a mother is one of the most rewarding experiences a woman can have; however, it comes with a troll of physical and emotional demands. Mothers, babies, and children in poor families are at increased risk of illness and face many challenges in accessing timely, high-quality care. This has contributed to poor use of health care facilities by patients, lack of transport, sub-optimal quality of care by some health providers and social inequalities.
For instance, 46% of pregnancies within the low range occur in female-headed households. Overall, around half (53%) of the pregnant women are single, 26% married and 19% cohabiting. Although teen pregnancy rates are falling, 14% of pregnant women are teenagers aged 10-19 years (Black et al., 2016) In communities, women live in such circumstances, making them vulnerable to society's demands. The spread of poverty and unemployment in communities compromises the lives of these families as they are exposed to a lack of good quality services, lack of education, substance abuse, violence, and HIV/ AIDS. As these factors are controlling the streets of our communities, the rates of postpartum depression in women of South Africa range from 21% to 50% (Pellowski et al., 2019). Most mothers in communities are unaware of such. However, it is seen through their occupation choices, for example, abusing substances, not attending clinic appointments, and being poorly responsive to their infant's needs, which often retards infant growth, resulting in behavioural problems and reducing cognitive functioning (Katzen et al., 2020).

(“Using a Community-Based Approach to Improve Maternal and Child Health,” 2023)
Maternal health influences the well-being of both mother and child during pregnancy, birth, and postpartum periods, reducing the risks of complications and mortality for both. Having healthy children in the community ensures a productive and sustainable society. Hence, investing in maternal and child health leads long-term benefits, including improved educational system, reduced poverty, and improved socio-economic status of the families (Mudiyanselage et al., 2024b) . The attached picture brings emphasize on how maternal and child health is a life time journey.
Maternal health is an emerging area within the field of OT. Our main aim for interventions and strategies is to PROMOTE the occupational well-being of all domains related to maternal health (Merkel et al., 2023). An estimated 39% of the world's children under the age of 5 years have not attained their developmental potential (Black et al., 2016). In communities, we find that children are not reaching their potential, and due to the lack of knowledge and neglect, the mothers are unaware of that situation; this is also influenced by the curriculum installed in the creches within the community. As a community-based OT, we must facilitate these milestones so that the children can reach their potential implementing sensory integration techniques, facilitating play-based activities. This is closely tied to developing parenting skills as we also give parents home programs that they could use. While in the community, I have seen that most of the children we see at the clinic, creche and primary school, lack sensory stimulation which affect their engagement in play and education working on these have been the key goal, however, in Kenville, there are other factors which are affected for example, overcrowding in schools, family matters, lack of infrastructure and lack of quality health care such factors allowing us to wear our big boots of advocacy.
Mothers and children from disadvantaged economic, social, and psychological backgrounds face more significant health burdens than those from non-disadvantaged communities as disadvantaged mothers are prone to have higher financial burdens, rates of smoking, alcohol use, young pregnancies, live in remote areas and other poor living situations Like their parents, children raised in a disadvantaged community tend to have increased risks of poor health, low educational attainment and begin their adult life as disadvantaged (Mudiyanselage et al., 2024). As much as this is evident by the community of Kenville, I believe that with more awareness and willingness to work with the community than to work in the community will better insight to the services provided by us as occupational therapist in maternal and child health as means to improve the burden to improve their mother and child's well being. As it is only a human right but the foundation of many communities, including Kenville.
References
Black, R., Laxminarayan, R., Temmerman, M., & Walker, N. (2016a). Disease Control Priorities, third edition (Volume 2): Reproductive, Maternal, Newborn, and Child Health. World Bank Publications.
Black, R., Laxminarayan, R., Temmerman, M., & Walker, N. (2016b). Disease Control Priorities, third edition (Volume 2): Reproductive, Maternal, Newborn, and Child Health. World Bank Publications.
Cobigo, V., Martin, L., & Mcheimech, R. (2016). Understanding community. Canadian Journal of Disability Studies, 5(4), 181. https://doi.org/10.15353/cjds.v5i4.318
Corlyon, J., & McGuire, C. H. (1997). Young parents in public care: Pregnancy and Parenthood Among Youg People Looked After by Local Authorites : Report of Component 1 of Preparation and Support of Parenthood.
Katzen, L. S., Tomlinson, M., Christodoulou, J., Laurenzi, C., Roux, I. L., Baker, V., Mbewu, N., Roux, K. W. L., & Rotheram, M. J. (2020). Home visits by community health workers in rural South Africa have a limited, but important impact on maternal and child health in the first two years of life. BMC Health Services Research, 20(1). https://doi.org/10.1186/s12913-020-05436-7
Mabaso, M. H., Ndaba, T., & Mkhize-Kwitshana, Z. L. (2014). Overview of Maternal, Neonatal and Child Deaths in South Africa: Challenges, Opportunities, Progress and Future Prospects. International journal of MCH and AIDS, 2(2), 182–189.
Merkel, T., Goodman, D., Novalis, S., Beck, M. J., Medva, A., & Wintermantel, F. (2023). Role of OT in maternal health. the American Journal of Occupational Therapy, 77(Supplement_2), 7711505061p1. https://doi.org/10.5014/ajot.2023.77s2-po61
Mudiyanselage, S. B., Dona, S. W. A., Angeles, M. R., Majmudar, I., Marembo, M., Tan, E. J., Price, A., Watts, J. J., Gold, L., & Abimanyi-Ochom, J. (2024a). The impact of maternal health on child’s health outcomes during the first five years of child’s life in countries with health systems similar to Australia: A systematic review. PloS One, 19(3), e0295295. https://doi.org/10.1371/journal.pone.0295295
Mudiyanselage, S. B., Dona, S. W. A., Angeles, M. R., Majmudar, I., Marembo, M., Tan, E. J., Price, A., Watts, J. J., Gold, L., & Abimanyi-Ochom, J. (2024b). The impact of maternal health on child’s health outcomes during the first five years of child’s life in countries with health systems similar to Australia: A systematic review. PloS One, 19(3), e0295295. https://doi.org/10.1371/journal.pone.0295295
Pellowski, J., Bengtson, A. M., Barnett, W., DiClemente, K., Koen, N., Zar, H. J., & Stein, D. J. (2019). Perinatal depression among mothers in a South African birth cohort study: Trajectories from pregnancy to 18 months postpartum. Journal of Affective Disorders, 259, 279–287. https://doi.org/10.1016/j.jad.2019.08.052
Using a Community-Based Approach to Improve Maternal and Child Health. (2023, September 27). Stanford Social Innovation Review. https://ssir.org/articles/entry/using_a_community_based_approach_to_improve_maternal_and_child_health#
0 notes
Text
Walk the talk with SADAG
October is a month of global celebration, highlighting National Learning Disabilities Awareness, Cancer Awareness, Active Ageing, and Mental Health Awareness. (Understood.org, 2020). This crucial month attempts to combat the stigma associated with mental illness, particularly in South Africa, where a significant portion of the population faces mental health challenges. (gov.za, n.d) Organisations like SADAG (South African Depression and Anxiety Group) play a vital role in advocating for improved mental health treatment, as mental well-being often remains overlooked in public health. (sadag.org, n.d)

SADAG is actively involved in coordinating various activities, including expert Q&A sessions, fun runs, and the notable Mental Health Advocacy Walk. This walk signifies more than just a stroll; it symbolises a collective journey towards greater understanding, compassion, and personal growth. The aim is to promote mental health, encouraging protective factors and healthy behaviours to prevent mental disorders while reducing risk factors contributing to their development. (Youth.Gov, n.d) Below is the poster for this year's mental health advocacy walk that was held on the 8th of October, two days earlier than the actual World Mental Health Day.

World Mental Health Day, the 10th of October, is an important day for occupational therapists, as it provides an opportunity to raise awareness about mental health and the role that occupational therapists play in helping people with mental health issues. According to the World Federation of Occupational Therapists (WFOT.org, 2019), occupational therapists are in a unique position to support people with mental health issues, as they can help them engage in meaningful activities and improve their quality of life. This is backed by research, such as a study by Lannigan et al. (2019), which found that occupational therapy can improve quality of life and mental health outcomes
The Mental Health Awareness Walk serves as a reminder that even the most significant change can start with a single step. It's not just a walk; it's a shared path towards a brighter, more compassionate society. Participation in such events contributes to a culture that acknowledges mental health, dismantles stigma, and promotes seeking help as a sign of strength.
In conclusion, SADAG's Mental Health Awareness Walk is a powerful initiative uniting people in taking steps toward a mentally healthier South Africa. It reminds us that change begins with us and that the journey toward understanding, compassion, and personal growth is a journey worth embarking upon. As we participate in this walk, let's commit to walking the talk by promoting mental health awareness throughout the year.
References
gov.za. (n.d.). Retrieved from https://www.gov.za/MentalHealthAwarenessMonth2022
Lannigan, E. G., & Noyes, S. (2019). Occupational therapy interventions for adults living with serious mental illness. The American Journal of Occupational Therapy, 73(5), 7305395010p1-7305395010p5
sadag.org. (n.d.). Retrieved from https://www.sadag.org/index.php?option=com_content&view=article&id=3197:world-mental-health-day-10-october-2021&catid=149&Itemid=132
Understood.org. (2020, October ). Retrieved from https://www.understood.org/en/articles/october-awareness-month-celebrating-differences-and-disabilities
WFOT.org. (2019, September ). Retrieved from https://wfot.org/resources/occupational-therapy-and-mental-health
0 notes
Text
The NoteBook of Love
The Notebook, both the movie and novel by Nicholas Sparks, is a heartwarming love story that follows the enduring romance between Noah Calhoun and Allie Nelson. It explores the theme of love, fate, and the power of memories as Allie struggles with amnesia and Noah, who later uses the pseudonym Duke, reads the novel to Allie, who stays in an institution to help her reconnect with their shared past.
True friends are those who still visit you after Alzheimer's has robbed you of your memory of them. In this case, Noah, Allie's husband, remained a true friend to his wife eternally. He sheds light on a valuable therapeutic approach throughout the movie, which is the importance of reminiscence therapy in the lives of individuals living with Alzheimer’s. Reminiscence therapy is an approach normally used by occupational therapists with people with dementia and Alzheimer's disease. It involves the recollection and discussion of past experiences, often through photographs, music, and sharing of stories. (Kennard.C, 2022)
Sharing memories and experiences from the past can evoke positive emotions and feelings of connection. As Occupational therapists, we tend to create a safe and supportive environment for clients to express their thoughts and emotions. (Woods, B. et al.) As OTs, we involve family members, as seen in The Notebook, to ensure that reminiscence therapy continues outside formal sessions. This encourages a support system that nurtures the patient's emotional well-being. As Noah reads their love story from the notebook, it not only helps Allie reconnect with her past but also strengthens their emotional bond. The shared memories evoke strong emotions and feelings, allowing Allie to experience moments of joy, love, and connection despite her condition.
Reminiscence therapy offers a sense of value, importance, belonging, power, and peace. This creates a feeling of intimacy and gives a special meaning to relationships, which in overall improves the client’s self-esteem and helps them develop interpersonal skills. (Kennard.C, 2022). In Allie’s case, it provided her with moments of happiness and a sense of accomplishment, reducing her feelings of confusion and frustration. This allowed her to maintain a conversation with Duke and to express herself clearly as she soon remembered the ending of their love story.
As Occupational therapists, we also use reminiscence therapy to help stimulate the cognitive functions of clients by engaging in conversations and activities related to their past, such as IADLs; meal preparation, community mobility, etc. By doing so, Ots activate the client’s memory pathways, potentially improving cognitive functions and memory. (Guler, A. et al.) Overall, reminiscence therapy promotes cognitive stimulation, emotional well-being, and social engagement, contributing to a higher quality of life for individuals living with dementia. (Braz. J, 2012)
In my mini-world of occupational therapy, ‘The Notebook” serves as a touching reminder that even when pages of memory seem to blur, the emotional connections remain vivid. The movie shows the profound impact that reminiscence therapy has on individuals who have cognitive challenges. Through the art of reminiscence, occupational therapists become the guardians of these treasured memories and stories that provide healing and bring a sense of purpose to those we serve.
References
Aşiret, Güler & Kapucu, Sevgisun. (2015). The Effect of Reminiscence Therapy on Cognition, Depression, and Activities of Daily Living for Patients With Alzheimer Disease. Journal of geriatric psychiatry and neurology. 29.10.1177/0891988715598233.
Braz. J. Psychiatry 34(4). (2012). https://doi.org/10.1016/j.rbp.2012.05.008
Kennard.C. (2022, 04 23). Verywellhealth. Retrieved from Verywellhealth.com: https://www.verywellhealth.com/reminiscence-as-activity-and-therapy-97499
Woods, B., Farrell, E. M., Spector, A. E., & Orrell, M. (2018). Reminiscence therapy for dementia. The Cochrane Database of Systematic Reviews, 2018(3). https://doi.org/10.1002/14651858.CD001120.pub3
0 notes
Text
Therapeutic use of self: my secret to a successful intervention plan.
Occupational therapists get to witness the good, the bad, and the ugly aspects of someone’s personality, preferences, and opinions. However, for the OT process (evaluation, intervention and outcomes) to truly be effective from initial evaluation to discharge, the student therapist needs to reciprocate some vulnerability of their own.
We turn to show our vulnerability in sessions with our client using therapeutic use of self as the therapist. This refers to the therapist's ability to use their own presence, personality, and skills to help their clients achieve their goals. The therapeutic use of self is a dynamic and client-centred process that we, as occupational therapists, adapt to based on individual needs and goals, using our own qualities and skills to support the client’s journey towards improved health and well-being to promote independence.
The definition of the therapeutic use of self is clear, but what does it mean to me, and how have I been using it in sessions. In my sessions with the client, I have used my personality and presence to create a strong and positive rapport. This enabled me to use my interpersonal skills to establish trust and to create a safe, non-judgmental environment. (Chamberlain, n.d.) Being authentic and genuine during our sessions allowed me to be honest about my reactions and feelings within a therapeutic relationship. Hence creating a space for my client to explore their thoughts and feelings. This helped her as she felt heard and validated. Such engagements with my client allowed me to plan a client-centred treatment programme for her, as our sessions were focused on her interest while working on impaired client factors. (Peterson, n.d.)

In reference to the picture. As the therapist in sessions, it is important that I am self-aware of the things I do or say because, beyond a condition, there is a human being who needs to be respected, cared for and given the best OT intervention by me. Therefore, giving my client unconditional positive regard allowed me to accept the fact that my client is trying her best and for me to focus on the here and now of the sessions and not be distracted by emotions and thoughts that may arise within the session. (Abson, 2022) This, however, does not mean I agreed to my client's life choices and routines, but it was for me to encourage my client to participate in rehabilitation efforts as I provided positive reinforcements to celebrate their progress and boost the client's confidence. Little things such as patience, respect and understanding can drive an OT intervention session to the clients' independence.
Lastly, as a student therapist on fieldwork, after a demo, an evaluation is the only thing I look forward to so that I can reflect on what happened during the session, what went well and what I might do differently in the next session. The feedback received from my supervisor allows me to learn and grow as an occupational therapist. I replicate the same approach for my clients as it's done for me. After our sessions, we have reflection time. Reflection provides a platform for the client to become more self-aware to gain insight into their abilities, limitations and challenges to help the client and therapist set new goals and modify existing ones. Through reflection, clients can gain a sense of empowerment and ownership over their therapy journey. They become active participants in the decision-making process, which can boost motivation and engagement. This tailors the client's intervention to be more effective and more client-driven.
Therapeutic use of self is being the best version of yourself so that you can be the best possible OT for your client. To create a therapeutic environment where clients feel understood, supported, and empowered to make positive changes in their lives.
References
Abson, D. (2022, 02 10). TheOTHub.com. Retrieved from https://www.theothub.com/article/therapeutic-use-of-self
Chamberlain, M. (n.d.). OTFlourish. com. Retrieved from OTFlourish website : https://otflourish.com/therapeutic-use-of-self-occupational-therapy/
Peterson, P. (n.d.). clinicient,com. Retrieved from https://www.clinicient.com/blog/client-centered-ot/
Pinterest.com. (n.d.). Retrieved from https://za.pinterest.com/pin/148478118938346538/
0 notes
Text
Me Vs. Cinderella of healthcare
Growing up, the Cinderella story was among the most-read stories, along with The Goldilocks and the Three Bears. Still today, it is one of the most read books to toddlers at creche. The story is about a sweet, beautiful Cinderella, cruelly mistreated by her evil stepmother and stepsisters. Her magical fairy godmother helps her by sending her off to win the heart of a handsome prince and lives happily ever after (Simon & Schuster, Inc, n.d.). How does the context of the story link with mental health being the Cinderella of health care? The ill-treatment Cinderella received from her stepmother and stepsisters made her the forgotten, neglected, and imaginary child in their house. This is the same way mental illnesses are forgotten and ignored within the health care sector, as there is a lot of stigmatisation around the illnesses, the lack of resources due to the tight budget allocated to mental health services, mental health being perceived as a luxury good etc. These factors create a gap that counters unfavourable perceptions and prejudices from the public and from diagnosed individuals. (Gabriel Ivbijaro and Elena Berger, 2016). However, the same way Cinderella had a magical fairy that freed her from her family, mental illness has the World Federation for Mental Health’s international campaign that aims to improve the quality of mental health services, reduce the stigma associated with mental and emotional disorders and protect the human rights of individuals defined as mentally ill.
Occupational therapists work with individuals with mental illnesses or at risk of developing mental illnesses. Our main aim is to ensure that individuals are not expressing occupational imbalance due to their conditions, to ensure that they regain optimal functional outcomes, and for them to have a sense of self-efficacy and accomplishment. We also have a vital role in the promotion of mental health. (HPCSA, 2022)
My colleagues and I are exposed to different mental and emotional conditions in our current placement, namely depression, dementia, schizophrenia, etc. As part of our scope, it would be beneficial to promote the importance of mental health care within the facility to reduce the stigma associated with conditions, allowing residents in the denial stage to learn about conditions and ensure they receive the support they require from caregivers. To close the gap of mental health being the Cinderella within the placement. I aim to use the holistic approach when working with my clients to identify how their condition affects their ability to perform daily tasks, maintain relationships with family and friends, and participate within their environment. Understanding the client holistically will allow me, as an OT student, to bridge the gap will allow me to address the psychological and physical aspects of a person's well-being. This will help my client’s set goals for themselves, develop coping strategies, and regain their independence, which can improve their mental state by, improving their self-esteem and motivation and reducing anxiety in occupational performance.
Social isolation and withdrawal are common challenges for people with mental illness (Morese, R. 2020). As a student placed in that facility, I aim to help the residents build social skills, establish support networks, and engage in community activities. This social integration can reduce feelings of loneliness and improve mental well-being. It will also assist the residents in identifying and participating in activities that bring them joy and a sense of purpose. Engaging in hobbies and social activities can be therapeutic and contribute to improved mental health.
In conclusion, paying attention to mental conditions is essential for health professionals to provide comprehensive care, improve patient outcomes, reduce stigma, and fulfil their ethical and professional obligations. Integrating mental health into daily healthcare practices improves overall health and well-being for individuals and communities.
References
(n.d.). Retrieved from Simon & Schuster, Inc: https://www.simonandschuster.com/books/Cinderella/Charles-Perrault/9780735814868#:~:text=Cinderella%2C%20the%20most%20popular%20of,and%20live%20happily%20ever%20after.
Gabriel Ivbijaro and Elena Berger, W. F. (2016). Civicus.org. Retrieved from Civicus.org: https://www.civicus.org/documents/reports-and-publications/SOCS/2016/Mental%20health%20as%20a%20neglected%20health%20issue%20.pdf
HPCSA. (2022, 11 10). Retrieved from HPCSA: https://www.hpcsa-blogs.co.za/the-occupational-therapists-role-in-promoting-mental-health/#:~:text=Occupational%20therapists%20use%20standardised%20assessments,functional%20limitations%2C%20and%20activity%20restrictions.
Morese, R., Palermo, S., Torello, C., & Sechi, F. (2020). Social Withdrawal and Mental Health: An Interdisciplinary Approach. IntechOpen. doi: 10.5772/intechopen.90735
0 notes
Text
Doing, being, becoming and belonging: my OT journey.
Occupational therapy is a field concerned with promoting health and well-being through occupations. The primary goal of occupational therapy is to enable people to participate in activities of everyday life. This is achieved by engaging people in occupations that they want to do, need to do and are expected to do. (WFOT, 2021) Occupational therapy is a client-centred profession therefore whatever you do is for benefiting the patient. However, my journey studying the qualification has benefited me in a way that I found my inner purpose as to why I want to be an occupational therapist.
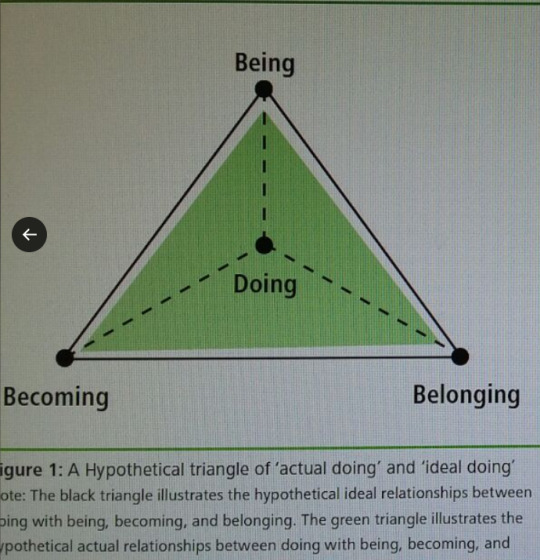
Using the model of occupational wholeness which has four dimensions “doing, being, becoming and belonging”, I have reflected on my journey as an occupational therapy student thus far and my way of moving forward to being a qualified occupational therapist.
Doing focuses on engagement in activities that are important for an individual and how those activities are responsible for shaping their identity and sense of self. (Ayton,2019) Doing occupational therapy has been one of the best decisions I have ever made as it has given as given a chance to learn new skills and grow as an individual. As a person who has difficulties with social interactions studying this degree has allowed me to open up as I am now able to work with patients, my colleagues and supervisors. This has boosted my confidence and gives me a sense of competence in everything that I do.
The concept of being, emphasises the importance of embracing one’s authenticity and cultivating a sense of mindfulness and self-awareness. (Wilcock, 1998). Occupational therapy has given me a chance of connecting with the present moment of my life. This is because I guide others, my patients, on their journey towards well-being. I developed personal growth with the challenges I overcome with my patients, the relationships I have built with them and in their successes in regaining independence in their occupations, these have shaped me to become more empathetic, resilient, and compassionate in myself and the profession.
The becoming dimension of the model revolves around personal growth and the pursuit of one’s aspirations. The road to becoming an occupational therapist hasn’t been easy and still isn’t. As it’s a demanding, and stressful journey because of the workload, and the expectations they have of you in each year of study. Even though that’s the case, this journey has given me a platform to develop personal growth and professional growth. My professional growth comes from hands-on training, and exposure to real-life situations as I have developed practical skills and I now have an understanding that becoming an occupational therapist isn’t just a job- it’s a calling that provides a sense of purpose and fulfilment as you go to bed knowing very well that you have played a role in improving someone’s life and that only brings joy and satisfaction.
Belonging highlights, the importance of social and community connections. It reflects on feeling a sense of belonging and being part of meaningful relationships and social networks. As a person who struggled to engage with others, this degree has changed me to be an ambivert as I can now socialise with my colleagues and patients. I believe I developed these skills through pair-working and group working with them. My colleagues have given me a chance to belong to some sort of community. This has allowed me to make friends and find a sense of belonging within them.
With reference to the model (OTTheory , n.d.), I can conclude by saying I have congruence between my dimensions hence why I have a greater life satisfaction and feeling of wholeness in my OT journey. Refer to the diagram below. Through all the hardships, and growth experiences that I have had within the profession until now. I will continue my journey with an open heart and a curious mind, as ahead of me is a path rich with opportunities for growth, fulfilment, and meaningful connections.
References
Allart Wilcock, A. (1998). Doing, being, becoming. Canadian Journal of Occupational Therapy, 65, 248–257.
Ayton, B. (2019, 09 19). Ideas on Doing, Being and Becoming. Retrieved from Ideas on Doing, Being and Becoming: https://www.linkedin.com/pulse/ideas-doing-being-becoming-brooke-ayton
OTTheory . (n.d.). Retrieved from https://ottheory.com/therapy-model/model-occupational-wholeness#:~:text=The%20Model%20of%20Occupational%20Wholeness,wholeness%2C%20health%2C%20and%20wellbeing.
World federation of occupational therapy(WFOT) , 2012: https://wfot.org/about/about-occupational-therapy#
0 notes
Text
Reflect on cultural humility
Have you ever felt out of place in a new cultural setting? or perhaps struggled to understand a patient's unique cultural perspective as an occupational therapist? These experiences highlight the importance of cultural humility. Cultural humility is a humble and respectful attitude toward an individual of other cultures that pushes one to challenge their own cultural biases, realize they cannot possibly know everything about other cultures, and approach learning about other cultures as a lifelong process. It is a personal commitment to being humble, curious, and flexible both inwardly and outwardly. Cultural humility requires a self-critiquing practice that encourages an open mind and introspection instead of habitually projecting preconceived notions. With cultural humility, we gain a deeper understanding of diverse communities and work towards creating a more equitable and inclusive environment. (Claire Coppage, 2022)
Occupational therapists use cultural humility to get an understanding of cultures that are different from our own and helps us recognize each patient's unique cultural experiences. As family physicians, we treat the whole person. We are involved in the communities we serve, and we maintain ongoing patient-physician relationships. In addition, we are trained to ask many questions. We learn from our patients and their families and acknowledge their cultures and how these cultures affect health, without making assumptions. Through these efforts, we can promote accessible, affordable, culturally proficient, and high-quality care.
Patient-centred care is respectful and responsive to the individual patient's preferences, needs and values, and it ensures that these values guide all clinical decisions. (Health leads, 2018). To achieve this, physicians and staff must be not only culturally competent as we care for our diverse populations and strive for health equity but also culturally humble. Only then might we truly be culturally proficient. Having a humble and respectful attitude toward people of other cultures. It involves ongoing self-exploration combined with a willingness to learn from others. It helps us recognize our cultural biases and realize that we can't know everything about a culture.
One would ask, how do OTs incorporate humility in their intervention? After receiving a referral, the occupational therapist identifies the client, obtains informed consent, establishes therapeutic relationships (first point of contact), provides the client with information to enable them to make informed decisions, and obtains informed consent. The occupational therapist conducts an in-depth assessment of the person, environment and occupational factors impacting the patient’s occupational issue/goals and shares possible recommendations. Culture is highly relevant to intervention in OT because it determines perceptions of health, illness, and occupation (Sonn, I, 2018). There must be an awareness of the patient’s culture to work effectively with him or her and to understand his or her meaningful occupations.
When I was doing my intervention with one of my patients. Even though we were of the same cultural background, we didn’t practice the culture in the same way. I challenged myself not to look at that as an obstacle but as an opportunity to learn about the Zulu culture. The patient was a Zulu lady who strongly believe in ancestors so as a therapist it was my duty to ensure that she gets all kinds of treatment she deserves, and this made me realize that at the end of the day do not judge a person’s cultural background but rather learn from them. “Meeting needs and touching lives “This slogan has been my motor as it was motivating me when doing my intervention, it reminded me that the focus of treatment is for the patient regardless of where they come from each person needs to be independent in their occupations.
It is very important that as OTs, we incorporate cultural formulation with cultural humility to improve cultural sensitivity of the diagnosis and treatment by focusing clinical attention on the patient's perspective and social context and it gives a chance to identify therapeutic implications that can be implemented. Hence, the choice of activity for the patient was guided by the patient’s cultural context, their background. The choice of activity was also realistic to the patient’s societal context which included the cultural, institutional, physical, and social environment in which the client is situated. This aspect of the client guided me in an understanding of occupational challenges and clinical decision-making processes.
Even with one patient I understood their culture and was able to integrate it into our intervention session. However, with other patients, I struggled to incorporate cultural humility into their intervention. Due to this, I have also received critical feedback from my supervisor regarding the need for greater cultural humility in my intervention session and the need to be able to integrate within a written report (case study). In some cases, I have struggled to acknowledge the power imbalance between the therapist and clients and have overlooked the importance of working collaboratively with clients to create culturally sensitive interventions pause.
Despite these challenges, I have taken these critiques to heart and plan to incorporate more cultural humility into my future practices. I have sought out additional training and resources on cultural competence and have made a cautious effort to approach interactions with an open mind and willingness to learn.
As I continue my journey as an occupational therapist, I hope to realize that cultural humility is an ongoing process one that requires ongoing reflection and growth. But by embarking on this concept, I will be confident that I am providing more effective and meaningful interventions to my patients and contributing to a more equitable and inclusive healthcare system.
In conclusion, cultural humility is an essential concept that can transform the way we interact with others in both our personal and professional lives. By recognizing the limitations of our cultural perspective and approaching interactions with openness, respect, and curiosity we can create a more inclusive and equitable environment for all. Whether you are an occupational therapist or simply living your daily lives, cultural humanity can help us build strong connections with those around us and create a more compassionate and understanding world.
For more information on culture humility click on video link: https://www.youtube.com/watch?v=c_wOnJJEfxE
References
Claire Coppage, K. G. (2022, 08 04). Retrieved from Study.com : https://study.com/learn/lesson/what-is-cultural-humility.html
Health leads. (2018, 11 09). Retrieved from healthleadsusa.org: https://healthleadsusa.org/resources/patient-centered-care-elements-benefits-and-examples/#:~:text=The%20Institute%20of%20Medicine%20defines,between%20individuals%20and%20their%20healthcare
Sonn, Inge, & Vermeulen, Nikki. (2018). Occupational therapy students' experiences and perceptions of culture during fieldwork education. South African Journal of Occupational Therapy, 48(1), 34-39. https://dx.doi.org/10.17159/2310-3833/2017/vol48n1a7
0 notes
Text
Reflect on evidence-based practice to guide your intervention
How do occupational therapist plan for their patient’s intervention? How do their work on formulating the appropriate discharge plan for patients? Yes, through understanding the patient and their preferred occupations, and going to university to bag the four years degree however all that is nothing enough as we are not taught everything at university, and we are not exposed to all the conditions and people out there. So, to make our profession what is it today, we use the evidence-based practice approach to work with patients.
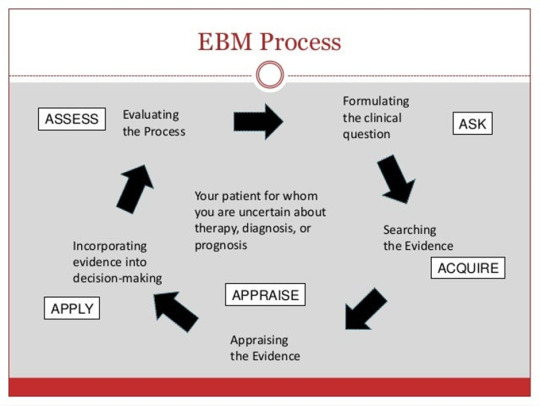
Evidence-based practice is applying research findings in our daily patient care practices and clinical decision-making. (Cabarrus college of health science, 2023) Therefore, the use of evidence-based practice allows us as occupational therapists to use the best available evidence/research to guide our intervention decisions, to improve the patient’s ability to perform occupations independently.
For example, as occupational therapists, we meet new patients daily who present with different conditions that affect their occupation engagement. The patient feels very frustrated and discouraged because of this. Our role is to help the patient regain independence and to find compensatory techniques if needed for the patient to engage in their preferred occupations.
But the question is how do we do so? We work with patients using the OT Process, so we Evaluate, intervene, and have outcomes. Therefore, the first step is to do assessments of the patient’s needs, abilities, goals, and interests by asking questions such as why are the patients seeking services, and what are the patient’s current outcomes in engaging in occupations and daily life activities? What environment/ personal aspects can inhibit or support the patient in the performance of their occupations? etc (AOTA,2020). We even make use of standardized assessments, our clinical observations, and by interviewing the patient’s family, caregiver, and employer. But after doing a thorough assessment and understanding the patient is only the start, how does an OT plan for intervention? This is when evidence-based practice comes in. We need to find the best and most adequate research to guide our intervention decisions.
So, we use research literature to find appropriate studies that are relevant to our patient’s conditions and needs. This helps us to understand the complexity of the clinical issue, gives insight into the scope of the problem, and provides us with the best treatment approaches and best available evidence on the topic. (Casucci & Wilson, 2020).
But evidence-based practice is not about collecting information about the patient’s condition and how that hinders their participation in occupations. Hence, it’s called evidence-based practice one needs to integrate the evidence with their clinical expertise (assessments, observations, interviews, etc.) and the patient holistically (Hopinsmedicine.org, n.d.). This will enable the therapist to use evidence-based recommendations for intervention in the patient's day-to-day practice.
After the implementation of evidence into the patient’s daily life, the therapist will need to monitor and evaluate the outcomes of the intervention. Outcomes are measured with the same method of evaluation and are determined through a comparison of the patient’s status at evaluation with the patient’s status at discharge or through the rehabilitation stages(transition). If needed, necessary adjustments are to be done to ensure that the patient is getting the best possible care. Refer to the picture to see the integration of the research evidence; clinical experience and patient preferences.
After understanding what evidence-based practice is and how it is implemented. I now understand the importance of following the cycle of evidence-based practice in my personal growth as an OT student. As it will allow me to provide more effective and individualized care for my patients.
However, in occupational therapy, it is never about the therapist as we are a client-centered profession so following the cycle is never about benefiting me but it is for the patient. Hence during fieldwork, feedback from the supervisor is crucial. As in the previous week of fieldwork, I have planned intervention sessions that were either unsuccessful or made little difference for the patient. This is because I have been planning sessions without thorough research of the patient’s conditions and their presentation. After receiving valuable feedback from my supervisor on how my sessions lack integration of the patient’s condition, principles of treatment, etc., this has helped me improve my clinical skills and approaches. The feedback has challenged me to be more open-minded about integrating the evidence found in the conditions with my clinical expertise. Last week, I was able to plan a session that was more client-centered that showed a link between the patient's condition and the principles of treatment. The session was a bit of a success in some areas but a lack in some. With this week's blog topic, I can reflect on what was missing in that session; that was research evidence as I was able to use feedback from the previous weeks.
Through the topic, I have gained a deeper understanding of the importance of evidence-based practice in occupational therapy, and using it with feedback continually received feedback from my supervisor allows for self-growth within the profession, to help me provide effective interventions and recommendations for my patients.
In conclusion, evidence-based practice is a crucial component of occupational therapy. By using integrating the evidence with clinical expertise, cultural competence, and individualized care to create meaningful and effective direct and indirect intervention decisions to provide our patients with the highest quality of care. So, the next I work with my patients, I will remember the power of evidence-based practice and how it can help me achieve the patient’s goals and provide them with independence in their occupation.

References
References
Cabarrus college of health science . (2023, March 20). Retrieved from Cabarrus college of health sciencelib guide.com: https://cabarruscollege.libguides.com/c.php?g=527815&p=3608849
Casucci, T., & Wilson, B. (2020, May 12). Accelerate learning community . Retrieved from Accelerate learning community: https://accelerate.uofuhealth.utah.edu/improvement/how-to-conduct-a-literature-search
Hopinsmedicine.org. (n.d.). Retrieved from Johns hopikins medicine: https://www.hopkinsmedicine.org/nursing/center-nursing-inquiry/nursing-inquiry/evidence-based-practice.html#:~:text=EBP%20is%20a%20process%20used,et%20al.%2C%202022).
American Occupational Therapy Association. (2020). Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy, 74(Suppl. 2), 7412410010. https://doi.org/10.5014/ajot.2020.74S2001
http://image.slidesharecdn.com/ebm4obsgynjuly2013topost-130807125100-phpapp01/95/evidencebased-medicine-for-obstetrics-gynecology-5-638.jpg?cb=1375879989
0 notes
Text
Reflect on collaborative practice -multidisciplinary team and teamwork and Reflect on how you have been a health advocate
In a multidisciplinary team, each member has a different role because each professional works with the patient within their speciality area, while collaborating to provide recommendations that work together to improve the patient’s outcomes. In a multidisciplinary team, the occupational therapist has an important role in focusing on promoting functional independence and improving the quality of life for individuals especially those with physical or learning disabilities and mental health through the engagement of occupations such as ADLs, leisure, education etc. (O'Reilly, n.d.) OTs work closely with doctors, physiotherapists, speech therapists, social workers, nurses etc. to provide the best possible care for patients. In occupational therapy, working as a team doesn’t end with working with health professionals only, we also work with families, employers, community members, and teachers this is because we are a client-centred profession, and we aim for independence in all experts of life. Being part of such a large team means one must be willing to share what one knows and be ready to learn from others. (Gethealtie, n.d.) This helps team members understand their colleagues’ roles and responsibilities and the patient holistically.
One for my experiences of working within a multidisciplinary team, I worked with a physiotherapist student on a patient who has a left neck femoral fracture, they initially were trying to get the patient to start walking and to perform passive mobilisation of the leg, however, through teamwork we were able to identify other limitations that led to the patient being assigned a wheelchair, which I as the OT had to provide wheelchair education and training through occupations. This patient also gave me a chance to work with a social worker to founding him a place to stay. The collaboration of us has helped the patient with his functional abilities as he is now able to use a wheelchair while engaging in occupations, it also helped because the patient has found a placement that will be able to cater for needs. These sessions were very effective and beneficial as each team member played their role to provide the best care for the client.
This week's reflection is based on the patient I worked with last week. In the intervention session, I had hoped to improve the patient's level of independence in meal preparation and feeding with her presenting limitations. However, the session didn’t go as planned as the patient presented better than in our previous assessment session and the student therapist failed to upgrade the session to meet the patient’s functional level. After receiving feedback from my supervisor, I was disappointed in myself for failing to plan an appropriate treatment session for my patient. Even though I am disappointed, the most important thing is to use the feedback constructively to improve my skills.
These are some of the ways I am planning to reflect on my intervention and use the feedback to make a change in the future:
I am prepared on seeking clarity from my supervisor on where I went wrong. This will help me understand which specific aspect of intervention I need to improve on. I plan to revisit my intervention plan so that I can modify and improve on the areas identified by the supervisor. I must use more additional resources such as textbooks, and articles to understand my patient’s diagnosis and their presentation. I would have to practice and refine my skills through hands-on participation, to do so I am planning on doing my effectives this coming vacation to build on my experience on the practical side of intervention planning. To work on my theory, for intervention I will be participating in online learning opportunities (like doing the MOCA training). These things will make it easier for me to link the theory learnt in class with the presentation of a patient.
For the feedback received, I want to focus on my strategy mentioned above because I believe as an occupational therapy student, it is important to use the feedback constructively to learn and grow in the field so that I can plan and implement effective intervention sessions that will enable patients to improve on their limitations through participation on everyday activities.
Not only will my strategy work for my current patient, but it will be something I will be doing every time I have an intervention session with other patients so that I become a more effective therapist and provide better care for my patients. It will also enable me to play a critical role within a multidisciplinary team because through effective assessment and intervention planning, adaptive equipment and in collaboration with other health professionals and the patient’s family, I can help patients achieve independence in their areas of occupation and improve their quality of life.
Since my previous patient is discharged. I am working on a new patient this week; I am planning an effective intervention session for the patient which will be focusing on her ADLs. I am also looking forward to working within a multi-disciplinary working for the patient. This will enable me to develop a culture of learning from the other professionals and for them to learn from me because a lot of professionals are still having difficulties differentiating between the roles of an occupational therapist and a physiotherapist. Apart from being part of a team to learn, it will also grow our networks and skills as professionals. Getting myself in a multi-disciplinary team will allow for clear communication between myself (OT), the other professionals and the patient’s family to reduce the objectives, and tasks, and reduces conflict as each member will be clear about what is expected of them. (Indeed editorial team, 2022) For example, as a team we are working on a stroke patient, the patient could need a physiotherapist to get them to start walking, a speech therapist to work on their speech, an optometrist to work on the adjustment of their vision and I as the occupational therapist to work on refocusing independence on the patient's areas of occupations such as ADLs(Feeding), work etc and I will closely work with the family on providing education on the condition and ways of handling the patient to promoting active independence in occupations, and providing education and training on assistive devices provided for the patient.
In summary, a multidisciplinary team is formulated to diagnose patients accurately, formulate the best treatment plans, expedite patient recovery, and create comfortable and trustworthy experiences throughout the patient's recovery journey. All of this may be much easier to accomplish in a collaborative team instead of individuals working separately. (Norrefalk, 2003)
References
Gethealtie. (n.d.). Retrieved from Gethealtie.com: https://www.gethealthie.com/blog/benefits-of-multidisciplinary-care-teams-for-patients#:~:text=Improved%20patient%20outcomes,needs%20in%20an%20effective%20way.
Indeed editorial team. (2022, 10 1). Retrieved from Hk.Indeed.com: https://hk.indeed.com/career-advice/career-development/multidisciplinary-team
Norrefalk, J.-R. (2003). How do we define multidisciplinary rehabilitation. Journal of rehabilitaion medicine , 35: 100-101.
Oncohema Key. (2016, 06 8). Retrieved from Oncohemakey.com : https://oncohemakey.com/11-rehabilitation/
O'Reilly, N. (n.d.). Role of Occupational Therapist in a Rehabilitation Team . Retrieved from Physiopedia.com: https://www.physio-pedia.com/Role_of_Occupational_Therapist_in_a_Rehabilitation_Team
0 notes
Text
Reflection of what is client centredness and what it means to me
A broad definition of what client-centredness means is that the client must make the choices which affect their lives. The client becomes an autonomous decision-maker of what must be done. As such the therapist’s role is to support the client in making the best decision possible so that they don’t decide out of fear or make decisions which will cause harm to themselves or the people around them. But what does client-centredness mean to us as OTs?... As a profession that focuses on occupations, the above definition means that we must allow patients to engage in occupations that they want to do, so as an OT being client-centred is the key to everything because the main aim of occupational therapy is for an individual to regain independence in occupations even though we want them to regain independence it depends on to them to choose the occupations they want to regain independence in. We have to assist and guide them through proper intervention to regain independence in those occupations. As the definition of what is occupational therapy says, Occupational therapy is a client-centred health profession concerned with promoting health and well-being through occupation. The primary goal of occupational therapy is to enable people to participate in the activities of everyday life. Occupational therapists achieve this outcome by working with people and communities to enhance their ability to engage in the occupations they want to, need to, or are expected to do, or by modifying the occupation or the environment to better support their occupational engagement.
The definition is clear, but so what does client-centred mean to me and how I have used it in my sessions. Client-centredness to me means when working with the client, I must identify through assessment what limitations they have and how it is affecting their performances in occupations however the client decides the occupation they want to regain independence in. Therefore, my role is to plan an intervention session using the correct techniques, principles, AFRs and models to help the client regain independence in the occupation of choice. I have previously worked with a patient with a lot of limitations in the performance of occupations such as (ADLs- dressing, grooming, transfers etc) due to affected client factors therefore, he was assigned a wheelchair. The patient's primary goal was to learn how to mobilise in his wheelchair so that he was able to move around. In this case, I had to plan an intervention session that involved the use of the wheelchair while the client was engaging in other occupations, I was doing what the client wanted to do but also ensuring that they are doing what they have and are expected to do at the same time. This made me understand much better what client-centredness in OT practically means.
This week, I worked with a client whose primary goal was to be able to prepare a meal for herself and her family and for her to be able to feed herself independently. Due to that, I had planned to do a meal preparation and feeding session with her. While planning this session I focused a lot on the presentation of the client and forget the cause of the problem and other things( client factors) that might have been limited/impaired. This was evidenced by the feedback, I received from my supervisor. The lack of understanding was crystal clear in my session write-up as my aims weren’t corresponding to any of my principles of treatment (structuring, presentation, handling, and presentation) and this affected the whole session, resulting in the session not being as beneficial as I wanted it to be for my patient. Therefore, in my following sessions, I will have to focus on the client holistically so that I plan proper intervention sessions that will benefit the client hostilely, this means I have to more spend time researching the patient diagnoses and medication and how these affect the patient, look for other commodities and how those affect the patient in performances of their occupations. I believe this will help me found the link between the patient and the suited principles of intervention I should use for the sessions.
So, in conclusion, as an occupational therapy student, I want to grow more towards being client-centred this will help me reinforce independence in occupations the patient wants while engaging them in occupations they have and are expected to do. I can only do this by asking this patient questions such as what matters to you instead of what’s the matter with you. I can achieve this by working by the definition of what is occupational therapy then only I would be able to give the best rehabilitation services through effective research, assessments, and intervention planning for my patients.
I’m sorry to include this in this week's blog. I have been feeling overwhelmed by my workload, which has made me feel very anxious and stressed lately. I feel as if I am not trying enough to understand the concept to put it into practice in my sessions because even if I know the type of session, I want to have the patient I am failing to cooperate with what I want to do with the patient with the correct principles of treatment. Please assist me to step by step as to how I shift from writing an assessment session write-up to a treatment session write-up and how I implement it into a session.
References
(n.d.). Retrieved from MyOT Spot: https://www.myotspot.com/occupational-therapy-quotes/
Baumann, M. K. (2015). What does client centered mena to you? . Retrieved from Intergrative client counselling institute : https://www.icc.institute/iccm/what-does-client-centered-mean/#:~:text=Client%2Dcentered%20refers%20to%20a,make%20decisions%20based%20on%20fear.
0 notes
Text
Reflect on the assessment and intervention that you implemented with your client. You need to reflect on the feedback received from your supervisors and
how will this change the intervention you will provide next week.
08/03/2023
Nompumelelo Mtshali.
I have been in the placement for the past 2 weeks. During these weeks I was able to assess 3 patients. My first patient was Mr M, a 24-year-old. He was diagnosed with chronic kidney disease stage 5. From my observations and assessments with him, I found that he had decreased physical endurance, and decreased muscle strength of both his lower limbs and presented with oedema of both his lower limbs which limited his range of motion. I used lecture notes, a website and a video from youtube to guide my assessment with him. According to OAT.COM, it is advised that OTs should focus on improving physical activity, and improving psychological functioning as patients with this diagnosis show a lot of anxiety and depression symptoms. It is important that as OTs, we also facilitate independence in ADLs, IADLs and Work. In my first with Meluleki, I treated oedema but elevated his legs with a blanket, which was one of the treatment principles from the lecture notes. In the following session, I planned to do a treatment session using an IADL activity( Home Management) unfortunately he was transferred to another hospital. However, I did share with my supervisor the activity I had planned for him. I received great feedback from her but she did say I should incorporate more principles of the AFR I used, in this case, it was the Biomechical AFR however the session was well planned.
My second patient, Ms B was diagnosed with Hydrocephalus. I only conducted assessments with her. My assessment was guided by research from the American Association of Neurological Surgeons that shared that hydrocephalus occurs when a stroke or injury damages the brain and brain matter shrinks. The brain may shrink in older patients or those with Alzheimer's disease, and CSF volume increases to fill the extra space. In these instances, the ventricles are enlarged, but the pressure usually is normal. From this information, I assessed my patient more like a stroke patient as she presented similarly to them. I followed the principles of assessments from the lecture notes for CVA. Ms Baartman is the patient, I did my assessment findings on for the previous week. From the feedback from the supervisor, I did well on the assessment findings but I need to use more OT jargon when reporting, be specific on muscles and joints being assessed and focus on the format of assessments.
My third patient, Mr N has a left neck femur fracture, and pressure sore on his feet. I assessed his ROM, Muscle strength, and endurance and observed for any impaired psychological components as he is old. From his first assessment, I found that he did have limitations in his range of motion of the lower limb, he has muscle stiffness in his upper and lower limbs, and he complained of pain. So from the first assessment, I planned to continue with assessments on 08/03/23. In the assessment, I was aiming to assess his ADLs( Bed mobility- moving from supine to long sitting than too short sitting). The assessment was conducted in the presents of Physio students and the supervisor, from it, the client requires maximal assistance with bed mobility and transfers. I continued with the treatment of wheelchair transfer and wheelchair education with the patient. From the treatment, I had to use principles used for dementia patients. I can't have a feedback session with the supervisor due to time.
As much as I had to work with 3 patients, the week was very stressful which raised my anxiety levels to their maximum. However, I believe I will have the confidence and ability to plan and execute better and more relevant treatment sessions with the use of correct AFRs Principles and other treatment principles for my patients. I will be using feedback and more resource to execute such sessions.
Reference list
Lecture notes for CVA by Mrs Nadioo
Lecture notes endurance, oedema, ROM by Mr Mpanza
Lecture notes muscle strength by Mrs Tupuae
youtube
0 notes