
juniperpublisher-ph
Juniper Publishers | PublicHealth
Juniper Publishers | aims to disseminate knowledge in the field of public health in
order to improve efficacy, effectiveness and efficiency of public health
interventions to improve health outcomes of populations. This aim can
only be achieved by adopting a global and multidisciplinary approach.
151 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

theaasiflifestyle
Beast Creations

theonlygaryking
To Err is Human...So Err...

waterqualityanazex
Untitled

silent-stories
vampires will never hurt you

heartsfourdazai
☆ RUE ☆
Text
Cartographic Principle of the Detection of Blue Stake Hidden Installations in the Tenke Fungurume Mining Cancer in Katanga in The Democratic Republic of the Congo-Juniper Publishers
Juniper Publishers- Juniper Online Journal of Public Health
Abstract
The location, location and mapping of hidden facilities make it possible to avoid the risks of accidents and other nuisances that can cause material and human damage during the various phases of planning and construction of a project. Hence it is important to identify these to solve several problems on a given site. Damaging these buried utilities during construction work; urbanization continues to be one of the major risks for different industries. Currently, it is important to update information on hidden utilities that will serve several scientific disciplines during field work and for successful projects involving excavation, well drilling, exploration drilling, leveling And construction in the field of civil engineering. Bluestake (picketing and marking) processes identify and locate the various hidden utilities such as underground piping, ducting and cable systems, sewers and other installations that can emit a frequency that can be detected during field prospecting . Accordingly, the Blue stake processes are based on the geophysical prospecting method, see the electromagnetic approach using an apparatus consisting of a transmitter, a receiver, electrodes, the ground rod and the electromagnetic field clamp which Of the searched utility sends a detectable frequency and then locates it for mapping.
Keywords: Brucellosis; Community awareness; Goats; Guji; Risky groups; Sero-prevalence
Go to
Introduction
Presentation
This Blue Stake method is applied in the concession of the mining company Tenke Fungurume, which is located in the province of Lualaba ex Katanga in the Democratic Republic of the Congo about 195 Km northwest of the city province of Lubumbashi . This procedure applies not only to the mining concession but also to all operational areas of Tenke Fungurume Mining in the rest of the country (Figure 1).
Problem
The Democratic Republic of the Congo has a number of public services and companies working in various fields such as hydroelectric networks, water and sewerage networks,urbanization services and other areas of civil engineering such as road network construction , dam, earthwork, laying and then other works in geological fields such as drilling and prospecting wells, geo-mechanical survey. Some of the Congolese State’s public services do not have reliable information and detailed maps of hidden underground installations in different sectors where work and various developments are evolving; where there is a risk of accidents which could damage equipment, personnel and the environment if these different installations such as electrical cables, pipes for water supply, telecommunication installations and various cavities on-site do not properly locate, map, identify and mark before performing the different types of work on a given site.
Objective
The objective is to identify research and mark the utilities to meet and then inform and prevent the risks of injuries and various types of accidents that can damage the environment, the ecosystem, or harm human life or cause property damage during excavation and penetration into buildings and land surfaces. As a result, we prepare maps to represent, diagram and locate the various buried installations and of which we do not possess any information. So we have to keep the diagrams, the maps, concern the buried or hidden utilities, and update their schemas if new information is available.
Go to
Principle And Regulation Of The Blue Stake Method (Piquetage-Marquage)
This procedure is applied when we have to penetrate a surface of more than 2.5Cm, excavate, drill, level, dig. During the various inspections of the work on the ground, we must thoroughly inspect the work area concerned by identifying, and marking the various installations located by means of suitable color paint, a drape, a picket or other marking such as lime, cement or ribbon. Thus, localized or detected installations are coded by the following colors: Red: Electric, Yellow: Gas, hydrocarbons, Orange: Communication cable, Blue: Water system, Green: Sanitary sewer systems, drains, sewers, piping Pulp, Purple: Process water from solvent extraction or electrolysis, White: Aeration system. Any field inspection prior to commencement of work such as drilling, drilling platform preparation, excavation, leveling and other civil engineering work must be done at least 48 hours or more before; in order to allow a good identification and elaboration of the detailed maps which can allow the location of the hidden installations on a given site.
Go to
Technology and Methodology for Detection of Entering Networks
Detection by destructive techniques
We mean by destructive technique, any method of sounding which rests on a mechanical and / or manual earthwork, in order to look for the structures not to hang when working nearby, while maintaining their operation [1]. There are two types of digging techniques:
Mechanics: generally deployed during the first tens of centimeters where we are assured of the non-existence of the risk of damage to the structure.
Soft: used when approaching the work on the last tens of centimeters of excavation. They are often established by hand, or by means of a vacuum truck.
During earthworks, the excavation techniques must be adapted according to the nature of the soil and the depths indicated by the network operator. Sometimes the layout of a network does not really correspond to the reality of the terrain, for example when we see that a structure passes at the edge of a tree because we know beforehand that this is not possible. Indeed, the regulation of the roadway provides a radius of 2m from the center of the tree, where no network must pass. In this case, it is necessary to begin by digging the mechanical shovel up to a certain depth (45cm for example), then it is necessary to continue digging with soft techniques. The purpose of the use of intrusive techniques is to expose all the networks entering the work area in order to gain visibility on the position of the structure and also to know precisely its construction material, its outside diameter, its protective coating, and its geometrical characteristics. We can also see singular points such as changes in direction and slope, as well as cut-off organs and their accesses [2].
According to the methodology in this Blue stake procedure (Picketing - Marking) All new underground equipment must have a demarcation wire as well as appropriate safety ribbons buried with the line of material during installation. Thus, gas lines, communication lines, plumbing as well as optical fibers, electrical installations such as low voltage cables must be buried in the ground to a depth of 70cm and then covered with a layer of washed sand, or other fine material approved at least 30cm above the utility lays and then a suitable safety tape with an indication. The medium and high voltage electrical cables must be placed at a depth of 1.20m to 1.50m covered with red dyed concrete and an indication tape located 15cm or 20cm above concrete and then placed at ground level with the naked eye, a plate marked with a sign of visible danger (Figures 2 & 3).
Go to
Detection by non-destructive techniques
At present, there is no non-destructive method which ensures 100% detection of all types of structures, which is why it is necessary to study the different techniques and adapt them to the other types of networks and to the environmental conditions of the project area.
Principle
This non-destructive technique relies on the detection of electromagnetic waves which diffuse in a current-conducting network. The latter can be an electricity or telephone network, but also a pipeline whose construction material allows the current to be transported. This is the case for water, sewerage or gas works that are made of copper, lead or steel. In addition, some networks are not conductive in nature, but they are sometimes installed with Plynox current conductor cables (cable or tracer wire) which allow detection. This is the case for some fiber optic networks. Three methods of electromagnetic detection are used depending on the nature of the networks to be detected, the possibility of access to the network, the presence or not of the flush and the purpose of the detection (avoidance of damage or provision of network mapping: will be detailed in the Principle and use of detection equipment which will be seen below).
Go to
Geophysical Appearance of the Blue Stake Method (Piquetage-Marquage)
The Magnetic Prospecting
Prospecting by artificial or natural electromagnetic fields (EM), generated by currents varying in time, is called electromagnetic prospecting [3-6]. Note that electromagnetic techniques are interesting, even when it is a matter of rapid recognition, a “detection” or the simple discovery of areas of anomalies, quantitative interpretation in several dimensions (2D, 3D) can become very complicated and; is far from “intuitive”. On the other hand, they have a crippling defect: their depth of investigation is limited, the more limited as the frequency of the electromagnetic field is higher. Electromagnetic prospecting equipment is used for a wide variety of conductors, both natural and artificial, such as conductor’s in situ rock (graphite, massive sulphide, shear zones), artificial conductors (electric lines, pipes, metal tanks and pipes, railway tracks ...).
The Concept of Electrical Conductivity
Electrical conductivity is the ability of a material or a solution to let the electric charges move freely, thus allowing the passage of an electric current. Physical Principle: Electrical conductivity is the inverse of resistivity. It corresponds to the conductance of a portion of material 1 m in length and 1 m 2 in cross-section. Some of the best drivers include:
Metals (such as silver, copper, gold or aluminum) for which charge carriers are “free electrons”.
Solutions of electrolytes (having ions in solution). For these, the conductivity value depends on the nature of the ions present in the solution and their concentrations. The conductivity of a solution can be measured using a conductivity meter. Some materials such as semiconductors have a conductivity that depends on other physical conditions, such as temperature or exposure to light, etc. These properties are increasingly used to produce sensors.
The Concept of Electromagnetic Induction
In variable regime, electric field and magnetic field are closely related, and even literally in dissociable. It is from this that comes the name of electromagnetism. A variable magnetic field generates an electric field: in this consists the electromagnetic induction of Faraday. In a conductor, an electric field creates a current, which creates a magnetic field; it is the law of Ampere. The EM prospecting method involves simultaneously three distinct physical processes, namely:
The first consists in the production of a primary magnetic field which varies with time;
The second is the birth of induced currents (eddy currents) in all the conductors on which this primary field acts;
The latter is the detection of these conductors by the measurement of the secondary magnetic fields created by the eddy currents.
The amplitude of currents induced in a conductive body depends on several factors, roughly equivalent, which are: the electrical properties of the conductor; the dimensions and shape of the conductor; the frequency of the primary field; the location of the driver in relation to geophysical instruments
With regard to the Blue stake method, the detectors used apply the principles and methods of geophysical prospecting based on the localization of electromagnetic field induced on different utilities sought on the ground. The different frequencies transmitted by the utilities are picked up (detected) by means of a transmitter and a receiver. Using a GPS, the data are collected and then processed to obtain a map representing different anomalies of the conductors buried in the ground and of which we have no information in a given sector.
Go to
Materials Used in the Blue Stak Method (Pike- Marking)
VLOCPR02
Is an electromagnetic current detector composed of a transmitter and a receiver. The latter acts as a current generator whose power and frequency are modulable. A control screen indicates the various variables which are listed in the table below (Figures 4 & 5).
Presentation and description of receiver
The receiver is as shown below. The tube is made of carbon fiber which makes it resistant and lightweight. In the diagram you can see the different information provided by the main screen: The compass indicates the direction of the search utilities (i.e galvanized cables or pipes); the color changes to blue when the direction is parallel to it (Figures 6 & 7). The arrows help to point to this one while the gauge gives a maximum (or a minimum depending on the mode used) to plumb the utility finds. Also, the detected frequency and a depth gauge (within 10 cm) are shown. Simply press the “i” key to get the depth to the nearest centimeter (in the display, we are not talking here about accuracy) and the intensity of the signal in Ampere. After having connected the transmitter to the network according to the different cases that will be seen below, the measurement in the field is done as follows:
Briefly locate the utilities by scanning from right to left, keeping the detector perpendicular to the ground,
Orient the receiver with the compass (blue light when in the axis),
Check the direction of the utilities by turning the receiver at 90 degrees, the signal must be minimum since it is oriented perpendicularly,
Once the position and direction are established, the base of the detector must be placed on the ground and
“I” to display (“+” to record) current and depth. The detector has an internal memory for recording.
Note that the depth measured is the distance from the base of the receiver (at ground level) to the axis of the pipeline either of the cable or pipe. Thus for networks whose diameter is not negligible, it will be necessary to subtract the length of the radius to have the exact depth of the top generatrix of the network. Attention, in certain cases, the diameter supplied is the nominal diameter, which differs from the outside diameter for some pipes (steel, for example). Always use the outside diameter to calculate the exact depth (Figure 8). Particular attention should be paid when locating in areas with elbows or perpendicular fittings as depth measurements may be imprecise due to distortion of electromagnetic fields. This constraint is very important and obliges us to always be vigilant and to take a critical look at the results obtained (Figure 9).
sebakmt5000: vibratory acoustic impulse detector
Unlike electromagnetic detection, acoustic detection is another non-destructive technique used to detect non-metallic networks. It is currently one of the most relevant methods for identifying plastic structures and connections. This detection technique relies on the injection of pulses by the generator before they are picked up by a receiver at ground level. There are two methods of signal injection:-Injection of pulses on the pipe: fixed on the plumb of the structure by a flange, the generator sends vibrations that are received by an accelerometer. This method is frequently used for water pipes. It has the advantage of not causing the cut of service to the customer. Injection of pulsations on the fluid contained in the pipe: complicated for the implementation, this method often provokes the presence of a representative of the concessionaire of the network, as well as the cut of the service, ensured by the work to the customers, because direct fluid access is required. We can sometimes avoid the interruption of the service by a connection on the “pressure” socket in the box.
Detection of buried networks at 20 cm and generally suitable for non-conductive pipes, this method of detection contains several disadvantages: -No indication of depth of detection: it is therefore not adapted to the mapping of buried networks; Ineffectiveness of detection in the presence of a vegetable ground or under a concrete pavement (field not properly compacted); signal noise in the presence of dense traffic in the vicinity, a sheath or other obstacles above or nearby; difficulty in locating short connections; risk of damaging certain pipes by the injected pulsations. Owing to these disadvantages, this method is increasingly abandoned and replaced by electromagnetic detection and georadar techniques. The following is an example of an acoustic detector [1] (Figures 10 & 11).
Go to
Experimentation and work on land
In this study we use the VIVAX METROTECH vLocPro2 series detector equipped with a transmitter (transmitter), receiver, electromagnetic field clamp (clamp), earth rod, cables and a GPS. Note that the receiver has a compass as a guide, indication and orientation. The transmitter produces an electromagnetic field which is recorded and then picked up by the receiver in the form of the different investigative frequencies during prospecting operations, either in wide mesh and tight on site. These frequencies can be changed depending on the driver located on the ground. The VLocPro2 series detector is a unit that provides radar (radar) functions at several search frequencies. There are two modes of signal detection of the desired installations:
Passive mode or power
only the receiver is used and allows a simple and fast location of most underground networks. This mode is efficient in wide mesh during the general recognition of the various drivers on ground having a large area. Here the network itself emits a wave whose frequency is known, it is the case of some electrical networks; the detector receives this frequency and allows the identification of the utilities induced by this frequency (photo 8). Note that the passive mode is subdivided into:
50Hz mode: which picks up signals at 50Hz come from the under voltage electric cables
And on the metallic networks induced by these cables.
Radio mode: which receives detectable radio signals come from high power transmitters. Radio signals will be used to locate most conductive networks of more than 50 linear meters and of telecommunication cables in burrows and other ground wires for the protection of lightning sensitive equipment.
Cathode Protection Signal Mode (CSP): Allows the receiver to locate the 100Hz frequency generated by a Cathodic protection current generator (Figure 12).
Active mode or active detection
This mode is used when the magnetic field is too weak. A current of a given frequency is circulated in the conduit or the wire rope which is transformed into an antenna, so that from the surface the direction is followed by an indicator compass located on the receiver of the detector. We use simultaneously the receiver and its transmitter which allows to generate a frequency on the sought-after utilities in order to locate and identify these with much more precision and then obtain the information on the depth of the utilities that we seek. Note that this mode is used in reduced mesh in addition the sought conductors must be visible to allow to connect the different accessories of the detector in ground. Thus, this technique is deployed with the use of a current transmitter whose frequency of the signal transmitted must be the same as that of the receiver. This mode has several availabilities for field detection, namely:
Indirect or inductive transmission mode
This mode is used when the contact with the conductive network to be detected is not possible to establish a direct connection. To establish the transmission, we position the transmitter on the surface of the ground in line with the structure so that it can induce a positioning frequency. Moreover, the establishment of the issuer is carried vertically network tracing or geo referencing, referring to the plans from the response to visible utilities field. Nevertheless, this method has technical limitations such as the risk of confusion during the transmission of the signal which is broadcast on the conducting networks close to the detected structure. This can greatly influence the accuracy of plan metric measurements and depth accuracy.Thus, this mode is sometimes used to carry out the layout of underground conductive networks because of its speed of execution of the non-necessity of connecting the transmitter to the network. Nevertheless, it is formally discouraged to use it for geo referencing services, as it is the least accurate mode of transmission (Figure 13).
Connection in direct mode
This mode is used when we have the possibility of access to a conductive part and not protected by an isolation of the network, we connect the transmitter with clamps to the electrodes connected to it by connecting cords and cables. The first cable is connected to the desired conductor and then the second to a ground point with a rod driven into the ground. Thus, the transmitter supplies electrical energy to the desired line or network. The transmitter and receiver must be set to the same frequencies during field searches, and using the compass we can follow the precise orientation of the desired utility. Here the frequencies we had used a frequency between, 8 kHz, and 512Hz. Note that the security measures are very strict, do not connect equipment without the permission of those who manage the research network or on a cable more than 35V. Its combination with high power and low frequency contributes significantly to the realization of greater electromagnetic detection distances. In addition, the transmitter is protected from parasitic currents around it. This makes it possible to obtain the best results, even in the presence of a large underground dense area in buried networks (Figure 14).
The Magnetic Field Clamp (Clamp mode)
The magnetic field clamp allows the signal from the transmitter to be injected into the utility in use. This signal is picked up by the receiver, following the compass the orientation of the utility sought will be easier to trace. Note that the clamp must be well enclosed around the utility. Note that the search utility is visible and accessible to place the clamp with a specific frequency between 8kHz and 200Hz. Moreover, the current emitter allows selection only of a frequency adapted to the clamp. It does not generate any connection to the earth and is particularly useful for detecting power networks. This mode considerably reduces the risk of confusion between conductive networks that are too close. Thus, it allows a more precise detection than that which is guaranteed by the mode of transmission by induction (Figure 15).
Go to
Results of Field Research
In this section, we will present some fieldwork in inductive and passive mode when localization of a pipe of water pipe and electrical cables buried underground. Note that there are several cases but we will illustrate some more general examples.
Case of a Galvanized Pipe
Working in active mode: These data (a and b) were taken using the electromagnetic field clamp (Clamp mode)
a) The transmitter is set at a frequency of 32.8 kHz, by injecting the 100 mA current into the ground (Figure 16).
b) The transmitter is set at a frequency of 65.5 kHz, by injecting the 100 mA current into the ground (Figure 17).
c) The transmitter and its receiver are set to the same frequency (Figure 18).
d) The transmitter is set at a frequency of 32.8 kHz
e) The transmitter is set at a frequency of 65.5 kHz
f) Working in active armature mode: without direct connection
During field work, the receiver and its transmitter are set at the same frequency; For example, in 32kHz mode, in this mode the transmitter is not connected to the utility sought by any connection. The emitter generates an induced electromagnetic field which translates into the waves that enroll the desired utility; the receiver picks up these waves, which appear on the screen as electrical energy in milliampere. Thanks to the compass we can follow the direction of a pipeline or different utilities sought (Table 1).
Case of an Electric Cable
In this case, we had set up the receiver and the transmitter at a frequency of 32 kHz during field reconnaissance, that is, in active armature mode. For safety reasons the equipment used must not be connected to live electrical cables. To establish the transmission, we position the transmitter on the surface of the ground in line with the structure so that it can induce a positioning frequency (Figure 19).
Go to
Cartography of Utilities Obtained
The coordinates of the different utilities sought were obtained thanks to a GPS, in consequence the treatments of these last were made using software GIS and Autocard. Note in this framework we will illustrate the map obtained by the autocard sector software of our field research. These utilities are located at a depth that is not constant. In general, the depth of investigation varies between 0.30Cm and 1.50m depending on whether it is an electrical installation (cable) or a piping installation (Figures 20 & 21). The coordinates taken were put in an Excel file during their processing on autocard but converted into CSV file during processing and digitization on GIS. Note that the map shown below was realized by the drawing software Autocard (Figure 22).
Go to
Recommendation
After the time spent on our research and prospecting on the ground and view the need and importance of this method Blue stake (picketing-marking) hidden utilities of which we have no information in the screen; we recommend to the administrative and administrative authorities of the Congolese State to be able to provide the Republic with laws and norms that can enable the different services of the state such as cadastre, urban planning and civil engineering services and all those working in the fields roads and other construction sites and to individuals see other power companies is inspired and put into practice the standards of this method of Blue stake (picketing-marking) in order to avoid and prevent accidents in their yards or damaging existing utilities that can cause material loss or workers’ lives on the ground or deprive several people or residents of a neighborhood without electrical energy or water after damaging the utilities (photo14). Lack of detailed plans and maps of various utilities can cause very serious damage during excavations, f and drilling on the ground from which the prevention of these various dangers is necessary. Thus the Congolese State or other bodies, or even individuals, could use this Blue stake approach for development projects and urban planning in different societies in order to perform the various tasks safely according to the principles and standards in the framework for environmental protection and sustainable development. Our wish in this area of research and projection in the future; is to extend this method to obtain maps and detailed plans of several sectors which can be consulted by different public services of the state or by private individuals with the major aim of not damaging the utilities meetings and then to update them in cases of excavation discovery and penetration at various sites and sites in accordance with the appropriate safety principles and standards (Figure 23).
Go to
Conclusion
The Blue Stage method, which is a process of identifying, marking, and mapping buried (hidden) facilities, enabled us to work with reduced wire mesh to precisely locate electrical cables and pipe sector of our research in the city of Fungurume in the province located in the vicinity of the national road N ° 39 to the NW of the city of Lubumbashi. During fieldwork, electromagnetic prospecting in active mode where the direct connection of the electromagnetic field clamp connected to the transmitter and around the equipment sought and / or the electrodes connected on the one hand to the ground on the ground, using a ground rod and the other on the utility sought gives much more detail regarding the location, direction and depth of galvanized pipe located in our research explained above. Our finding is that the current injected into the ground from the emitter expressed in milliampere; records a resistivity which decreases as a function of the distance traveled on ground; in other words, the closer you are to the transmitter source (the transmitter), the stronger the signal, the farther away from the source the resistivity decreases, therefore the location and identification of the desired utility becomes more and more more difficult.
The histograms and curves shown above interpret the way in which the required utilities (galvanized electrical cables and pipes) perform during the geophysical prospecting work on an electromagnetic field approach with respect to active mode in direct connection using either the electromagnetic field clamp, or the electrodes pushed into the ground and connected to the equipment (the Vloc Pro2 detector). Let us note that in this case we work in a reduced mesh for more precision on ground. The same applies when working in active armature mode where the transmitter is not connected to any utility (cable, hose) searched on ground. The passive mode is used for general recognition in wide mesh, allowing us to locate different signals that are considered anomaly during field prospecting.
It should be noted that acoustic detection by Hydrolux5000H2 and its acoustic generator PWG / 2-Fast require good attention and hearing when working on terrain; the very sensitive input equipment even registers the surrounding parasites, which can lead to a misinterpretation of the results and therefore be misled.The representation on the map of the utilities by different colors can be explained according to the code which governs this method as seen above in order to distinguish the networks from the electric cables, those of the pipes or the like. It should be noted that the detection of these hidden utilities was carried out on clayey, sandy and talcous soil, as well as on the siliceous and dolomitic shales characterizing the series of mines located in our research area.
For more articles in Juniper Online Journal of Public Health please click on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Text
Comparison of the Work Ability Status in Manual and Office Workers – an Occupational Health Survey-Juniper Publishers
Juniper Publishers- Juniper Online Journal of Public Health
Abstract
Today, disability is turning into a major occupational health issue. Therefore, work ability is forming and developing as a multilateral concept. The objective of this study was to compare work ability among manual and office workers in a manufacturing industry. This cross-sectional study was carried out on 784 workers of a manufacturing industry in 2014. The subjects completed an inventory that measured their work ability based on the work ability index (WAI). Demographic and occupational information of the subjects was also collected. The WAI scores of the manual and office workers were obtained and compared. In total, the response rate to the questionnaire and mean WAI score of workers were 84.40% and 42.46±3.96, respectively. In addition, the mean WAI scores of office workers, older subjects, married individuals, smokers, and subjects with BMI>25 was significantly lower; whereas, work experience and educational level had no impact on this score. Research findings showed that WAI scores of the workers were affected by demographic factors, and thus these factors should be corrected to maintain the score at an optimal level. Moreover, the work potential of all people with different levels of ability can be exploited by modifying current strict recruitment criteria.
Keywords: Work Ability Index; Disability; Work
Go to
Introduction
Workability is a broad concept that includes physical, psychological, and social abilities of a worker to do job and cope with certain occupational and individual needs, health conditions, and psychological and mental resources [1-4]. Today, disability has turned into a major occupational health issue in industrial societies. Therefore, work ability is forming and developing as a multilateral concept. In occupational setting, the vision of work ability generally refers to the equilibrium between resources and individual’s work demands [5]. The assessment of work ability is essential for different reasons including the identification of work ability decline in early stages, investigation into and follow-up assessment of the effects of preventive measures and early rehabilitation, and evaluation of work disability [6].
An applicable method is needed to consider all dimensions of work ability. This method has been developed under the title ‘Workability Index’. In 1980, Finnish researchers developed the Work Ability Index by integrating the concepts of health resources and coping with work demands into work ability to show the current and near future work ability based on job demands, health factors, and psychological resources [7]. WAI is a self-report instrument for the assessment of a worker’s ability to work. It is used in workplaces for establishing objectives to maintain work ability throughout working life and to identify workers prone to disability and early disability-related retirement. This study aimed at measuring work ability and comparing it between manual and office workers, as well as investigating the effect of demographic and occupational variables on work ability in a manufacturing industry.
Go to
Materials and Methods
Study design and subjects
In this cross-sectional study, information of a group of workers in a manufacturing industry in Tehran, capital city of Iran, was collected between December 2013 and November 2014. To collect demographic information, such as age, marital status, BMI, educational level, and smoking status, the workers were asked to complete the questionnaires. Among 817 workers, with at least one-year work experience, who completed the questionnaire, 33 female workers were excluded due to the minority matter. Finally, data of 784 workers were analyzed.
Work Ability Index
The work ability of workers was measured using the 7-item Work Ability Index:
Current work ability compared with the lifetime best,
Work ability in relation to the demands of the job,
Number of current diseases diagnosed by physician,
Estimated work impairment due to diseases,
Sick leave during the past year (12 months),
Own prognosis of work ability two years from now, and
Mental resources
The total WAI score of these seven items ranges from 7 to 49 points. In addition, the total WAI score is divided in four groups, namely poor (7-27), moderate (28-36), good (37-43), and excellent (44-49).The reliability and validity of Iranian edition of this questionnaire have been approved by other studies [8]. The WAI questionnaire was distributed among the workers with at least one year of work experience, who volunteered to participate in the study. The conduction of this study, was approved by the Ethical Committee of Iran University of Medical Sciences.
Statistical Analysis
In this study, WAI was the dependent variable and the independent variables included occupational and demographic characteristics. The Chi-square test was used to investigate the relationship of qualitative variables, the t-test was employed to compare quantitative variables, and regression analysis was utilized to investigate WAI scores among manual and office workers by moderating independent variables. In all test, the significance level was considered as 0.05 with CI=95%. The statistical analysis was done using SPSS16.
Go to
Result
In total, 817 out of 968 workers completed the questionnaire and the response rate was 84.40%. After the exclusion of ineligible subjects, data of 784 workers were analyzed. The age range of the subjects was between 20 and 62 years, with the mean of 35.02±6.79 years. All subjects were male. The mean BMI of the research population was 25.60±2.70, and 6.1% of the subjects had BMI>30. The subjects had the average work experience of 7.51±4.79 years in this industry. More than half of them had average educational level, 27.2% had low educational level, and 18.8% had high educational level. In addition, 88.6% of them were married. Twenty percent of the populations were smokers and 75.9 of subjects were shift worker (Table 1). In addition, 76.9% and 23.1% of the subjects were manual and office workers, respectively. According to data, manual workers were younger and had lower BMI.
The mean WAI score of the research population was 42.46±3.96 with 40.7% of the subjects in excellent, 50.9% in good, 8% in moderate, and 0.4% in poor groups. The mean WAI score of manual workers (42.67±3.75) was significantly higher than that of office workers (41.78±4.51), p=0.008 (Table 2). The mean WAI score of subjects younger than 34 years was 42.99±3.71; whereas, the mean WAI score of subjects≥34 years was 41.96±4.12. This difference was statistically significant (p<0.001).The mean WAI score of smokers and non-smokers were 41.17±4.63 and 42.78±3.70, respectively. This difference was statistically significant (p<0.001). The mean WAI scores of subjects with BMI<25 and BMI≥25 were 43.16±3.63 and 42.08±4.08, respectively (p<0.001).Moreover, the mean WAI score of single subjects was higher than that of the married subjects (43.74±3.47 versus 42.30±3.99). This difference was statistically significant (p=0.001). According to statistics, the WAI scores of shift workers & non-shift workers were 42.60±3.74 and 42.03±4.55, respectively. This difference was not statistically significant. The WAI score of the subjects was not significantly different in terms of work experience and educational level (Table 1). Based on the WAI score, subjects were divided in the Low (7-36) and High (37-49) groups. Results of the Chi-square test from the comparison of demographic and occupational factors between these two groups were almost similar to the t-test results, as follows: The WAI score was negatively correlated with age[OR=3.36( 95% CI: 1.77-6.35), p<0.001] and BMI [OR=2.68 (95% CI:1.33-5.39), p=0.004], and decreased with increased BMI and aging. Manual [OR=1.79 (95% CI: 1.00- 3.20), p=0.049] and shift workers [OR=1.83(95% CI: 1.03-3.25), p=0.049] were categorized in high group with a higher probability. On the other hand, smokers obtained lower WAI score [OR=2.84 (95% CI: 1.61-5.01), p=0.001]. The numbers of single and married subjects were higher in the high and low groups, respectively; however, this difference was not statistically significant (Table 3). Linear regression analysis showed that the WAI score was significantly higher among manual workers after modifying the effect of independent variables, such as age, marital status, BMI, and smoking status (Table 4).
Go to
Discussion
In this study, the WAI score of workers in a manufacturing industry was investigated, and a comparison was made between the manual and office workers in this regard. In addition, the effect of personal and occupational factors on WAI was assessed. The total WAI score of the subjects was 42.46±3.96, on average, with almost 50% of them in the good category and more than 90% in the good and excellent categories. In a study by Alavinia et al. in Holland on office workers, a slightly lower mean score was obtained (41.1±5.1). This difference from our findings may be due to the age of participants, which was higher in their study (35.7 years versus 34 years).In addition, the categorization of their subjects based on WAI score was largely similar to that of our subjects [9], with 42.8%, 45.4%, 9.7%, and 2.1% of subjects in the excellent, good, moderate and poor work ability categories, respectively.
According to our research findings, the total WAI score of manual workers was higher than that of office workers. Results of a study conducted by van der Gulden et al. were different from our findings. In their study, office workers obtained higher WAI score than manual workers [10]. Reasons that explain this difference are as follows: First, given the work and recruitment conditions in Iran, there is far greater chance of employment for workers at higher health level. In addition, the employment terms are much stricter for manual workers than office workers. Therefore, manual workers are usually recruited from completely healthy people, which are less prone to work According to our research findings, the total WAI score of manual workers was higher than that of office workers. Results of a study conducted by van der Gulden et al. were different from our findings. In their study, office workers obtained higher WAI score than manual workers [10]. Reasons that explain this difference are as follows: First, given the work and recruitment conditions in Iran, there is far greater chance of employment for workers at higher health level. In addition, the employment terms are much stricter for manual workers than office workers. Therefore, manual workers are usually recruited from completely healthy people, which are less prone to workrelated disabilities in future (effect of healthy worker). Second, the mean age of office workers was significantly higher than that of manual workers in our study. This difference can justify higher WAI score among the latter group. In addition, the WAI score in our study was inversely correlated with age. Some other studies also reported this inverse correlation of age with WAI score [11-15]. Nevertheless, a study into the health-care shift workers showed lower WAI score among younger workers [16]. In our study, the mean WAI score of smokers was lower than that of non-smokers, which was consistent with the findings of Tuomi et al. and Mohammadi et al. [4,17]. Kaleta et al. [18] also reported a statistically significant correlation between smoking and weak WAI among women. Subject with higher BMI obtained lower WAI score. This finding was consistent with results of previous studies including Tuomi et al. Kaleta et al. and Fischer et al. [4,18,19] who reported a correlation between increased BMI and lower work ability. In our study, single subjects obtained significantly higher WAI scores than married subjects. In a study by Monteiro et al. [20] the excellent and moderate scores were more common among single and married subjects, respectively.
Go to
Conclusion
According to the findings of this study, the WAI score, as a helpful index for establishing workplace objectives to preserve work ability throughout the working life and to identify workers prone to work-related disabilities or disability-related early retirement, is affected by demographic and occupational factors. As a result, attempts should be made for correcting these factors to preserve WAI score at a desirable level. Moreover, our study showed that the recruitment conditions for workers are very strict, specifically among manual workers. Therefore, employment terms should be moderated in favor of employing people with moderate and even weak work ability. In this way, the work potential of all people with different levels of ability can be exploited.
For more articles in Juniper Online Journal of Public Health please click on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Text
Rethinking the Hospital Pharmacist Service: Centralized Logistics– Ict Systems and Clinical Pharmaceutical Care Strategies as a Management Opportunity for Public and Private Institutions-Juniper Publishers
Juniper Publishers- Juniper Online Journal of Public Health

Abstract
In last year’s healthcare costs are increased constantly in logarithmic way and this conditions need an high efficiently resource management system more than past. Drugs, medical devices, diagnostics or medical errors are relevant voice in the public and private hospital current budget and healthcare Institution and government tray every day to control it. (U.S. HEALTH national expenditure amounted total 3.0 -3billion U.S. D. The total spending on medicine in the USA was about 6 more than 400 us dollars in 2015).An high performance HEALTHCARE org. Need today: deep innovations, right management of materials (LOGISTICS drugs and medical devices use), new technologies knowledge, risk management skills and other resource.
Keywords: Change management; Hospital pharmacy; Innovation; Strategy; Healthcare; Pharmaceutical care and Clinical pharmacy; Logistics; Medical error; Clinical outcomes
Go to
Introduction
Strategic, change, knowledge management approach, sharing economy philosophy and other new instruments as velocity management [1] gives improving the global results. (Economic but also clinical). Also Multi-professional medical equip with permanent presence of the clinical pharmacists give improving in global results (clinical - economic outcomes) [2]. Risk management Reduce total costs due by therapy and other kind of error And gives solution to related problems in preventive and proactive way .The clinical pharmacists complete the patient medical team Adding deep pharmaceutical and pharmacological competencies (To prevent ADR, therapy errors, and monitoring the PHARMACOLOGICAL therapy) resulting in more containing in medical error. Inefficacy HR management gives high contributed in the TOTAL results [3] make possible rapid introduction of the different healthcare professionals in EQUIP.
But Today we have also a powerful instrument to efficacy control the costs to be used: centralized logistics systems (to reduce GLOBAL costs of drugs and medical device). The centralized logistic (and regional buying center) make possible a great rationalization in costs and in hospital pharmacy working time.
This system Increase the AMOUNT of orders (Cumulative way) and this make possible to have more discount in drug prices by pharmaceutical industries. The ordering by the different hospital linked and associated in this way this contribute to containing total costs more versus without this strategy. More over This make possible reduce hospital pharmacy stokes (immobilized drugs costs, less expiration data problems) giving the same time continuity to the therapy to the hospital wards in safety way. This systems need a just in time systems and a great support by ICT (healthcare professionals with informatics and data management knowledge.)The rapid communication with the hub and spoke make possible To have the drugs in strictly time.(we can think to saving life drugs especially).The hosp. pharmacist clinical competences gives the correct priority (in ordering procedure) and this is a crucial fact in the global management of the systems.
With centralized logistic need a small stoke of drugs in the hospital pharmacy whit 60-80 kind of molecules (critical medical devices and drugs) and an emergency ICU Drugs Cabinets to cover emergencies (if not ACTIVE an h24 hospital pharmacist service.) The great amount of drugs and medical devices are stoked in central ware house. This approach needs high expertise by the clinical hosp. pharmacist To rationalize the systems without error: right classification of critical drugs and an efficacy risk management system to prevent dis- functions (root cause analysis, FMEA approach, total quality management and other strategy). We can say that the clinical pharmacists works must be an edge between ward the hosp. pharmacy and the hub. (ICT mediated). Other instrument to manage at the right level can be Dose unit drug systems, informative prescription with applied software, oncologic unit’s sterile robot, emergency drugs cabinet systems and some other. All this rationalize the hospital global request of drugs and med devices but also reduce in high way therapy error. ICT technologies provide scurrility system to transfer patient and other data. The total knowledge is increased using these ICT systems. (Biomedical database for prevent interactions, contraindications and other).
But what is relevant in this new process is the active role of hospital clinical pharmacist in more consultant activity versus the classic logistic Functions. (A cultural changes) from the classic logistic function towards more clinical new pharmaceutical consultant functions. This make possible in the same time to adequately monitoring the healthcare costs (drugs and med. devices) containing medical and therapy error, improving also the clinical outcomes [2]. The application of clinical pharmacist presence in stabile way in medical team results in about 35 % cost reduction (drugs, med dev.), costs due by medical errors, reducing recovery days. In example, an Italian practical experience: health ministerial project: “Ward clinical pharmacists in oncology”[29]. A collaboration of: SIFO (Italian Society Hospital Pharmacy), Italian Federation of professional Pharmacists’ Orders, Italian assoc. Of Medical Oncology), EAHP (European Association of Hosp. Pharmacist), a multi-center experience involving 5 public hospitals with the presence of clinical pharmacists in the oncology wards. The result was a reduction of ward drug and MD stokes from 32% to 88% and 30% less of drugs therapy errors [29].
Related to these results. The managerial competences and skills and knowledge of the clinical pharmacist are often requested by general manager office and by physician’s director of the many discipline to monitoring and control the global buying systems [5]. Antimicrobial stewardship [7] , med. Gases pharmacy management , high cost drugs management , medical dev.high competencies ,Toxicological equip with hosp. pharmacists presence ,oncology lab ,ICU, nutrition team service , pain management medical equip , and other involving clinical pharmacist create an high synergy. Other relevant role can be played in surgery field [23] nephrology, heart disease and many other .In ex. the total cost for innovative drug therapy are under an high increase (therapy of hepatitis c ) , antimicrobials meet great resistance ,oncology therapy do not present equal efficacy towards all neo plastic tissue the same .“The economic aspect is relevant on cost of drugs and payment by government and institution or insurance. (In example 35.000 euro/USD/ patient for some biological MABS).Even ministry of health in some countries (ITALY) not pay all some new innovative drugs but use a system that verify the results obtained. (Payment by results or risk sharing et other procedure)” [6]. This problems need a deep and continuous high activity by clinical pharmacist to create a more rational decision making systems in today therapy world.
Go to
Material and Methods
In this observational and research work we report some relevant publications ( in our opinion ) involved in this change and related to the results we have find we submit to healthcare institution a new systems to efficacy control and reduce the healthcare costs improving clinical outcomes .We observe the hospital pharmacy organization in different countries in order to verify The organizational way of works .We describe also a practical research experience involved in management of emergency drug in hospital setting [24]. Then after this research we analyze the total costs involved in this kind of organization change and the advantages that can be obtained.
Go to
Result
Observing the hosp. pharmacy organization in many countries we can say that the pharmacy service is more oriented to the classic function as logistic, galenic lab, nutrition lab, dispensing activities and other.
But only few hosp. pharmacy service are highly oriented to advanced clinical function as advanced center usually do the same the university course involved in hospital pharmacy are more focused on the classic pharmacist function and only in recent decades towards more clinical Functions.(only few cases really involved in improving the clinical outcomes in medical team and not only with monitoring tasks). Also technology applications are not equally available to all hospital places. (Small – large hospitals, rural or city et other). From literature we have find this results: “During 1930 to 2016 a progressive development of clinical pharmacy and pharmaceutical care was developed. We have observed a “general positive influence of the pharmacist’s presence as a part of the medical equip, on public health in various clinical outcomes”; this according to systematic reviews, clinical trials and meta-analysis” [8]. “The model of clinical pharmacy practice adopted by many pharmacy department hospitals is no longer appropriate for the demands of today’s health-care services. Reviews many new models proposed for clinical pharmacy practice including an integrated model for providing a pharmaceutical care management approach in the health-care system. This model is a response to the failures of traditional drug and pharmacological therapy.
It is an idea about how health professionals should integrate their professional work to obtain clinical outcomes important to patients and clinicians” [9]. “Hospital information system is widely used to improve efficiency of china hospitals. A novel clinical pharmacy management system developed by our hosp. was introduced to improve work efficiency of clinical pharmacists, by providing pharmacy information services and promoting rational pharmacological drug use. Taking prescription review in the dep. of surgery, work efficiency of clinical pharmacists, quality and qualified rates of prescriptions before and after utilizing clinical pharmacy management system were compared. Qualified rates of both the inpatient and outpatient prescriptions of the general surgery department increased, antibiotics use decreased. This system apparently improved work efficiency standardized the level and accuracy of drug use, which will improve the rational drug use and pharmacy info service in our place. The utilization of prophylactic antibiotics for the aseptic operations reduced” [10].
“Clinical Pharmaceutical Care “as a new discipline, to improve clinical and economic endpoint in pharmacological therapy reducing therapy errors with a more rational use of resource in medical team. This new approach take advantages by Management discipline and ICT principles. Core training must include Management, ICT new social media, psychological behavior and other skills and attitudes for team working added to the classic clinical pharmacy core programs. The knowledge in field of diagnostic discipline gives great advantages in this field for the high relationship with much drug therapy [11]. “Based on the results of this study, the observed achievements were due to medical lab.
And imaging knowledge and competencies of the clinical pharmacist, as part of the equipe in a hospital setting. Such expertise of the clinical pharmacist has resulted in a significant impact on therapy. For patients’ safety and health and cost reduction and for clinical pharmaceutical care purposes, it is incumbent upon the hospitals to engage and demand an active role from clinical pharmacists, especially in fields such as diagnostics (med. Lab. and imaging) [12]. “to obtain more efficient results in improving some clinical outcomes the clinical pharmacist must have an expert skill in the field of psychological and behavior aspects to use a practical settings when member of medical team .Rotation in different wards provide a a real good experience. This skill and attitudes is useful in pharmacistspatients’ relationship in order to have high patient’s compliance level...” [13]. Reduction of medication therapy errors is needed and demanded by: patients, health authorities, government, insurances companies. “Multi professional healthcare team is the right way of work in health care today. A WARD clinical pharmacist today contributes in many fields: hematology oncology, toxicology, infectious diseases, emergency med., nephrology, nutrition pharmacy service, pain management and others” [11].
The clinical endpoints depend also by the med. device used and pharmacist specialist represents a great resource in cost containment in every level (to use the right one in every different situation) in this specific use. Ph. care principles can correctly be applied in themed. Devices dedicated to the single patient. Consultant activities in properties, classification, legislation, Alternative products, logistic are the working filed in which hospital pharmacist play a relevant roles in medical equipe” [14]. “The innovation introduced with biomed. Databases and searching engine motors improved research works with rapid ways in all kind of scientific areas Internet, and professional social media have brought a great development in rapidly connecting with professionals. The researchers in last 3 decades has been great possibility to share their practical experience more than past with improving results.
They are playing a crucial and relevant role today working field through this rapid development. LinkedIn, Slide share, Research gate, Pub Med, you tube NCBI, Facebook, and other etc. The possibility to create new bridge researchers; with similar interests, discipline with more rapid development ,never seen in last 3 decades”[15]. “In ICU we can see reduction in mortality rate when pharmacist takes really part of the equip. [12]. “Clinical Ph care required more use also of social media to meet researcher in more efficient way. In the same time clinical pharmacist can be a scientific edge between professional in therapy filed. PH care management can be useful tools to have more rational therapy systems.
Drugs are registered for specifically indication, and at the same time every drug to be a rational therapy need a rational decision making system that require a multidisciplinary equipe that can cover all aspect of Pharmaceutical and pharmacological molecular metabolism (also kinetics andPharmacodynamics) this have great possibility for clinical pharmacist but it must increase expertise in field of diagnostic (lab medicine and imaging) for the high relationship whit pharmacological drug therapy. The old algorithm was “physicians - patients - classic pharmacist and drugs “today it must be “patient physicians - clinical pharmacists (as consultant) and drug [16].
“Physicians alone cannot cover all aspect of the pharmacological treatment (for example in the field of drug therapy monitoring, interactions, adverse drug reaction ADR, toxicology, novel delivery systems, immune globulin-based) therapeutics and other innovative drugs and medical devices systems, which have their pharmaceutical specific worlds. This article likes to improve the ph. care application in countries with an advanced healthcare system to provide more rational drug therapy to patients. When not possible, it would be a good idea using ph. care, in particular populations such as: severe disease, critically ill, patients with multiple illnesses, transplants, immunosuppressant, oncology or other serious conditions, at least when the treatments cost a lot” [2]. Using sharing economy instruments we can reduce healthcare costs about 38 -40 % and obtain this results in more rapid way .The results obtained with sharing economy time can be applied in healthcare: sharing of knowledge“ICT systems can reduce errors and waste materials, rotation drugs and med. devices stokes and reducing costs: Dose unit systems and programs reduce costs about 10-15% and ward clinical pharmacist presence in stabile way in medical team can reduce cost about 25-30%.” (8)In a lancet infection disease meta-analysis was reported” Our findings of beneficial effects on outcomes with nine antimicrobial stewardship objectives suggest they can guide stewardship teams in their efforts to improve the quality of antibiotic use in hospitals [17].
According to last editorial The Clinical Pharmacists Main Focus. J Appl Pharma 9: e114 we can see that one of the main focus of the clinical pharmacist “must be applied in priority way to the most critical patients in order to achieve the best results available [12]. In this condition even benefit of 1 life achieved in mortality rate is a real golden endpoint (we can think for example to a pediatric poisoning, or severe infectious disease in pregnancy or the effect of inefficacy immunosuppressive therapy in transplanted et other) [13]. This can be considered in example as reduction in NNT to improve a therapeutic strategy” [18].
We have also see in some practical experience that the introduce in daily works of some technologies make possible a right management (reducing total costs and with safety) in example in emergency drug cabinet systems [7] “no near miss event or other patient risk or even fatal event was observed and was covered the the emergency need of drugs in the 99% of cases, and only 1 time was necessary the central pharmacy call.” (The same results we have observed during One year), we can have also a reduction in total costs providing an efficacy system .( about 50.000 euro in 5 years in an Italian public hospital 700 beds) [24]. Other ICT instruments are in examples dose unit system to provide single Unit of drugs (preventing waste or expiration of pharmacological therapies- full therapy traceability), informatics prescription software (to detect interactions, allergy, toxicity ),Informatics management of narcotic drugs or antidotes for right logistics and other.
Go to
Discussion
Analyzing the literature reported in this work and the results of a specific practical experience [24,28] we can say that using drugs central logistics (hub and spoke pharmacy system) added to ICT instrument and clinical pharmaceutical care and amore clinical pharmacy approach we can have reduced costs about 40%.This result not only due by drugs and med. devices costs rationalized but also by the reducing of med. errors, days of recovery and especially by improving clinical outcomes. In example the costs for an expensive transplant can be lost easy if not applied efficacy pharmacological drug therapy .(the same thinking about complex cardiac surgery or other critical and expensive patients situation).The pharmacist competences/ skills added to ADVANCED ICT INTRUMENTS can improve the global clinical results .This is the reason to shift from the classic logistic competences and skills of clinical pharmacist towards more and deep clinical tasks and to make an intensive ICT use as requested today.
Go to
Conclusion
We think that this kind of change in pharmaceutical dep. is today needed and this shift of hosp. pharmacist competence from the classic logistic roles towards more clinical /economic management tasks.gives reduction of 35-40%in healthcare total costs The application of clinical pharmacist to strictly control the prescription of drugs an M .DEV. (according protocols, guidelines, central - local rules ) make possible an great appropriateness verify [17,18]. We think that the efficacy instruments to the clinical pharmacist and healthcare institution to manage healthcare costs can be:
Management principles and TQM
Clinical Pharmaceutical care (new health care discipline) [19]
ICT technologies
Sharing economy principles of applications
The total costs involved in this change in working activities of hospital pharmacist are included in the costs rationalized by this new management system.(we can say that is not a cost but a resource.)Pharmacy must be considered not only like a definite fiscal place but a complex world where the consultant clinical activities can make the difference in patient outcomes (clinical, economic, quality of life)The core process must be a rethinking in hospital pharmacy competences enhancing the clinical competences level and time dedicated to this specific tasks. This kind of process must involve politics stakeholders institution, healthcare org., decision making hospital general managers, universities and the same all healthcare Professional [20-25].
The principal goal is obtained if this change is accepted by all. The actors and professionals involved in healthcare management agree with this new approach. But is crucial that the same hosp. pharmacist know that in this new organization system other specific kind of responsibility are involved in direct patient clinical pharmacy and pharmaceutical care works .The experience we have see [7] can be usefully transferred to other hospital and other situations giving good results [26,27].
For more articles in Juniper Online Journal of Public Health please click on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Text
Influence of Secondary and Associated Conditions on the Health Status of Persons with Stroke-Related Paralysis: Cross Sectional Analysis of the National Paralysis Survey-Juniper Publishers Juniper Publishers- Juniper Online Journal of Public Health Abstract Objective: To investigate the relationship between secondary (preventable) and associated (sequelae of stroke) conditions and poor health status among US adults with stroke-related paralysis. Design: A cross sectional epidemiological study was conducted using the National Paralysis Survey data. This survey is a random digit-dial survey of over 70,000 households, conducted in 2012-2013, which examines the health of persons with paralysis. Setting: National representative population of persons with paralysis in the United States. Participants: Adults with stroke-related paralysis (n=446) Main outcome and Measures: Descriptive and weighted logistic regression analyses determined associations between poor health status (i.e., fair to poor reported health) and secondary/associated conditions (i.e., contractures, injury, abnormal muscle movement, pain, sleep disturbances, urinary tract infections, autonomic dysreflexia, and sexual dysfunction) among persons with stroke-related paralysis. Results: Sleep disturbances (61%), pain (54%), abnormal muscle movement (49%), and urinary tract infections (45%) had the highest prevalence. All but abnormal muscle movement (p=0.08) were associated with poor health status after controlling for covariates (i.e., age, sex, race, education, marital status, and severity of paralysis). After controlling for covariates and all other conditions, sleep disturbances (OR = 3.26; 95% CI, 1.63–6.51; p<0.001) and urinary tract infections (OR= 2.96; 95% CI, 1.53-5.73; p<0.001) remained associated with poor health status. Conclusion: Sleep disturbances, urinary tract infections, and pain are among the most prevalent to negatively impact health status. Rehabilitation and health promotion activities targeting the prevention of secondary conditions and amelioration of associated conditions could increase the health-related quality of life of this population. Keywords: Stroke; Health Status; Secondary; Associated Conditions Abbreviations: NPS: National Paralysis Survey; UTI: Urinary Tract Infection; CAUTI: Catheterization Associated Urinary Tract Infection Go to Introduction Persons who experience paralysis following stroke frequently also experience other conditions related to their primary condition. Prevention of the frequency or intensity of these secondary and associated conditions can improve health and quality of life. Secondary and associated conditions are physical, mental, and social disorders resulting directly or indirectly from a primary disability [1-3]. Secondary conditions (e.g., pain, urinary tract infections, pressure sores) are considered preventable while associated conditions (e.g., contractures, autonomic dysreflexia, sexual dysfunction) may be mitigated. The objective of this cross-sectional study was to determine the relationship between secondary and associated conditions and poor health status among US adults with stroke-related paralysis. It is hypothesized that certain conditions (i.e., pain and sleep disturbances) are more strongly associated with poor health status than other secondary and associated conditions and should be targeted in rehabilitation and health promotion. Pain and sleep disturbances are common in this population and influence mental states and overall health outcomes [4,5]. Go to Method A cross sectional study was conducted using the National Paralysis Survey (NPS). The NPS was developed by the Centers for Disease Control and Prevention with the Christopher and Dana Reeve Foundation. This population-based telephone survey conducted in 2012-2013 contacted70, 458 households to identify 1,305 households who had at least one person with paralysis. It was cognitively-tested and pilot-tested before field implementation [6]. Participants who responded ‘yes’ to having “difficulty in moving the upper or lower extremities” and identified ‘stroke’ as the condition or health problem that caused difficulty in movement were included in the study. Health status was assessed with the self-report question “In the past 30 days, would you say your general health is: excellent, very good, good, fair, or poor,” and was coded dichotomously (good-excellent v. fair-poor). The NPS asked participants about presence of secondary and associated conditions resulting from their primary disability (yes/no). The conditions utilized in this analysis included: contractures (i.e., loss of joint motion), injury as a result of loss of sensation (i.e., cut, burn, broken bone), abnormal muscle movement (i.e., spasticity, uncontrolled jerky movement, or low muscle tone), pain, sleep disturbances (i.e., difficulty falling asleep, staying asleep, staying awake during the day, waking up early), urinary tract infections (UTI), autonomic dysreflexia (i.e., high blood pressure from overstimulation to the nervous system), and difficulty with sexual function. Demographic and paralysis specific variables included in analyses were age (<45, 45-54, 55-64, >65 years), sex (male, female), race (white, non-white), education ( Prevalence and confidence intervals (95% CI) were calculated for demographics and secondary/associated conditions. Chisquare tests assessed differences among variables and health status. Logistic regression analyses were conducted using appropriate sample weights to correct for differential selection probabilities and adjust for non-coverage and non-response to determine the odds ratio of poor health status for each secondary/ associated condition in independent models and in one combined model with all conditions included. Models were controlled for age, sex, race, education, marital status, and severity of paralysis (i.e., difficulty bathing/ dressing) using State version 13. Go to Result The overall survey response rate was 21%, with 446 persons with stroke-related paralysis identified from the NPS. Poor health status was reported by 60% of persons with stroke-related paralysis (Table 1). Poor health status was most prevalent among adults aged 55-64 years (69.3%), female (61.7%), white (60.4%), single (67.9%), and less than high school education (62.5%). There were significant differences by health status in the distribution of age (p=0.03) and severity of paralysis variables (p<0.001) (Table 1). The following secondary/associated conditions were most prevalent, ranging from 40-60% of the population: pain, sleep disturbances, urinary tract infections, and abnormal muscle movement. All were associated with health status, except sexual dysfunction, which was marginally statistically significant (p=0.06) (Table 1). Logistic regression analyses showed all but abnormal muscle movement (p=0.08) were associated with poor health status after controlling for covariates (Table 2). In a combined model including all covariates and secondary/ associated conditions, only sleep disturbances and UTI remained associated with poor health status (sleep OR = 3.26; 95% CI, 1.63– 6.51; p<0.001; UTI OR= 2.96; 95% CI, 1.53-5.73; p<0.001). Click here to view Large table 1 a May not total 100% because of rounding. bNumber of participants is reduced because of list-wise deletion (i.e., any participants with missing data were excluded). c χ2 test used to calculate P values. Click here to view Large table 2 aModel 1 adjusted for age, sex, race, education, marital status, and severity of paralysis (i.e., difficulty bathing/dressing). b Model 2 adjusted for model 1 variables and other secondary/associated conditions. Go to Discussion As hypothesized sleep disturbances and pain were among the most prevalent to negatively impact health status. Findings also indicate that UTIs were highly prevalent and strongly associated to poor health status in this population. This preventable secondary condition, although common in persons with paralysis, is influencing health status of individuals post stroke. Sleep disturbances occur in more than 50% of stroke patients [4]. The presence and severity of sleep disturbances are typically realized once patients return to their daily lives [7], making post-discharge involvement critical. In conjunction with medical treatment, health promotion activities can enhance awareness of opportunities for improved health through recognizing sources of pain and severe sleep problems and encouraging on-going communication providers. Pain is associated with depression, cognitive dysfunction, and decreased quality of life [5]. It is often under-recognized, undertreated, and persons with stroke are often inadequately educated about their post-stroke pain (5). Although pain was not associated with health status after adjusting for all conditions, this may have been due to the co-occurrence of pain with other conditions. Pain is subjective, and therefore susceptible to measurement error compared with other conditions such as UTI. UTIs are also a common complication in stroke patients [8]. Catheterization-associated urinary tract infection (CAUTI) is caused by prolonged use of a catheter. CAUTI has been addressed by multiple national organizations including the Centers for Disease Control and Prevention, which has developed guidelines for the prevention of CAUTI [9]. The implementation of these guidelines in healthcare facilities, among caregivers and persons with stroke-related paralysis could reduce this preventable secondary condition and improve health status. Go to Study Limitations This study can be generalized to a specific population of individuals with stroke in the United States, specifically persons who initially reported ‘difficulty in moving the upper or lower extremities.’ There are limitations using secondary data sources. The NPS was designed to assess a broader population of persons with paralysis and not specifically stroke, so study findings are weighted to a broader national population of paralysis. Moreover, the study asked participants if they ‘ever’ had the secondary/ associated condition. Resulting, some persons in the study may not have had the condition at the time of the study. Further sexual dysfunction and autonomic dysreflexia had approximately 12- 13% missing data, compared to the other exposures, outcomes, and covariates that had less than 5% missing. This may have affected the individual adjusted models including these conditions and the concurrent secondary and associated condition adjusted model. Go to Conclusion Rehabilitation for individuals with stroke-related paralysis should emphasize self-care and self-monitoring, pain management, healthy lifestyles, and promoting individual control over health [10]. Secondary conditions should be a focus of health promotion activities and complement rehabilitation and medical intervention in order for individuals’ post-stroke to reach an optimal state of health.
For more articles in Juniper Online Journal of Public Health
please click on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click onhttps://juniperpublishers.business.site/
0 notes
Text
Epilepsy and its Association with Depression | Juniper Publishers

Juniper Publishers-Open Access Journal of Toxicology
Authored by Sukaina Rizvi
Abstract
Depressive disorder is a frequent comorbid psychiatric condition in patients with epilepsy. It is more common in patients with temporal lobe epilepsy and frontal lobe seizures. Research has revealed a strong correlation between these two conditions. The early recognition of depressive symptoms in an epileptic patient is a predictor to improve quality of life. Besides treating epilepsy, antiepileptics have a role in treating nonepileptic conditions like mood disorders and pain syndromes. However, it is to be considered that certain antiepileptics decrease seizure threshold and increase seizure frequency.
Introduction
Over the years, a significant amount of research has been conducted showing relationship between epilepsy and depression. Epilepsy and depression are common conditions and often they occur together. Approximately, 40-60% people with epilepsy are affected with depressive symptoms [1]. This is a review article highlighting a strong association between two entities. The main idea behind this review article is to encourage practitioners to keep a close eye on symptoms of depression in people with epilepsy and to treat them accordingly which can impact positively on their quality of life.
Discussion
what is epilepsy? It is important to understand epilepsy on individual basis before moving on further. Epilepsy or a “seizure disorder” is a neurological condition affecting people of all ages. It involves a spectrum of various kinds of seizures, each presenting in a unique way in person to person. The two terms Epilepsy and seizure are used interchangeably; however, these are different in a context of frequency of occurrence as seizure is a single occurrence and epilepsy is two or more unprovoked seizures. According to Epilepsy foundation there are about 3.4 million people in United states who have epilepsy and there are 150,000 of new cases of epilepsy in the United States each year. It is also evident from a systemic review and meta-analysis research by A. K Ngugi, et al that median incidence of epilepsy as almost twice as high in low income countries than of high income countries [2]. The cause of epilepsy could be familial or could be secondary to stroke, brain infection, traumatic brain injury or idiopathic. Diagnosis requires a multidisciplinary approach including clinical presentation along with EEG, CT scan head, MRI, Neuropsychological testing, blood work. There are some seizures which present with normal finding on EEG. These are called pseudo-seizures and require a detail evaluation by a psychiatrist.
Epilepsy tend to impact a person on physical and psychological grounds as the occurrence of seizure is often uncertain. This could lead to an increase risk of mood disorders, physical trauma, cognitive issues, behavioral disturbances, depression, hospitalizations and mortality [3]. It is evident from a survey in UK that people with epilepsy tend to suffer from anxiety and sleep disorders more than the people without epilepsy [4]. This sleep disturbances and anxiety can significantly affect the quality of life in a negative way predisposing a person to develop depression.
As the focus of medicine has transitioned to research, we are now able to uncover that depression and epilepsy often coexist together. It is approximated that life time prevalence of depression in correlation with epilepsy is about 55% [5]. The exact cause of this association is still debatable as various mechanisms explain this link. People with depression have sleep deprivation which can decrease seizure threshold and increase seizure frequency. Preictal psychiatric symptoms usually consists of a constellation of symptoms preceding seizure and can last from minutes to days including prodromal symptom of depressed mood and irritability which is relieved after the onset of seizure or in some cases after few days of seizure activity [6]. Inter Ictal depression or dysphoria consist of brief episodes of crying spells, feeling of worthlessness, anhedonia, helplessness, hopelessness which usually last less than 30sec. In addition, inter ictal depression is also manifested by agitation, psychotic disturbances and impulse control issues which can ultimately predispose to increased suicidal tendencies [5,7]. It is important to recognize all these phases as their prompt recognition and their immediate treatment can lead to prevention of a seizure activity and would also improve quality of life.
It is stated that Depression affects some parts of limbic system of brain which includes amygdala which is a center for emotional/stress responses and hippocampus which has a role in cognition. This results in reduced hippocampal volume and functional or physical alteration of amygdala. Research publication have demonstrated increased risk of depression in patients with temporal epilepsy [5].
This is supported by the temporal lobe epilepsy refractory to antiepileptic medications that could lead to hippocampal sclerosis [8]. Studies have shown some correlation showing that people who have hippocampal sclerosis had a history of febrile convulsant seizure in childhood. Also, there is a study on infants with complex febrile seizures validating that sometimes complex prolonged febrile seizures can lead to acute hippocampal injury which later evolves to hippocampal atrophy [9]. This phenomenon could also explain an association between epilepsy and depressive symptoms secondary to reduced hippocampal volume.
Antiepileptics also have a significant role in various psychiatric disorders where they are primarily used for mood stabilization and for treating anxiety. However, effects of antiepileptics in terms of their therapeutic benefits and side effect profile varies from person to person. It is important to consider that studies performed on one group of people on AEDs should not be implied to another group. This is even more of significance in patients with epilepsy where there is a considerable variation in response to these drugs based on different reactions. Research has shown that people with epilepsy on antiepileptics are more predisposed to increased risk of depression as compared to the other populations [10]. According to Siddhartha, certain antiepileptics are notorious for this behavior which includes levetiracetam, ethosuximide, phenytoin, topiramate etc., which may precipitate underlying depression or anxiety. However, it is interesting to note that some AEDs like lamotrigine have beneficial effects of antidepressants [10,11]. It is stated in publications that each of AEDs act through unique mechanisms which alters the electrochemical gradient resulting in positive or negative behavioral changes. These mechanisms include GABAergic modulation either through stimulating chloride channels or inhibiting GABA uptake and inhibition of voltage gated sodium channels [12]. Landolt hypothesis of forced normalization should also be taken into consideration regarding behavioral manifestation of AEDs which states possibility of depressive symptoms after diminution of epilepsy either through surgery or use of AEDs [5].
There is evidence suggesting that tricyclic antidepressants and MAOI have a dose- dependent potential to decrease seizure threshold. Bupropion has also shown to decrease seizure threshold at all doses. Now there are cases reported in which Bupropion has led to seizure activity even at its extended release formulation. Alternatively, second generation antidepressants SSRI like sertraline, paroxetine, escitalopram does not lower seizure threshold and can be safely used for treating depression in epileptic patient [13,14]. There could also be a strong connection among depression, epilepsy and suicide as a people with MDD harm themselves by over ingesting antidepressants which could be lethal causing seizures or on the other hand, a people with epilepsy can become depressed over time with their illness and try to commit suicide.
Conclusion
In the light of above review article, it is concluded that epilepsy and depression share a unique bidirectional relationship as depression is a most frequent comorbidity in patients with epilepsy. Given their strong correlation a clinician should use a holistic approach to identify depressive symptoms in epileptic patients. There is also a need to investigate about any history of seizure disorder as there is evidence suggesting hippocampal changes in these patients predisposing to depression in later life. It is imperative for practitioners to obtain a through drug history, monitor their drug levels and to make correct choice of antidepressants if treating epilepsy. This also necessitates a need of collaboration between a neurologist and a psychiatrist to manage these conditions.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Toxicology please click on: https://juniperpublishers.com/oajt/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oajt/OAJT.MS.ID.555616.php
37 notes
·
View notes
Text
Analysis of Depression and Anxiety Among Patients Undergoing Surgery for Breast Cancer | Juniper Publishers
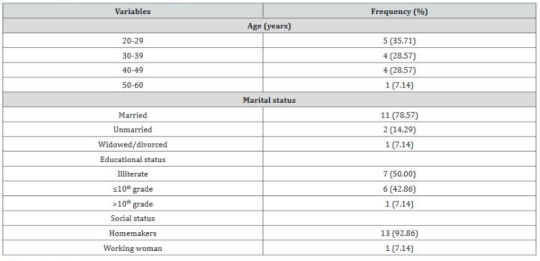
Juniper Publishers-Open Access Journal of Otolaryngology
Authored by Muhammad Ahmad
Abstract
Introduction: Pakistan is a developing country where up to 70% of women present when breast cancer is in its advanced stage. Advanced breast cancer is cancer that is metastatic. Advanced breast cancer is a life threating disease with a poor prognosis profile. Women with a diagnosis of advanced breast cancer engage in a multi-stage cancer treatment cycle often involving surgery, radiation treatment and chemotherapy.
Aims and Objectives: The basic aim of the study is to analyze the sources of distress among patients undergoing surgery for breast cancer in Pakistan.
Material and Methods: This study was conducted at Niazi Teaching Hospital, Sargodha during Dec 2017 to May 2018. Using a purposive sampling strategy, 14 adult female breast cancer patients were selected for this study with variations in their age, educational level, socioeconomic status, and number of exposures to RT. Data were collected through the recording of the face-to-face in-depth interviews, using a semi-structured interview guide.
Results: A total of 14 female breast cancer patients participated in this study. Their age ranged between 20 and 60 years, with an average of 35 years. Majority (79%) of them were married. About 50% of them were illiterate, whereas 43% were matriculate. All of them were Muslims and of Pathan ethnicity. Before RT, all of them had mastectomy of the affected breast, followed by chemotherapy
Conclusion: It is concluded that a substantial number of adult cancer patients were depressed and have a suicidal ideation, causing a significant functional impairment.
Introduction
Pakistan is a developing country where up to 70% of women present when breast cancer is in its advanced stage. Advanced breast cancer is cancer that is metastatic. Advanced breast cancer is a life threating disease with a poor prognosis profile. Women with a diagnosis of advanced breast cancer engage in a multi-stage cancer treatment cycle often involving surgery, radiation treatment and chemotherapy. These cycles of treatment are not free of side effects. Women must face possible disfigurement, surgical pain, the side effects from chemotherapy which can include feelings of anger, frustration, fear, isolation, fatigue as well as burns from targeted radiotherapy [1]. Globally, breast cancer is the most common cancer among women, and a leading cause of cancer-related deaths in this gender. It accounts for 23% of all cancer cases worldwide. The incidence of breast cancer has been increasing rapidly in the developing countries. Among the Asian countries, Pakistan has the highest prevalence of breast cancer, where one in every nine women is at risk of developing breast cancer [2]. In western countries, breast cancer is prevalent among women aged 60 years and above, whereas, in Asian countries, including Pakistan, it occurs during the reproductive age between 30 and 50 years. Hence, women with breast cancer, in Pakistan, may face more challenges due to household and child-rearing responsibilities, as compared to those living in the western countries [3]. According to the American Society for Radiation Oncology, radiotherapy (RT) is a common treatment modality for cancer which is prescribed to about two-thirds of the cancer patients, either before or after surgery. In breast-conserving surgery, RT reduces the chances of recurrence as well as the risk of metastasis and death from breast cancer [4,5].
Aims and Objectives
The basic aim of the study is to analyze the sources of distress among patients undergoing surgery for breast cancer in Pakistan.
Material and Methods
This study was conducted at Niazi Teaching Hospital, Sargodha during Dec 2017 to May 2018. Using a purposive sampling strategy, 14 adult female breast cancer patients were selected for this study with variations in their age, educational level, socioeconomic status, and number of exposures to RT. Data were collected through the recording of the face-to-face in-depth interviews, using a semi-structured interview guide.
Statistical Analysis
Student’s t-test was performed to evaluate the differences in roughness between group P and S. Two-way ANOVA was performed to study the contributions. A chi-square test was used to examine the difference in the distribution of the fracture modes (SPSS 19.0 for Windows, SPSS Inc., USA).
Results
total of 14 female breast cancer patients participated in this study. Their age ranged between 20 and 60 years, with an average of 35 years. Majority (79%) of them were married. About 50% of them were illiterate, whereas 43% were matriculate. All of them were Muslims and of Pathan ethnicity. Before RT, all of them had mastectomy of the affected breast, followed by chemotherapy. Analysis of the interviews data each category and its subcategories are described below with some excerpts from the participants’ narratives (Tables 1 & 2).
Discussion
Breast cancer is second most prevalent type of cancer and is equally common in developing as well as developed countries. The treatment expenditure of breast cancer is a burden not only for people diagnosed with cancer but also for their families and society as a whole. According to American Cancer Society (2010) breast cancer is one of the top three types of cancer that caused the most economic impact ($88 billion) [6]. Though successful treatment options are available to deal with breast cancer, pain and suffering associated with available treatment modalities is significant. Chronic, persistent pain acts as an additional stressor for a person already suffering from many psychological, social and medical stressors [7].
Research has demonstrated association between clinically relevant pain and breast cancer surgery in 10-50% patients. There are pathogenic mechanisms involved in breast cancer like nerve damage and certain sensory disturbances (e.g., burning and sensory loss) are part of side effects of surgical processes [8]. Breast cancer surgery is followed by chronic neuropathic pain syndrome like Phantom breast pain (a sensory experience that is present even after removal of breast and is painful), Inter costo brachial Neuralgia (pain in the distribution of inter costo brachial nerve) and Neuroma pain (pain in the region of scar on breast, chest or arm). Radical mastectomy is most disfiguring type of breast cancer surgery and it involves removal of breast, major and minor chest muscles, and lymph nodes [9]. Breast conserving techniques, another treatment option, were expected to reduce psychiatric morbidity and sexual dysfunction, but none of the studies involving appropriate assessment of psychiatric morbidity showed any advantage of breast conserving therapy [10].
Conclusion
It is concluded that a substantial number of adult cancer patients were depressed and have a suicidal ideation, causing a significant functional impairment. This study clearly demonstrated a significant association between pain complaint and depression among adult cancer patients.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Otolaryngology please click on: https://juniperpublishers.com/gjo/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/gjo/GJO.MS.ID.556003.php
29 notes
·
View notes
Text
SVM based Prediction of Major Histocompatibility Complex Binders: Identification and Analysis of Dracunculus medinensis Peptide | Juniper Publishers
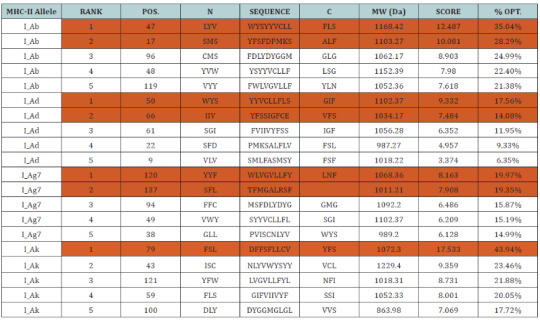
Juniper Publishers-Open Access Journal of Organic & Medicinal Chemistry
Authored by Sonu Mishra
Abstract
The largest human infecting parasite causes guinea worm disease, known as the disease and cause of poverty due to unavailability of the sanitized water. This is not lethal but causes the long term morbidity and motility in the infected human. In this research work, we predict the peptide binders of antigenic protein from D. medinensis sequence to MHC-I molecules are as 11mer_H2_Db, 10mer_H2_Db, 9mer_H2_Db, 8mer_H2_Db.Also study integrates prediction of peptide MHC class I binding; proteasomal C terminal cleavage and TAP transport efficiency by using sequence and properties of the amino acids. We also found the binding of peptides to different alleles by using Position Specific Scoring Matrix. NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis is 145 residues long with 137 nonamers having antigenic MHC binding peptides. PSSM based server will predict the peptide binders from D.medinensis of NADH dehydrogenase subunit 6 sequence to MHC-II molecules are as I_Ab.p, I_Ad.p, I_Ag7.p,I_Ak.p which are found antigenic epitopes region in NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis.
Keywords: Antigen; MHC; TAP; PSSM; NADH dehydrogenase subunit 6; Peptide
Abbreviations: MHC: Major Histocompatibility Complex; TAP: Transporter Associated with Antigen Processing; PSSM: Position Specific Scoring Matrices; SVM: Support Vector Machine
Introduction
The unique life cycle of the D.medinensis takes almost one and half years to complete with unusual six stages. This infection remains asymptomatic during the incubation period. This is one of the largest known human parasites which cause the high rate of the motility and morbidity in infected individuals for long time especially among the school going children’s.
The female worm released the larvae after the incubation period. Cyclops (intermediate host) eats infected larvae which gets entry into the human while drinking the contaminated water where the larvae gets mature and complete their six stages of the life cycle and finally the infectious female releases the infectious larvae which induces a painful blister (1 to 6cm diameter) on the skin of lower limbs; the person develop a slight fever, local skin redness, swelling and severe pruritus around the blister. Other symptoms include diarrhea, nausea, vomiting and dizziness. The severity of the wound infections in the infected individual led to a more complications such as redness and swelling of the skin (cellulitis), boils (abscesses), generalized infection (sepsis), joint infections (septic arthritis) that can cause the joints to lock and deform (contractures), lock jaw (tetanus). The blister burst within 1 to 3 days and female worms one or more slowly comes out from the wounds which causes an excoriating burning sensation and pain .Immersing or pouring water over the blister provide pain reliever. But this the moment that adult female is exposed to the external environment. During emergence of the limbs in open water sources it recognizes the temperature difference and releases the milky white liquid in the water which contains millions of immature larvae, when larvae released in water are ingested by copepods where they mount twice and become infective larvae within two weeks [1-7]. However, Identification of MHC [Major Histocompatibility Complex] binding antigenic peptide molecule will improves the understanding of specificity of immune responses against the pathogen, which is one of the important steps for vaccines discovery.
MHC class I antigen
The presence of the Major histocompatibility complex class I (MHC-I) molecules has been seen on the on the surface of all nucleated cells and display a large array of peptide epitopes for surveillance by the CD8+ T cell repertoire. CD8+ T cell responses,which are essential for the disease or infection control. The CD8+ T cells are actively and efficiently discriminate between the healthy and the infected cell through the recognition of peptides which are associated with MHC-I molecules present on the cell surface. The peptide with the length range of the 8-11 amino acids , are typically derived from protein antigens in the cytosol that arise from conventional as well as cryptic translational reading frames [8]. Proteins which are classically synthesized in the cytosol undergo proteasomal degradation and the resultant peptides are later on transported into the Endoplasmic Endoplasmic Reticulum (ER) and loaded onto MHC-I molecules [9]. Due to the loading of the peptide the class I MHC stabilizes and pass through to the cell surface where the circulating CD8+ T cells scans the complexes which is known as ‘immune surveillance’ [10-19]. Therefore, prediction of TAP binding peptides is important for identification of the MHC class-1 restricted T cell epitopes.
Proteasomal degradation
Proteasomal degradation is important step in the antigenpresentation process to regulate the balance between intracellular proteins [20]. Inside the proteasome by the action of proteinase the antigenic protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis are cleaved into oligopeptides [21] and then these oligopeptides are binds to the TAP, which transports these peptides into the ER.
TAP mediated peptide transport into ER(Endoplasmic Reticulum)
TAP is heterodimeric transmembrane protein, is a family of ABC transporter that transports antigenic peptide (NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis into ER [22] because most of the MHC binding peptides are unable to diffuse across membrane, but TAP protein is capable of transporting the peptide inside the ER where it binds to MHC class I molecules. These MHC-peptide complexes will be translocate on the surface of antigen presenting cells [23] and are recognized by T-cell receptors to elicit an immune response.
MHC class II antigen
The prediction of peptides binding to a MHC class II molecule is difficult due to different side chains and longer length found in the extracellular antigen presentation [24-26]. In the MHC class II antigen presentation process, antigenic protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis are ingested by antigen-presenting cells through the process of endocytosis or phagocytosis, then cleaved by cathepsins a class of protease into oligopeptides in the endosomes, than are fuse with lysosomes containing MHC class II molecules [27] and present them at the cell surface for recognition by T cells [28-36]. Where T helper cells trigger an immune response by inflammation and swelling due to phagocytes or may lead to an antibody-mediated immune response via B-cell activation. Since MHCs have a key role in immune system by stimulating cellular and humoral immunity against NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis and are used for controlling specific immunological processes by creating peptides to bind to specific MHC alleles and this binding affinity to specific peptides are used for designing synthetic peptide vaccines [37-40].
Materials and Methods
Predictions of MHC class I binding peptide
MHC binding peptide is predicted using neural networks trained on C terminals of known epitopes. By using RANKPEP we predict peptide binders to MHCI molecules from protein sequences or sequence alignments using Position Specific Scoring Matrices (PSSMs) whose C terminal end is likely to be the result of proteosomal cleavage.
Prediction of antigenic peptides by cascade SVM based TAPPred method
By using TAPPred we predict TAP binders on the basis of sequence and the properties of amino acids. We found the MHCI binding regions. The binding affinity of NADH dehydrogenase subunit 6 (mitochondrion) from D.medinensis having 145 amino acids shows 137 nonamers.
Predictions of MHC class II binding peptide
MHC peptide binding of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis predicted using neural networks trained on C terminals of known epitopes. By using RANKPEP we predict peptide binders to MHCII molecules from protein sequences or sequence alignments using Position Specific Scoring Matrices (PSSMs). MHC molecule binds to some of the peptide fragments generated after proteolytic cleavage of antigen.
Results and Interpretation
In this research work, we predict the peptide binders of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis sequence to MHC-I molecules are as 11mer_H2_Db, 10mer_H2_ Db, 9mer_H2_Db, 8mer_H2_Db (Table 2). MHC molecule binds to peptide fragments which are generated after proteolytic cleavage of antigen tend to be high-efficiency binders. TAP is an important transporter that involved in the translocation of peptides from cytosol to ER. TAP binds and translocate selective peptides for binding to specific MHC molecules. Therefore, predicting binding affinity of those peptides toward the TAP transporter is crucial to identify the MHC class-1 restricted T cell epitopes. Cascade based support vector machine shows 42 High affinity TAP binder residues at N and C termini using sequence and properties of the amino acids of NADH dehydrogenase subunit 6 (mitochondrion) from D.medinensis (Table 3). This method integrates prediction of peptide MHC class I binding; proteasomal C terminal cleavage and TAP transport efficiency by using sequence and properties of the amino acids. We also found the binding of peptides to different alleles by using Position Specific Scoring Matrix. NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis is 145 residues long with 137 nonamers having antigenic MHC binding peptides. PSSM based server will predict the peptide binders of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis sequence to MHCII molecules are as I_Ab.p,I_Ad.p,I_Ag7, I_Ak which are found antigenic epitopes region in NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis (Table 1).
* The RANKPEP consists of a list of selected peptides binding potential (score) to the MHC molecule from the query given at a selected threshold. Peptides shown here contain a C-terminal residue that is predicted to be the result of proteasomal cleavage and also focus on the prediction of conserved epitopes that help to avoid immune evasion resulting from mutation. Proteasomal cleavage options are only applied to the prediction of MHCIrestricted peptides.
* TAPPred showing Cascade SVM based High affinity TAP Binders sites, their sequence, rank, position and scores are displayed in the tabular output are to be found 42 High affinity TAP Transporter peptide regions which represents predicted TAP binders residues which occur at N and C termini NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis.
Conclusion
NADH dehydrogenase subunit 6 (mitochondrion) an antigenic proteins from D. medinensis involved multiple antigenic components to direct and empower the immune system to protect the host from the pathogenesis. Major histocompatibility complexes I and II (MHC-I and MHC-II) display specificity to bind with their respective epitopes. MHC class molecules are cell surface proteins that take active part in host immune reactions to response for almost all antigens. This knowledge of the immune responses to an antigen protein NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis clear that the whole protein is not necessary for raising the immune response, but a small fragment of antigen can induce immune response against whole antigen. This means the increase in affinity of MHC binding peptides may result in enhancement of immunogenicity of NADH dehydrogenase subunit 6 (mitochondrion) from D. medinensis hence are helpful in silico to design and develop highly predictive computational tools for the identification of T-cell epitopes. Finally, accurate prediction remains vital for the future to design synthetic peptide vaccine.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Organic & Medicinal Chemistry please click on: https://juniperpublishers.com/omcij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/omcij/OMCIJ.MS.ID.555557.php
39 notes
·
View notes
Text
Sero-Prevalence Of Brucellosis In Goats And Community Awareness In Liban District Of Guji Zone, Oromia Regional State, Southern Ethiopia-Juniper Publishers
Juniper Publishers- Juniper Online Journal of Public Health
Abstract
A cross-sectional study was conducted to determine sero prevalence of brucellosis, community awareness about zoonotic importance of the disease and its transmission to goat owners in Liban district of Guji zone Oromia regional state, southern Ethiopia. Study was conducted on 413 goats that are managed under pastoral production system. Sera samples were serially tested using Rose Bengal Plate Test (RBPT). Positive sera samples were retested by complement fixation test (CFT). Questionnaire survey was administered to 153 goat owners to assess community awareness. Collected data was analyzed using SPSS version 15 software. The study showed that goat brucellosis is a moderately distributed with overall sero-prevalence of 6.2% in Liban district. All 153 (100%) respondents in the area recognized abortion but 136 (88.9%) of the respondents have no awareness about zoonotic importance of brucellosis. The current study has determined women and children to be the risky group with higher probability of being infected with brucellosis from goats relative to men as result of close contact they have with goats during parturition, handling of cases like aborted foetus and retained placenta bare handed, milking and caring after goats. Therefore, awareness creation to the community and elimination of positive reactors are recommended to control brucellosis in the area.
Keywords: Brucellosis; Community awareness; Goats; Guji; Risky groups; Sero-prevalence
Go to
Introduction
Brucellosis is a contagious disease caused by bacteria of genus Brucella. In livestock, it is mainly a reproductive disease of the sexually mature animals with predilection site of placenta, fetal fluids and testes of male animals Wadood 2009. It has been recognized as a global problem of wild and domestic animals, especially cattle, sheep and goats Rijpens [1]. The disease is primarily an occupational risk in exposed professions, i.e. veterinarians, farmers, laboratory technicians, abattoir workers, and others who work with animals and their products. The primary source is the animal and infection is contracted either by direct or indirect contact through the skin or mucous membranes or ingestion of contaminated products, especially fresh dairy products. Pastoralists, especially women have direct contact while milking and helping ewes when deliver even with cases like aborted fetus of ewes and retained placenta which could increase the chance of infection with brucellosis Muhammed [2].
Brucellosis is prevalent in all major livestock production systems in sub-Saharan Africa, yet its presence often remains unrecognized through lack of awareness by both veterinarians and health care staff and absence of accessible laboratory diagnostic facilities. As a consequence brucellosis remains a largely neglected disease with little attention to control and prevention except in South Africa where a successful control policy has been instigated McDermott, Arimi [3] Preliminary data suggests that the incidence of brucellosis is highest in pastoral production system where large number of animal mix and lowest for confined farms Muriuki [4], Habtamu [5].
Goat brucellosis has significant economic and zoonotic implication for the pastoral communities in Ethiopia in consequence of their traditional life styles, feeding habits and disease patterns. Hence, knowledge of brucellosis occurrence in pastoral production system has considerable importance in reducing the economic and public health impacts of the disease Rahman and Dabasa [6] In Ethiopia, pastoral area covers sixty percent of the total land mass and holding inhabitants more than 10 million of people in seven regional states and Oromia pastoral area shares the largest percentage of pastoralism in the country PFE, 2004.
Serological studies of brucellosis have been carried out in farm and pastoral areas of the country. However, only few studies have been conducted on small ruminants brucellosis. Reported prevalence include 15% in sheep and 16.5% in goats in Afar Teshale [7] 3.2% in sheep and 5.8% in goats in Afar Ashenafi [8] and 3.2% in goats and 1.6% in sheep Mengistu in Konso; 1.37% Mindaye [2] 9.6% Yohannes [9] The presence of Fraser [10] brucellosis in livestock varies between different regions of the country Hoover and Friedlander [11] Maloney, Furthermore, only few serological studies demonstrated the occurrence of the disease among Borana and Hamer pastoralists PFE 2004.
Pastoralists of Borana area have cultural indigenous range and water ponds management knowledge governing pasture and water ponds and thus settlement is based on some predetermined scenario which allow some group of the community or clan to use these resources Oba [11]. This kind of settlement and livestock mixing, however, can favor disease transmission easily. Study conducted by Dabasa [6] shows that there is history of the disease in the area where sheep and goats are affected by the disease at the prevalence rate of 1.17 and 1.88%, respectively. This indicates that there was no study conducted on separate species of these animals. In particular, there is little information on goat brucellosis across various livestock production systems of southern part of the country, which gave impetus to the initiation of this study. Therefore, this study was designed to undergo serological survey of brucellosis in goats and community awareness about the disease in Liban district of Guji zone.
Go to
Materiel And Method
Study Area
The study was conducted in Liban districts of Guji zone pastoral area, Oromia regional state, southern Ethiopia. Guji zone comprises five pastoral districts namely Liban, Gorodola, Wadara, Girja and Sababoru. Liban district was selected based on presence of high goat population relative to other districts in Borena zone. The major animal species kept in the area include cattle, goat, sheep, camels, poultry, donkeys, mule and horses. Next to cattle, goats are the most important animal species kept in the area for milk production and income generation for small holders. The predominant goats are managed under pastoralism production system (Figure 1).
Study Design and population
A cross-sectional study was conducted on goats kept under pastoral system in Liben district. A total of 413 goats (378 females and 35 males) were tested using RBPT and CFT. All goats that were more than two years old were included in the study. Variables such as sex, age, abortion history, retained placenta and parity number were taken as potential risk factors. Information on each goat was recorded properly while collecting specimen from the goats. Visit to settlements and collection of sample was made early in the morning before the pastoralists start moving in search of pasture. Information related to management system of goats was recorded and responsible household member who care after the goats was also interviewed using semi structured questionnaires.
Sample size and sampling
Selection of animals was based on a stratified sampling method. Five (PAs) namely, Hadesakorat, Malkaguba, Siminto, Bulbul and Karsamale were selected based on their goat population. The five PAs were considered as strata, a total of 75 households were visited where fifteen (15) households were visited from each PAs. Villages and households were selected purposively based on the inclusion criteria (accessibility, willingness of the households to participate in research and security). Taking estimated prevalence of 3% brucellosis in individual animal reported previously by Sintayehu [12] at the area; and taking a confidence interval of 95% and 5% absolute precision, sample size was determined using single proportion formula set by Thrusfield, 2005:
n = 1.962 x Pexp (1-Pexp)
d2
Where: - n = the required sample size,
- Pexp = expected prevalence
- d= desired absolute precision
Therefore, the minimum sample size required was 45 goats. However, to increase the representativeness of the study sample and reduce the design effect, sample size was increased by 9 fold and the total number of goats included was 413. Study animal-related information on each tested goat (such as sex, age, abortion history, retained fetal membrane) was collected and recorded at the time of test.
Go to
Laboratory Techniques
Rose Bengal plate test (RBPT)
All sera sample were initially screened by using Modified Rose Bengal Plate Test (mRBPT) antigen at Yabelo Regional Veterinary Laboratory. Sera and antigen were left at room temperature for half an hour before conducting the test. 75 μl antigen and 25 μl test serum were taken using micropipette and mixed thoroughly on the RBPT plate of the test box using a tooth pick and the box was hand rocked for 4 min. Samples that showed signs of agglutination were recorded as positive while those with no sign of agglutination were recorded negative.
Complement Fixation Test (CFT)
The entire sera tested by RBPT and found to be positive for the test were subjected to CFT for confirmation. The test was conducted at National Animal Health Diagnostic and Investigation Centre (NAHDIC).
Data collection and analysis
All information related to study animal such as age, sex, abortion history and history of retained fetal membrane was recorded in Microsoft excel spread sheet. Recorded information and test result analyzed using SPSS version 15 statistical data analyzing software. Chi-square and P value report was analyzed to compare significance difference of suggestive risk factors.
Go to
Result
Rose Bengal plate test (RBPT)
Out of 413 goat sera screened with RBPT 27 (6.5%), samples were found to be positive for Brucella antibodies. Of these RBPT positive sera, 26 were also found to be positive by CFT giving an overall confirmed brucellosis sero-prevalence of 6.3% in the study area (Table 1) Out of 153 goats owners 136 (88.9%) said they had no awareness about zoonotic importance of brucellosis (Table 2), although almost all of them recognized the existence of abortion locally known, in local language (Afaan Oromo), as”Sallesu” mean abortion. Almost all pastoralists of Liban district assist does during parturition and in removing retained fetal membranes bare handed (Table 2). Drinking of goat milk is common in poor household regularly and it is also consumed in relatively rich family when there is no sufficient milk that they obtain from cows during dry season. However, most of the pastoral community consumes goat milk by boiling the milk with tea known as shayi ananan (shayi adessa) in local language to mean milk with tea (Table 2). Prevalence of Brucellosis is high in Hadesakorat relative in order by Siminto and Malkaguba but has no statistically significant variation between PAs (Table 3).
Go to
Discussion
Brucellosis is bacterial disease of animals with zoonotic and economic implication worldwide Corbel [13]. The overall sero-prevalence of goat’s brucellosis in the current study area, based on RBPT was found to be 6.5% whereas on the basis of CFT, determined to be 6.2%.The Seroprevalence of brucellosis showed that it is moderate relative to previous reports on brucellosis. This is fairly in agreement with the report of Yohaness [9] who reported 11.10% prevalence in goats using RBPT in Yabello district. However, the current finding result is lower than that of Al-Majali [14] where 27.7% (305 of 1100) of goats were seropositive by RBPT and CFT. This result is slightly higher than report of Sintayehu [12] which was 3% in Borena area of souther Ethiopia. But the present study is higher than, finding of Bekele [15] at Jijjiga who detected brucellosis 2.3% (7 of 309) in goats using RBPT and 1.9% (6 of 309) using CFT and Tekelye, Kasali [16] who recorded 1.3% in goats in central highlands of Ethiopia. This difference in sero-prevalence of brucellosis within the same ecosystem could be described as strong clan-based segregation of animals and range lands in the pastoral area Teshale, Bekele [16] Differences in geographical location and livestock management in the central high lands or low lands of the country could be due to mixed farming in the high lands, in which fewer animals are raised separately Ferede [17] However, the higher prevalence rate detected in pastoral area could be due to variations in the management practices in pastoral area, free movement of animals or frequent introduction of new animals without prior serological testing and keeping of animals with high incidence of abortions. This is in agreement with previous reports of Hamidullah [18], Negash [19].
In present study area, goat owners use common grazing range lands and watering points which created relatively higher prevalence rate of brucellosis as reported by different researchers on brucellosis Teshale [7] Negash [19] In the present study, a higher sero-prevalence recorded in males (20.0%) than in females (5.3%) with significance difference occurrence of brucellosis (Table 1); this result is contradictory to report of Negash [19] that serological prevalence was lower in males (8.99%) as compared to females (9.22%). This could be due the method used to collect sera sample and sex composition difference. In the present study, 88.9% of the pastoral community in the study area has no awareness on zoonotic importance of brucellosis. This is in agreement with study conducted in Jima zone by Bashahun [20-24] where they found that 97% of the respondents said they have no awareness on zoonotic importance of Brucellosis. Women and children are risky group among family members mainly exposed to the disease. Furthermore, 150 (98%) of the owners were found to have habit of handling cases like abortion and retained placenta with bare hand which is in agreement with report of Bekele [14], Negash [19] Handling cases could be main way of transmission of disease from human to animals and increase chance of the risky groups to be infected by brucellosis [25-30].
Go to
Conclusion
Brucellosis is transmissible from animals to humans through consumption of contaminated milk, raw milk products, meat or direct contact with infected animals. Women and children’s close contact with goats while milking and keeping flock, unsafe handling of placenta, aborted fetus and assisting births bare handed were common practices among analyzed population. These practices may predispose children and women to acquire brucellosis from goats which are reservoirs of the most pathogenic Brucella species, B.melitesis for human and animals [31]. Therefore, collaborative activity between veterinarians, physicians and other governmental and nongovernmental organizations is needed to take preventive and control action through educating communities and creating awareness on zoonotic importance of brucellosis.
For more articles in Juniper Online Journal of Public Health please click
on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Text
Ionic liquid as Functional Dispersant for Nanomaterials in Polymer Matrix | Juniper Publishers

Juniper Publishers-Open Access Journal of Polymer Science
Authored by Jiji Abraham
Abstract
Ionic liquid has been used as a novel dispersant for fillers in polymer matrix. Enhanced interfacial interaction between reinforcing material and polymer matrix leads to smart materials. Use of ionic liquid as a modifier is environmentally friendly method to fabricate nanocomposites potential applications.
Keywords: Ionic liquid; Polymer matrix; Interfacial interaction; Potential applications
Abbrevations: RTILs: Room-Temperature Ionic Liquids; MWCNT: Multiwalled Carbon Nanotube; GO: Graphene Oxide; BNNS: Boron Nitride Nanosheets; BIIR: Bromo butyl Rubber; ILs: Ionic Liquids; GO-ILs: Modified Graphene Oxide; MEMS/NEMS: Micro/Nanoelectromechanical Systems; ZIL: Zwitterionic Imidazolium-Based Ionic Liquid
Ionic liquid as a Functional Dispersant for Nanomaterials in Polymer matrix
Potential applications as well as strength and durability of polymers can be enriched by the reinforcement using various nanosized fillers. However wide spread application of nanomaterials as reinforcing agents has limited due to their processing difficulty and the tendency to form agglomerates. Incorporation of active groups on fillers by emerging chemistry is a good method to overcome the problems associated with filler dispersion. At present, many advanced strategies have been developed to improve the dispersibility and stability of nanofillers in solvents and matrices which include (a) the covalent attachment of functional groups through chemical reactions (b) the non-covalent adsorption or wrapping of various functional molecules. Due to some structural alteration and the need of additional solvent during covalent fictionalisation, non-covalent functionalization is preferred.
Non-covalent functionalization of fillers by Room-Temperature Ionic Liquids (RTILs) has got considerable attention in these days. RTILs, usually liquid at or near room temperature are non-volatile, non-flammable and thermally stable. They provide an environmentally benign “green” alternative to organic solvents for chemical synthesis, extractions and bio catalysis [1].
Use of ionic liquid as novel dispersant for fillers has been developed as an environment friendly technology to functionalize them. Commonly reported dispersants are solid in state which needs additional solvent to disperse nanomaterial. In contrast ionic liquids are fluid at room temperature and are made entirely of ions (asymmetric cation and a symmetric anion) [2].
Das et al. first reported the use of ionic liquid as a dispersing agent for Multiwalled Carbon Nanotube (MWCNT) [3]. Cation-π interaction between cationic part of ionic liquid and π conjugated MWCNT surface is the reason behind the dispersion of MWCNT. Since ionic liquid can act a dispersant, it will improve overall performance of the nanocomposites. Researches from the same group had tried different ionic liquids to functionalize MWCNT and studied its effect on various properties of fabricated nanocomposites. These studies showed a clear evidence for the enhanced dispersion of MWCNT in presence of ionic liquid, improved cure characteristics, mechanical performance, dielectric characteristics, electrical conductivity, ionic conductivity, thermal stability, thermal conductivity oxidation resistance, thermo mechanical properties and processability. Flexible and stable electromagnetic shielding materials can be fabricated with the aid of ionic liquid modified MWCNT [4,5].
Studies also reported in the area of dispersing other fillers like graphene, graphite oxide, graphene oxide, clay, layered double hydroxides, silica, carbon black etc. with the aid of ionic liquid. On mixing Graphene Oxide (GO) and ionic liquid, ILs had been effectively intercalated into the interlayer of GO, which was found to be able to raise the exfoliation degree of GO. It is found that both thermal stability and the thermal conductivity of Bromobutyl Rubber (BIIR) nanocomposites could be improved by incorporating the Ionic Liquids (ILs) modified graphene oxide (GO-ILs) [6]. Tribological study of functionalized graphene-IL nanocomposite ultrathin lubrication films on Si substrates the promising applications in the lubrication of micro/nanoelectromechanical systems (MEMS/NEMS) [7]. It is possible to control the pore size, electrical conductivity and mechanical robustness of the polyurethane nanocomposite foam by incorporating it with modified the graphene oxide using 1-methyl imidazole chloride ionic liquid [8]. Boron Nitride Nanosheets (BNNS) are exfoliated with the help of ionic liquid by physical adsorption on IL on BNNS surfaces. Highly thermally conductive and electrically insulating polymer nanocomposites can be prepares using this material [9].
Ionic liquid can be used as interfacial agent or surfactant or organic modifier for layered double hydroxide in polymer nanocomposites [10]. Ionic liquids were used as an environmentally friendly material to improve the processability of layered silicates containing polymer nanocomposites [11]. Zwitterionic Imidazolium-Based Ionic Liquid (ZIL) was used to modify both cationic and anionic clay minerals. The ZIL was able to penetrate into the interlayer space of clay and modified the interfacial properties [12]. Studies have been reported on the role of ionic liquid as an interfacial modifier for silica and as a cure accelerator in polymer nanocomposites [13].
In conclusion the use of ILs afforded not only high-yield, mild, facile exfoliation of various fillers but also non-covalent functionalization of fillers for multifunctional applications. Merging processing techniques of nanocomposites with ionic liquid for efficient dispersion of nanomaterials facilitates the development of new, high performance materials.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Polymer Science please click on: https://juniperpublishers.com/ajop/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ajop/AJOP.MS.ID.555576.php
26 notes
·
View notes
Text
Beauty, A Social Construct: The Curious Case of Cosmetic Surgeries | Juniper Publishers
Juniper Publishers-Open Access Journal of Dermatology & Cosmetics
Authored by Vandana Roy
Abstract
In this article we deconstruct the social norm of beauty and cosmetic beauty treatment, an issue that is seldom discussed in medical circles and is often lost to popular rhetoric. In doing so, we also reflect on the institutionalized system of social conditioning.
A Historical Perspective
Cosmetic surgery, as with reconstructive surgery, has its roots in plastic surgery (emerging from the Greek word ‘plastikos’, meaning to mold or form). The practice of surgically enhancing or restoring parts of the body goes back more than 4000 years. The oldest accounts of rudimentary surgical procedures is found in Egypt in the third millennia BCE. Ancient Indian texts of 500 BCE outline procedures for amputation and reconstruction. The rise of the Greek city-states and spread of the Roman Empire is also believed to have led to increasingly sophisticated surgical practices. Throughout the early Middle Ages as well, the practice of facial reconstruction continued. The fifth century witnessed a rise of barbarian tribes and Christianity and the fall of Rome. This prevented further developments in surgical techniques. However, medicine benefited from scientific advancement during the Renaissance, resulting in a higher success rate for surgeries. Reconstructive surgery experienced another period of decline during the 17th century but was soon revived in the 18th century. Nineteenth century provided impetus to medical progress and a wider variety of complex procedures. This included the first recorded instances of aesthetic nose reconstruction and breast augmentation. Advancements continued in the 20th century and poured into present developments of the 21st century.
Go to
Desires and Demands in Contemporary Times
In recent years, the volume of individuals seeking cosmetic procedures has increased tremendously. In 2015, 21 million surgical and nonsurgical cosmetic procedures were performed worldwide. In the United Kingdom specifically, there has been a 300% rise in cosmetic procedures since 2002. The year 2016 witnessed a surge in the number of such treatments with the United States crossing four million operations. Presently, the top five countries in which the most surgical and nonsurgical procedures are performed are the United States, Brazil, South Korea, India, and Mexico. Such demand can be viewed from different perspectives. At one end it is a product of scientific progress, growing awareness, economic capacities and easier access and on the other, something on the lines of a self-inflicted pathology. This article dwells on the latter and attempts to address a deep-rooted problem of the social mind.
Lessons from History
History is witness to a number of unhealthy fashion trends, many of which today appear extremely irrational and even cruel. Interestingly, the common thread connecting all of them is the reinforcement of social norms and stereotypes. Forms of socialization which lie at the intersection of race, class and gender-based prejudices. To elaborate, hobble skirts and chopines restricted women’s movement and increased their dependence on others. Corsets deformed body structures, damaged organs and led to breathing problems. The Chinese practice of binding women’s feet to limit physical labor was regarded as a sign of wealthiness. Dyed crinolines and 17th century hairstyles made people vulnerable to poisoning and fire related injuries. Usage of makeup made of lead and arsenic, eating chalk and ‘blot letting’, reflected a blatantly racist obsession with white and pale skin. Lower classes faked gingivitis to ape tooth decays of the more privileged who had access to sugar. Furthermore, other practices like tooth lacquering, radium hair colors, mercury ridden hats, usage of belladonna to dilate pupils and even men wearing stiff high collars, all furthered societal expectations and notions of class superiority. Till the 1920’s, there was rampant usage of side lacers to compress women’s curves. Even today many ethnic tribes continue with practices which inflict bodily deformations. In the urban context as well, trends like high heels, skinny jeans and using excessive makeup dominate the fashion discourse. Cosmetic procedures are the latest addition to the kitty.
The Social Dilemma
What is it that leads the ‘intelligent human’ of today to succumb to archaic and regressive notions of beauty? What motivates them to risk aspects of their lives to cater to selflimiting rules of ‘acceptance’? The surprising part is that this anomaly is often placed in the illusory realm of ‘informed consent’. In common parlance, ‘to consent’ implies voluntary agreement to another’s proposal. The word ‘voluntary’ implies ‘doing, giving, or acting of one’s own free will.’ However, when the entire socio-cultural set up and individual attitudes validate certain behaviors, there is very less space left for an alternate narrative. Let alone free will.
Pierre Bourdieu once argued that nearly all aspects of taste reflect social class. Since time immemorial, societal standards of beauty have provided stepping stones to social ascent and class mobility. Better ‘looking’ individuals are considered to be healthier, skillfully intellectual and economically accomplished in their lives. Such an understanding stems from well entrenched stereotypes in complete disregard of individual merit and fundamental freedoms. An inferiority complex coupled with external pressures and self imposed demands, subconsciously coerce individuals into a vicious cycle of desire or rejection. Active and aggressive media has played a key role in forming societal perceptions of what is attractive and desirable. In addition, lifestyle changes reflect an image obsessed culture, reeking of deep-rooted insecurities. At the root of a submissive and conformist attitude lies a subconscious mind lacking selfesteem and self-worth. People continue to look for remedies in the wrong places. The only difference is that corsets and blot letting have given way to surgeries and cosmetic products. The biggest question is, how have ideas otherwise seen as deviant, problematic and inadequate retained control over minds of millions of individuals?
A Gendered Culture
‘Beauty’ is understood as a process of ongoing work and maintenance, its ‘need’ unfairly tilted towards the fairer sex. History has demonstrated the impact of dangerous beautification practices on women. Contemporary ideals aren’t far from reaching similar outcomes. Today, there is a powerful drive to conform to the pornographic ideal of what women should look like. There has been a growth in the number of adolescents who take to cosmetic surgeries to become more ‘perfect’. In many countries, the growth of the “mommy job” has provoked medical and cultural controversies. Presumably there is an underlying dissatisfaction which surgery does not solve. Furthermore, where does the disability dimension fit in here? What happens to the ‘abnormal’ when the new ‘normal’ itself is skewed? For those with dwarfism and related disorders, new norms become even more burdensome.
The massive pressure to live up to some ideal standard of beauty, particularly for women, reeks of patriarchal remnants of a male dominated society. This kind of conformity further nurtures objectification and sexualization, reducing women to the level of ‘chattel’ to feed the male gaze. There is a also a power struggle at play where biased standards help maintain the unequal status quo. Today, there is idolization of celebrities, beauty pageants and advertisements by cosmetic companies over sane medical advice. They set parameters of size, color and texture to be followed by the world at large. Moreover, people who deviate from such norms are made to feel stigmatized or ostracized from social spheres. The existence of male-supremacist, ageist, hetero sexist, racist, class-biased and to some extent, eugenicist standards reflect a failure of society as a whole. It is thus high time that we revisit and deconstruct skewed standards of beauty.
Mind Over Matter: Psychological Dimensions
Culturally imposed ideals create immense pressure of conformity. Consequently, they have been successful in engendering insecurities via their influence on perception of self and body image. Such perceptions often become distorted and discordant with reality, leading to serious psychological disorders. One such disorder is the body dysmorphic disorder (BDD). This is a psychiatric disorder characterized by preoccupation with an imagined defect in physical appearance or a distorted perception of one’s body image. It also has aspects of obsessive-compulsiveness including repetitive behaviors and referential thinking. Such preoccupation with self-image may lead to clinically significant distress or impairment in social and occupational functioning. With reference to cosmetic surgeries, patients with BDD often possess unrealistic expectations about the aesthetic outcomes of these surgeries and expect them to be a solution to their low self-confidence. Many medical practitioners who perform cosmetic surgery believe themselves to be contributing towards construction of individual identity as well. The notion that beauty treatments can act in much the same way as psychoanalysis has led countries like Brazil to open its gate of cosmetic procedures to lower income groups. This happens while the country continues its battles with diseases like tuberculosis and dengue. The philosophy behind such ‘philanthropy’ is that ‘beauty is a right’ and thus should be accessible to all social groups. While on one hand we may applaud such efforts of creating a more ‘egalitarian’ social order, on the other hand it is hard to overlook the self-evident undercurrents of social prejudice and capitalistic propaganda.
Medicalization of Beauty
Traditional notions of beauty embody a kind of hierarchy and repression which alienate individual agency and renders them as powerless victims. Such is the societal pressure which normalizes cosmetic procedures and subverts serious health effects. These include adverse effects due to cosmetic fillers like skin necrosis, ecchymosis, granuloma formation, irreversible blindness, anaphylaxis among others. Other dangers like heightened susceptibility to cancer and increased suicide rates. However, patients are often unaware of the risks which are hidden behind a veil of expectations and reassurances. Furthermore, quackery and inadequate standards such as lack of infection control also compound the problems of this under regulated field.
Role of Stakeholders
At the heart of any successful social transformation lies the power of united will and collective action. Thus, the consolidated and sustained effort by all stakeholders is the key to realizing an ecosystem conducive to tackle negative social norms. At the outset, government regulation is needed with respect to cosmetic procedures and the cosmetics industry. These regulations should encompass all private and public avenues and should also work against misleading advertising. Spreading awareness is the key to a better informed society. The state should fund and run specialized awareness sessions pertaining to psychological problems and aid mechanisms, gender sensitization as well as those aiming at spiritual and introspective personal development of individuals. NGO’s, medical professionals, academicians and members of the civil society, must come together to eradicate forms of social discrimination which undermine social institutions and individual agency around the world. This would help facilitate discussion, data collection, coalition building, and action that may eventually lead to behavioral changes.
Aesthetic surgery today seems to be passing through an ethical dilemma and an identity crisis. And rightly so for it strives to profit from an ideology that serves only vanity, bereft of real values. Nevertheless, there are exceptional cases where medical-aesthetic inputs have been vital in restoring morale by subverting stigmatization.
The Way Ahead
Beauty is unfair. The ‘attractive’ enjoy powers gained without merit. The perfectionist in humans seeks outward validation of external beauty over inner virtues. Scientific progress and an increase in human expertise to manipulate natural phenomena has paved the way for these desires to become a reality. There is no denying that advances in plastic and reconstructive surgery have revolutionized the treatment of patients suffering from disfiguring congenital abnormalities, burns and skin cancers. However, the increased demand for aesthetic surgery falls short of a collective psychopathology obsessed with appearance. This article expresses trepidation about such forms of social consciousness that first generates dissatisfaction and anxiety and then provides surgery as the solution to a cultural problem.
We have to work towards a social order which embraces people as they are and facilitates free choice, individual liberty and informed decision making. This is particularly pertinent when these decisions work towards framing cultural perceptions and expectations for millions around the world. We should open our hearts to diversification of beauty and aesthetic. Let our entertainment, fashion, capital and media revolve around heterogeneity of ideologies and cultures. In the words of Eleanor Roosevelt, “No one can make you feel inferior without your consent”. So, let us all come together and create a better society. A society, where principles of justice, equity, good conscience and humanity override primitive and archaic ideologies of naive men. A society where individual will be truly free and, discourse a product of informed thought.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Dermatology & Cosmetics please click on: https://juniperpublishers.com/jojdc/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/jojdc/JOJDC.MS.ID.555556.php
31 notes
·
View notes
Text
Typhoid Fever, a Public Health Problem in Hospitals : Case Study at a Work station in Kinshasa, DR Congo-Juniper Publishers
Juniper Publishers- Juniper Online Journal of Public Health
Abstract
This study focuses on typhoid fever in its public health aspect. It is a driving force in admissions to hospital. It affects more adults who are part of the staff of health establishments in Kinshasa in the DRC. Our clinical picture was dominated by headache (25%), fever, insomnia and cough (12.5%), asthenia, abdominal pain (8.4%), and the dissociation of Pulse and temperature, vomiting and hypertension (4.2%). Our study shows that workers assigned to collection-sorting until disposal of care waste are sick of typhoid on their workstation.
Keywords: Typhoid fever; public health; Case study; Kinshasa (DRC)
Introduction
Human health has several factors that cause its evolution to be linked to several factors such as physiological, moral, armed conflict, expansion of several diseases and degradation of the family environment in society. Migration, displacement of populations especially in developing countries are factors that underlie various diseases. These diseases worry physician researchers and their work teams. Typhoid fever is common in several countries of the world and is common in countries with low levels of hygiene. It is endemic and poses a significant public health problem. According to statistics, there are 21,000,000 cases per year and 200,000 deaths worldwide [1]. In developing countries, the incidence is 540 cases per 100,000 or 0.2 cases / 100,000 in temperate countries [2]. In high-income countries, typhoid fever is contracted while traveling abroad. It quickly eradicates because the living conditions are better and the health system is also better. Moreover, given its climatic conditions, the living standards of the inhabitants and other endogenous factors, Africa is not immune to the spread of typhoid fever.
Man is the only reservoir of viruses because contamination is by water, food because in the most affected areas children, adolescents and even adults are the first carriers of this virus. Since the 1990s, the incidence of antibiotic-resistant Salmonella typhi has increased rapidly in the Indian continent, South Asia, sub-Saharan Africa [3]. Man is then the chronic carrier and plays an important role in the transmission of the disease. He may lodge it and excrete it in the stool. So we call it a disease of the hands rooms. The literature shows us that this disease is a public health problem but we do not have national statistics in DR Congo. This pathology is endemic [4].
For example, Mr PARENT studied typhoid fever in Lubumbashi (eastern DRC). In Kinshasa in 1977, Omanga conducted a study in children. In 2008, an epidemiological study of adult typhoid fever in the city of Goma in eastern DRC on 57 cases from January to December 2008 [5]. The bacteriological and epidemiological aspects of salmonellosis were observed at the University Clinics of Kinshasa (CUK) in 1968 by Gatti [6].
Some Concepts
Salmonella are enterobacteria that do not ferment lactose and aid in the non-production of urease. They are parasites of man, rodents, poultry and reptiles. As a result of oral penetration, salmonella (single-cell species) are the basis of typhoid fever, gastroenteritis and Food-borne infections. Typhoid fever is a bacterial infection caused by Salmonella enteria serotypes Typhi and Paratyphi (A, B, C). It is a mesenteric lymphoma starting point and is caused by four antigenically distinct human Salmonella servers but of similar pathogenicity These Salmonella are called major because of the seriousness of the pathology they cause.
From the point of view of Pathophysiology and biological diagnosis, Salmonella are integrated with a contaminated drink or food. The infective dose would be 105 bacteria. They are evidenced by haemoculture and / or by coproculture, and / or by demonstration of specific antibodies by indirect diagnosis. The serodiagnosis of WIDAL and FELIX detects the presence in the blood of antibodies directed against the constituents of Salmonella [7]. As for preventive treatment, it is based on general hygiene and TAB vaccination of specially exposed populations such as military personnel and hospital staff. From a curative point of view, treatment is based on antibiotic therapy (use of chloramphenicol followed by fluoroquinolones and cotrimoxazole) [8].
Public health is a study of the physical, socio-cultural and psychosocial determinants of population health and actions to improve the health of the population [9]. Other authors define public health as a science and the art of preventing disease, prolonging life and promoting health. The ultimate objective is to enable each individual to enjoy his or her innate right to health and longevity [10,11]. Unlike medicine, public health rests on two levels; On the one hand, it emphasizes prevention rather than curative treatment and on the other hand it develops a population approach [12].
Case study in this article concerns the workers and not the nurses of the four hospital structures in Kinshasa (CUK, Kinshasa University Clinics, HGRK, Kinshasa General Reference Hospital, HGK, Kintambo General Hospital and HGRN, Reference of Ndjili or Sino-Congolese hospital) in DRC ongo allocated to the management of hospital waste. As a result of our observations, we define hospital waste as a collection of household waste (DAOM) and infectious-care waste (DASRI) as shown in the attached photos. Our primary objective is to review the clinical signs associated with typhoid fever on this target population. One way to make an inventory during a fixed period of the presence of this disease of the hands rooms in this workstation. Far from us to see, the epidemiological aspects, but we will insist on the prevention of the diseases associated with typhoid fever.
Materiel and Method
This study of prospecting and research-action concerns 80 suspected cases of typhoid fever following various clinical signs observed in the exercise of their function in 2006. These are the general signs (fever, asthenia, dissociation of the pulse and temperature); Digestive signs (abdominal pain, diarrhea,vomiting); Neurological signs (headache, dizziness, insomnia); Respiratory signs (cough, Ronchi) and other signs such as high blood pressure and angina (Figure 1)
Case follow-up began in 2008. The dossier must meet the following criteria:
Be between 30 and more (often the men are assigned to this work door)
Present the general, digestive, neurological, respiratory and other signs mentioned above
Find in the stools, urine, blood, cerebrospinal fluid the seed sought.
A total of 272 workers or interviewers (141 at the CUK, 69 at the HGRK, 35 at the HGRN and 27 at the HGK) are assigned to this position. We chose 20 per hospital, so we have a sample of 80 cases to follow. These cases were not chosen at random but more for their regularity at work and sometimes their seniority of the 80 agents, clinical signs were observed during the study, of 24 of them, 30% of the cases. Thus the 24 workers were followed and hospitalized in internal medicine of each place of work.
The elements related to our surveys show, when we observe the photographs, that there is a failure in hospital hygiene, individual and collective. Indeed, workers collect waste that is not sorted without protection. With their hands, they accompany the waste to their place of treatment. As the incinerator no longer works, the waste is put in a National Program, sanitation bin where they are burnt. This behavior is dangerous for the environment (pollution of the air, fauna and flora (Figure 2).
Mode of Contamination
The method of contamination in the 24 cases of 80 workers in our sample was indirect. On the other hand, the probability of direct contamination comes from the workplace. The clinical signs observed during the 2006 campaign Table 1 shows that the clinical signs of typhoid fever occur on 30% (24/80) of workers assigned to the collection and treatment of hospital waste in the healthcare setting. Some workers have a picture suggestive of typhoid fever others have been for a fever that has resisted against quinine, chloroquine, artemisin, and to antibiotic therapy. The length of time between the onset of the illness and the day on which we requested hospitalization was long of the 24 cases, 17 cases or 70.85% accepted their hospitalization in February 2007. Admission was motivated by the isolation of germs in the stools of workers complaining of digestive disorders. In a few cases the symptomatology was not suggestive of typhoid fever.
The microbiological diagnosis was selected on the basis of blood cultures, coprocultures, urocultures and biliculture. Thus, 15 haemocultures were performed in 17 patients, 16 positive coprocultures. S. typhi was isolated from 11 urocultures (only one allowed). It was demonstrated in the 17 patients. Associated conditions not mentioned here, such as intestinal parasitic infections, hookworm infection, amoebiasis, anguillulose have not been studied. Urinary tract infections have been associated with typhoid fever. The patients were treated with chloramphenicol monotherapy at 25gr. Antibiotics were administered as a combination. The average duration was 14 days. Progressive treatments were applied (Table 2).
Discussion
Worldwide annual estimates of typhoid are 17 million according to the WHO [13]. In our study of the sample of 80 staff members divided by 20 in four hospitals, there was an improvement on 12 of the workers for the 17 with recognized symptoms of typhoid. This study did not allow us to classify the epidemic as seasonal. However, the disease is linked to a defective hygiene and the predominance is masculine because in the collection of waste and discarded, it is the men who are affected. The statistical study of the clinical symptoms compared according to the authors on 208 cases, we also demonstrate the persistence of the same symptoms to date. Fever took the lead with 89.9% of the 208 cases studied [4].
In this case, typhoid fever is predominantly an adult disease and urban origin predominates. The mode of direct contamination illustrates the fact that paramedical personnel (workers) are affected. Fever that does not respond to antimalarials or antibiotics is a reason for hospitalization as well as permanent headaches. Improved indicators of typhoid for 70.85% of patients or sufferers is effective. Patients are advised to wash their hands after each treatment. Similarly at home, they should take boiled water disinfected if possible with chloramines. Public health interventions to prevent typhoid require that health education be emphasized in terms of worker hygiene (hand washing at work, during meals, etc.), sanitation systems (Such as appropriate gloves, boots, overalls, glasses, etc.), to ensure that appropriate clothing is used in the handling of hospital waste.
Conclusion
This study is a development of this condition within healthcare institutions as regards the management of hospital waste. Measures to combat typhoid in hospitals include education and awareness in a healthy way of treating hospital waste from collection, sorting through treatment. It is recommended the use of appropriate treatments, antibiotics or vaccine use (does not provide definitive protection) available to those who work or are exposed to high-risk areas. Let us also not forget that the DRC is in Africa, which is an area at risk where the population is confronted with the highest burden
For more articles in Juniper Online Journal of Public Health please click
on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
0 notes
Text
Severity of Hip Displacement in Relation to Subtypes and Motor Function in Cerebral Palsy- Role of Hip Surveillance | Juniper Publishers

Juniper Publishers-Open Access Journal of Orthopedics and Rheumatology
Authored by Kunju PAM
Abstract
Background: Hip dislocation in children with cerebral palsy (CP) is a common and often over looked problem by the treating pediatricians. Though it can be diagnosed early by using radiographs, knowledge about the standardized methodology and need for periodic surveillance is lacking among primary care pediatricians. Hip surveillance by X-ray pelvis can identify early hip dislocation and it is shown that early intervention may prevent the need for surgery [1].
Methods: The study was done in a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs. One hundred and one children with CP formed our study population.Clinical evaluation for details regarding CP type and assessment of motor ability by gross motor function classification system (GMFCS) was done. A hip X-ray was done for calculation of, migration index for establishing or ruling out hip displacement. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results: There were 48 boys and 53 girls (mean age 4.80 years). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Out of 36 hemiplegic CP only one had MP > 40. out of 6 children with spastic quadriplegia, 5 (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed MP >40% in 9 out of 43 and 7 out of 16 respectively.According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Conclusion: All the children in this study did not undergo a hip X-ray prior to this study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia; Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement and hemiplegia had very low risk. According to the gross motor function classification system,GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40%. The study showed the relationship between the CP subtypes and the severity of the motor involvement. It also emphasized the need for early hip surveillance.
Keywords: Hip dislocation; Cerebral palsy; Lateral Displacement; Hip surveillance
Introduction
In children with spastic cerebral palsy reduced activity of the hip abductor muscles in comparison to the spastic adductors leads to diminished growth of the greater trochanter of femur results in pathologic deformities of the hips-femoral anteversion and coxa valga antetorsa [2]. If untreated, dislocation of the hip typically occurs at age 2–7 years with a maximum at the age of 6 years. The incidence of hip displacement in cerebral palsy is related to the severity of involvement; varying from 1% in children with spastic hemiplegia, up to 75% in those with spastic quadriplegia [2,3]. So periodic evaluation of hip function is essential for early intervention and preventive measures.
Hip surveillance is defined as: “The process of monitoring and identifying the critical early indicators of hip displacement” [4].Hip displacement refers to the displacement of the femoral head laterally out of the acetabulum and is measured using a migration percentage (MP). Hip subluxation refers to hip displacement where the femoral head is partially displaced from under the acetabulum while hip dislocation refers to hip displacement where the femoral head is completely displaced from under the acetabulumn [5,6].Hip surveillance is important, to prevent morbidity of spastic hip disease-The aim of the management in children with spastic hip displacement is to maintain flexible, well-located and painless hips with a symmetrical range of movement. The key to achieving this goal is early identification and intervention.
Periodic hip surveillance also helps to reduce the need for extensive surgical procedures which is highly specialized area of orthopedics which may not be available in every center. So primary care pediatrician has a role for hip surveillance and timely referral.
Patients and Methods
The study was done in a pediatric neurology department of a tertiary care hospital as a onetime radiological evaluation of children with CP between the age group of 4-9 yrs prior to the referral to orthopedics. One hundred and one children between the age group of 4-9 yrs. with the diagnosis of CP formed our study population.A pediatric neurologist and physiotherapist in the department examined the children and completed an assessment form. Clinical evaluation for details regarding CP subtype and assessment of motor ability by gross motor function classification system (GMFCS) [6] was done. Winters, Gage, Hicks (WGH) gait type was determined, in addition to inquiring regarding pain during history taking. Orthopedic consultations done whenever required.
Radiographic Examination
Decision for referral for surgery depends on the degree of displacement of the femoral head and acetabular dysplasia. The migration percentages as described by Reimers and the acetabular index described by Hilgenreiner are the conventional measurements of displacement of the hip and acetabular dysplasia in young children with cerebral palsy.Radiographic assessment consists of measurement of migration percentage (MP) from a supine AP pelvis radiograph with standardized positioning [7] (Figure 1). Reimers Hip Migration Percentage is the percentage of body width of femoral capital epiphysis displaced out of the acetabulum (which falls lateral to perkins line) [8].Measurement of migration percentage of femoral head was done as given in the (Figure 2).
In the adult or older child, where the triradiate cartilages are fused and therefore inapparent, the inferior margin of the pelvic teardrop is used instead.The acetabular angle using Hilgenreiner’s line should be less than 28°at birth. The angle should become progressively shallower with age and should measure less than 22° at and beyond 1 year of age.
Present study an anteroposterior (AP) pelvic radiograph at the time of first visit was done. Any decrease in the range of movement at the hip or presence of scoliosis was a definite indication for further detailed radiological examination & immediate referral. In the present study 101 children were assessed between 4 and 9 years of age. Children with MP > 33% and > 40% were compared in relation to those with MP below these limits. Migration percentage (MP) in relation to CP subtypes and GMFCS grades were done.
Results
There were 48 boys and 53 girls (mean age 4.80 years). Distribution of Cerebral Palsy sub types were as follows. Hemiplegic 36 (35.64%), Quadriplegic 6(5.94%), Diplegic 43(42.57%) and Choreo athetotic 16(15%). 12 children were Gross Motor Function Classification System (GMFCS) level 5, while 26 were GMFCS level 4. Results of hip displacement by radiography as measured by MP in relation to CP subtypes and motor severity are presented in (Tables 1&2) and (Figure 3).
Only one child out of 36 children with spastic hemiplegia developed MP > 40%. The maximum number of hip displacements was seen in children with spastic quadriplegia, where 5 of 6 children (83%) had MP > 40%. Spastic diplegic and choreoathetotic subtypes showed intermediate risk of hip displacement (9 out of 43 and 7 out of 16 respectively had MP >40%). In the present study onset of hip displacement could not be assessed as hip surveillance was not done in a periodic basis. Figure 4 shows x-ray hip of 4-year-old with very minimal displacement (MP 33.33%) and Figure 4 shows severe hip displacement in an 8-year-old child.
According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Discussion
The natural history of spastic hip disease of CP is progressive lateral displacement of the hip secondary to spasticity and muscle imbalance in the major muscle groups around the hip. Displacement may progress to severe subluxation, secondary acetabular dysplasia, deformity of the femoral head, dislocation and painful degenerative arthritis [4,5]. The long-term effects of dislocation of the hip can be disastrous for individual patients leading to pain and loss of the ability to sit comfortably in up to 50% of cases [6]. Other problems include difficulty with perineal care and personal hygiene, pelvic obliquity and scoliosis, poor sitting balance and loss of the ability to stand and walk [7-11].
A hip is usually considered to be subluxed,if the migration is equal to or greater than 33%. Reimers [17] found that among normal, the 90th gentile for migration percentage at four years was 10% with spontaneous migration of less than 1% per year. An unstable migration percentage is when progression is greater than or equal to 10% over 1 year [12-16]. Present study has shown that even a single radiological evaluation could identify hip displacement in children after the age of 4 yrs. Majority of (5 out of 6) quadriplegic CP, had severe type of hip displacement compared to hemiplegic CP (1 out of 36). Compared to other bilateral types of CP diplegia had lower rate of hip displacement (9 out of 43). This may be because of the less motor function impairment. So GMFCS may be a better predictor for early prediction of hip structural impairment. It is seen that there is direct correlation between the GMFCs class and severe hip displacement. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40% compared to only 4.76% in GMFCS I and II put together.
Subtyping of CP may have a role in predicting occurrence of severe hip displacement as shown by the almost complete occurrence in quadriplegic CP. However, a mere clinical examination and subtyping will not help in identifying severe hip disease in other type of CP. So, a systematic analysis of GMFCS is required for intensified screening of hip dysfunction. Moreover, as described in various guide lines periodic hip surveillance is mandatory for better ambulation and avoidance of surgery. This can be attained by early intervention measures. Figure 4 itself shows the importance of early surveillance. AACPDM - (American Academy for Cerebral Palsy and developmental medicine) recommends following schedule of hip surveillance (Table 3).
Conclusion
Need for hip evaluation in children with CP is emphasized by this study. All the children in this study did not undergo a hip Xray prior to the study. 22 out of 101 children had severe degree of hip displacement. The maximum number of hip displacements was seen in children with spastic quadriplegia and hemiplegia had very low risk. According to the gross motor function classification system, GMFCS level I had no child with MP > 40%. Whereas 50% of children in GMFCS level IV and V had MP > 40 %. The study showed the relationship between the CP subtypes and the severity of the motor involvement in producing hip displacement. Referral to an orthopedic surgeon with experience in treating hip displacement in children with CP is recommended when there is presence of hip pain on history and/or physical examination. Periodic hip surveillance is mandatory for early detection of hip displacement. When the migration percentage is greater than 30% and/or there is less than 30 degrees of hip abduction with or without other findings, referral to an orthopedic surgeon is recommended [1,17].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Orthopedics and Rheumatology please click on: https://juniperpublishers.com/oroaj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/oroaj/OROAJ.MS.ID.555848.php
50 notes
·
View notes
Text
Non-Invasive Glucose Monitoring: Application and Technologies | Juniper Publishers
Juniper Publishers-Open Access Journal of Diabetes & Obesity
Authored by Ghozzi Dorsaf
Abstract
The chronic metabolic disorder, diabetes mellitus is a fast-growing global problem with huge social, health, and economic consequences. The prevailing method for determination of blood glucose concentration is using a self-monitoring glucose meter. Most of the commercially available devices for glucose measurement are invasive or minimally invasive. Invasive devices used for blood glucose monitoring are painful whereas minimal invasive devices have limited time span and stability. Thus, there is a need of an economic, compact, painless and convenient non-invasive device which can promote frequent blood testing which help in control of blood glucose level. There have been numerous developments in the field of non-invasive glucose monitoring NGM during the last decade, which stress the need for a critical review. This manuscript aims to review the various NGM techniques and application. The limits and future trends in NGM are also discussed.
Keywords: Non-invasive glucose monitoring; Diabetes; Technology; Application
Introduction
The prevalence of diabetes is constantly increasing worldwide at an alarming rate. According to the International Diabetes Federation in 2015, an estimated 415 million people globally were suffering from this condition [1]. Currently no treatment exists or is under development which could possibly cure this illness in the near future. The therapy of diabetes mellitus so far consists in monitoring the blood glucose (BG) level of a patient to avoid the danger of hypo- and hyperglycemias and to assist in adjusting the diet and medical treatment.
Self-monitoring of BG concentrations has advanced over the past few years. Glucose values determined by home meters correlate well with laboratory results. Because of the importance of precision and accuracy of self-monitoring BG devices, guidelines for the performance of these devices were recommended in 1987 by the American Diabetes Association [2]. Almost all commercial blood glucose monitoring devices (BGMD) employ a cost-effective electrochemical biosensor, which is capable of being mass produced and responding rapidly to glucose detection. They use automatic lanced devices to prick the fingertip of diabetics has to measure blood glucose very frequently. There have been tremendous developments in the last few decades to develop improved BGMD [3] with reduced blood sample requirement of less than 1μL. The painful aspect are minimized by employing alternate sampling sites (hand, arm). However, the cost of strip and the boredom of making repeated measurement are becoming most important. The minimally invasive approaches have been developed by using subcutaneous sensors to determine glucose concentration in interstitial fluid. But they suffer from limitations in terms of discomfort to patients, requirement of continuous calibration, and high susceptibility to biofouling. Therefore, the development of NGM techniques [4,5] is the only way to develop pain-free glucose monitoring technology for diabetics. This is the major stimulant for continuous ongoing developments in the field of NGM. There have been continuously increasing number of publications in NGM (Figure 1).
The developments undertake to improve the way of measuring the BG depend on several parameters such as the reading accuracy, techniques and approach, size of the device, and technology of the embedded systems. Each of this generation will be discussed.
The recent development of the BGMD is more toward noninvasive method. This method is used to measure BG levels in the human body by only placing the sensors directly to the human targeted area without drawing blood and insertion of needles or any types of biosensors. The study on the development of this technology has begun since 1957 and the works are still continuing up to the present. Since 2014, only a few numbers of devices that have been produced using this technology and they are only available in certain countries. Most of the non-invasive BGMD is registered under consumer product and not under a medical product because this device reads the value of the blood glucose without directly in contact with the blood.
This manuscript provides an update of various potential NGM technologies and devices along with their advantages, limitations. The goal of this study is to provide an update of various potential NGM technologies and devices along with their advantages and limits. In section II non-invasive glucose monitoring technologies have been discussed, while section III discusses the proposed NGM application, and section IV discusses technology versus application. Conclusions and future developments have been illustrated in section V.
Non-Invasive Glucose Monitoring: technologies
Non-invasive methods for glucose monitoring are more desirable and excellent alternatives to the above-mentioned technologies [6]. This could make millions of people more relaxed and comfortable about regular blood glucose testing. Although many research works have already been carried out in this area, the search of a successful non-invasive technique continues [7]. The order of presentation is partially arbitrary: we tried to report first those technologies more known, used and described.
Near infrared spectroscopic
It is a spectroscopic method which uses radiation in the near infrared (NIR) region of the electromagnetic spectrum (750-2500nm) [3,4]. There are mainly three bands in NIR range: combination overtone band (2000-2500nm), first overtone band (1400-2000nm) and second or higher overtone band (750- 1400nm). It allows the glucose measurement under the skin to a depth of few mm in range. The penetration of light into the skin decreases with the increase in wavelength [5]. As the light interacts with tissue, it is partially absorbed and scattered due to interaction with chromophores within the tissue [8]. The combination and the first overtone regions are dominated by glucose absorption information while shorter wavelength region mainly carries scattering information [9]. NIR light transmission or reflectance has been studied through an ear lobe, finger web and finger cuticle, skin of the forearm, lip mucosa, oral mucosa, tongue, nasal septum, cheek, and arm.
NIR diffuse reflectance measurements performed on the finger showed a correlation with BG but predictions were often not sufficiently accurate to be clinically acceptable [10]. The technique has serious limitations as it is affected by physicochemical parameters such as changes in body temperature, blood pressure, skin hydration, and concentrations of triglyceride and albumin. Moreover, it is sensitive to environmental variation in temperature, humidity, atmospheric pressure and carbon dioxide content. The measurement are also affected by the thickness and thermal properties of the skin [11,12], and the disease states such as hyperglycaemia and hyperinsulinemia [13,14].
Mid-infrared spectroscopy
Mid-infrared (Mid-IR) spectroscopy is based on light in the 2500-10.000nm spectrums [15]. The physical principle is similar to that of NIR. When compared to NIR, however, due to the higher wavelengths, Mid-IR exhibits decreased scattering phenomena and increased absorption. For this reason, the tissue penetration of light can reach a few micrometers [16] in the case of human skin, that corresponds to the stratum corneum. As a consequence, only reflected, scattered light can be considered: there is no light transmitted through a body segment. On the other hand, a possible advantage of Mid-IR compared to NIR is that the Mid-NIR bands produced by glucose, as well as other compounds, are shaper than those of NIR, which are often broad and weak.
Mid-NIR is less studied technique compared to NIR for glucose measurement, probably due to the strong limitation in penetration. Studies are reported related to finger skin and oral mucosa [17]. One strong limitation is the poor penetration. Furthermore, Mid-IR is a affected by similar problems and confounding factors than NIR, despite glucose bands potentially improved for instance, some studies have shown significant dependence of skin Mid-IR spectrum on its water content [16]
Raman spectroscopy
Raman spectroscopy used laser radiation source from visible to Mid-IR, when some portion of scattered light shows a different wavelength from that of excitation beam, the effect is known as Raman effect. When scattered light has a higher wavelength and lower intensity (10-3 times) than the original signal shown in (Figure 2).
Optical coherence tomography
The optical coherence tomography (OCT) allows the real time and precise non-invasive glucose monitoring. OCT uses low coherence light source, an interferometer and a photo-detector to measure the interferometric signal. The interferometer consists of reference arm, sample arm and a moving mirrors. Light returned from the reference part of the interferometer is combined with the backscattered light from tissue. The resulting interferometric signal is detected by a photo-detector. The delay in back scattered light or the changes in scattered light due to variation in glucose concentration is used for measurement of blood glucose [18,19].
Bioimpedance spectroscopy
The first study of non-invasive continuous glucose monitoring system involving impedance spectroscopy was published by Cadduff’s group in 2003. As result from this research, the company pendragon developed a wrist glucose monitor called Pendra. The equipment gatherers information of a LC resonance circuit from 1MHz until 200MHz, with the skin working as dielectric from the capacitor. One limitation of this research is that it requires an equilibration process, where the patient must rest for 60min before starting measurement [7].
Fluorescence spectroscopy
This technique is based on the generation of florescence by human tissues when excited by lights at specific frequencies. In the case of glucose, one study demonstrated that when a glucose solution is excited by an ultraviolet laser light at 380nm, fluorescence can be detected at 340, 380, 400nm, with maximum at 380nm [15]. It was also proved that fluorescence intensity was dependent upon glucose concentration in the solution. Also light in the visible spectrum can be used, but this is more adequate for studying fluorescence of tissues rather than that of solutions. In tissues, the use of ultraviolet light could lead to strong scattering phenomena, in addition to fluorescence. Moreover, even when using different wavelengths, the fluorescence phenomenon can depend not only on glucose, but on several parameters, such as skin pigmentation, redness, epidermal thickness [6].
Non-Invasive Glucose Monitoring: Application
GlucoWatch®
The first commercial U.S. Food and Drug Administration (FDA) approved non-invasive glucose monitor was the GlucoWatch® biographer (Cygnus Inc.). This wrist worn system electrochemically measured glucose concentrations in skin interstitial fluid (ISF) extracted by reverse iontophoresis (RI) [23-24]. The GluoWatch® electrochemically detected levels of extracted ISF glucose through enzymatic glucose oxidation at skin-worn sensing electrodes modified with glucose oxidase (GOx). The GlucoWatch® had a user-friendly interface that included an alarm for greater than 35% changes in glucose, an activity marker (for meals, exercise, and insulin injection), accompanying software for data analysis and internal memory to store up to 8500 readings [20,21]. Clinical trials of the GlucoWatch® showed adequate precision for home bloodglucose monitoring. The Cygnus GlucoWatch was marketed in the early 2000s but was retracted from the market due to various reasons, which included reported skin irritation caused by the RI process, the long necessary warm up time (2-3h), and the need for calibration using standard blood glucose strips. To address these drawbacks, recent research efforts have focused on producing reliable, efficient non-invasive glucose monitoring platforms.
Tattoo-based glucose sensor
Wang et al. recently developed a wearable, tattoo-based non-invasive glucose monitoring platform based on integrating RI with amperometric glucose detection on a flexible substrate [22]. The iontophoretic and glucose sensing electrodes were fabricated on a single temporary tattoo platform using screenprinting, leading to a body-compliant and easy to wear flexible, conformal device for single use glucose measurements. This sensing platform obviated the discomfort of Glucowatch® by reducing the applied iontophoretic current for ISF extraction and by utilizing a low voltage cathodic detection of the GOxgenerated hydrogen peroxide at the Prussian Blue electrode transducer. The performance of the tattoo-based electrodes was evaluated with healthy human subjects by comparing the recorded glucose signals before and after meal, and the results were validated by simultaneous blood glucose measurement using a commercial glucometer. Control experiments were carried out without enzyme modification of the glucose sensor to confirm the sensing mechanism. Although the tattoo-based device was intended for disposable use, such a sensor holds considerable promise for continuous non-invasive ISF glucose monitoring by offering a body-compliant, flexible and costeffective platform. Future work toward the development of such systems should focus on the testing of performance over longterm use, sensor integration with wireless electronics, and examination with large populations of both healthy and diabetes suffering individuals.
Non-invasive sweat glucose monitoring
Sweat is a very attractive bio-fluid toward non-invasive, continuous monitoring applications due to its distinct advantages, such as having the most sampling sites outside the body, continuous access, an ease of collection device placement and comfort, as well as its composition of physiologically important electrolytes and metabolites [23]. Gao et al. demonstrated a flexible and fully integrated sensor array platform for multiplexed in situ perspiration analysis, measuring multiple sweat metabolites (glucose and lactate) and electrolytes (sodium and potassium) as well as skin temperature in a wearable patch type platform [24]. The reported device integrated signal transduction, processing and wireless transmission for the realization of a practical wearable sensor device.
D. Pendra
Pendra from pendragon medical ltd, Switzerland was another NGM device in the form of a wrist-watch, which based on impedance spectroscopy. It was approved by FDA in may, 2003 as an adjunctive device to standard blood glucose meters to detect trends and patterns in glucose levels [25]. It consists of an open resonant circuit (1-200MHz) that lies in contact with skin with the help of a tape on the backside of the device and performs the impedance measurements. It cans perform up to four measurements per minute with sensitivity in the range of 20-60mg dL-1 glucose per ohm. It has USB connectivity for downloading data to a PC, Pendra user software for data analysis. The correlation studies showed a poor correlation of only 35.1%. The production of Pendra was stopped as the company went bankrupt in 2005.
Application versus technologies
In this review, we presented a description of NGM. According to the indications of the health technology assessment (HTA) methodology, we carried out the analysis on the basic of clear and objective criteria. Some of the technologies have not been exploited in a device yet, while some others have led to a device at least in advanced prototype condition [26]. It must be noted however, that currently only three devices have reached a regulatory approval for commercialization in United States and/ or Europe.
Among these three, for different reasons two of them are not on the market anymore. The only available one is the GlucoWatch, and in any case it cannot completely substitute a traditional meter. Furthermore, GlucoWatch is reported to possibly have some drawbacks: in fact, it sometimes causes skin irritation, and it may be uncomfortable to use in the daily life of the patients.
The development of non-invasive glucose biosensors for diabetes management is just beginning. Despite promising recent advances, there yet remain numerous challenges to overcome for the successful implementation of non-invasive glucose monitoring technologies, combining accurate real-time glucose readings with long-term stability. In particular, largescale studies are required to critically assess the accuracy
A reliable means of efficient, selective fresh glucose uptake is crucial to the development of sweat-based monitoring systems. Further efforts should focus on accurate epidermal glucose measurements by combination with sensing of other physiological parameters (pH, temperature, humidity) toward continuous calibration and improved accuracy and correlation with blood glucose level. Future efforts should also aim at simultaneous monitoring of additional diabetes related markers toward a more comprehensive array of information regarding real-time glucose metabolism [27]. Further improvement in iontophoretic sweat stimulation is desired for controllable (consistent and reproducible) sweat generation without the need for exercise. Additional work should also focus on improved sweat collection, flow and replenishment in connection to epidermal flexible microfluidics devices. Overcoming these and other challenges will be crucial for the advancement of continuous epidermal glucose monitoring to realize its potential impact.
To achieve the targeted goals, a thorough understanding of all components of the non-invasive monitoring systems are required, including the applied technologies, skin physiology, device surface and material chemistries, and sensing electrochemistry as well as the interface of these systems. The successful realization of non-invasive glucose monitoring platforms require not only consideration of scientific problems, but also economic, legal and commercial concerns with the patient and physician education of key importance [28]. We envision that through a combination of these technological advances with large scale studies, glucose concentrations can be reliably and noninvasively monitored with minimal discomfort to patients for widespread applications toward improved glycemic control and autonomous therapeutic interventions through integration with autonomous, closed-loop insulin delivery systems. Given the rapid recent progress, it seems that non-invasive glucose monitoring has only scratched the surface of its full diagnostic potential and is poised to significantly increase its impact on medicine.
Conclusion
The non-invasive devices have tremendous appeal and a market in excess of at least one billion dollar per year worldwide. However, the development of non-invasive devices has been hampered by unsubstantiated claims, which proved to be misleading if not false. In conclusion, the problem of noninvasive glucose monitoring is currently not solved, and further efforts are still necessary to reach the goal of having a reliable and inexpensive device for the benefit of the diabetic patient.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Diabetes & Obesity please click on: https://juniperpublishers.com/crdoj/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/crdoj/CRDOJ.MS.ID.555740.php
24 notes
·
View notes
Text
The Effects of Anti-Fibrosis Drugs on the Self-Regulation of Alveolar Macrophages and Interstitial Macrophages in the Pathological Process of Pulmonary Fibrosis | Juniper Publishers
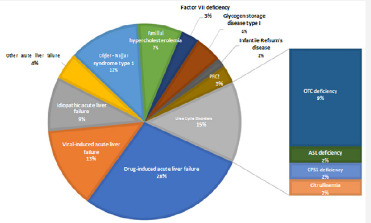
Juniper Publishers-Open Access Journal of Gastroenterology & Hepatology
Authored by Huaqiang Zhai
Abstract
Pulmonary fibrosis is a devastating condition with many kinds of inducements. Alveolar macrophages (AMs) and interstitial macrophages (IMs) are two subsets of macrophages which involve in the inflammatory reaction of pulmonary fibrosis. Traditional Chinese medicine has good effects on the treatment of pulmonary fibrosis. This review is aimed at summarizing the different roles of alveolar macrophages and interstitial macrophages in the pathological process of pulmonary fibrosis progression and anti-fibrosis drugs related to the self-regulation mechanism of these two kinds of cells, furthermore to explain the multiple mechanisms of traditional Chinese medicine for treating pulmonary fibrosis from the self-regulation of macrophages. Searches for keywords “alveolar macrophages”, “interstitial macrophages”, “pulmonary fibrosis” and “IPF” were performed in biomedical databases. The reported incidences of AMs and IMs in the pathological process of pulmonary fibrosis are involved in this article, and the influences of traditional Chinese medicine on the cells are summarized.
A comprehensive analysis of the literature confirms that alveolar macrophages appear to be better equipped for their antimicrobial task, whereas interstitial macrophages have more capacity for immune regulatory functions. Disease-modifying therapy for pulmonary fibrosis based on intervening the macrophages self-regulation relates to chemokines and cytokines. Traditional Chinese herbs for pulmonary fibrosis have different targets on the two kinds of cells. Alveolar macrophages and interstitial macrophages could be used to explore the pathological process and clinical medicine of pulmonary fibrosis, and they are conducive to interpret the multiple mechanisms of TCM for pulmonary fibrosis.
Keywords: Alveolar macrophages; Interstitial macrophages; Pulmonary fibrosis; Chemokines; Cytokines; Traditional Chinese medicine
Abbrevations: AMs: Alveolar Macrophages; IMs: Interstitial Macrophages; IPF: Idiopathic Pulmonary Fibrosis; TCM: Traditional Chinese Medicine; BALF: Bronchoalveolar Lavage Fluid; PDGF: Platelet-Derived Growth Factor; TNF-α: Tumor Necrosis Factor-Α; IFN: Interferon; TGF-β1: Transforming Growth Factor-Β1; CTGF: Connective Tissue Growth Factor
Introduction
Pulmonary fibrosis is a kind of chronic progressive interstitial lung disease. Idiopathic pulmonary fibrosis (IPF) is a common and devastating pulmonary fibrosis with no powerful drugs. Data showed the incidence of IPF seems to be increasing rates of 3-9 cases per 100000 a year, although varies worldwide [1]. The median survival was 2.5 to 3.5 years after the diagnosis of IPF [2]. The major clinical features of pulmonary fibrosis are symptoms of dyspnea, wheezing, dry cough, etc. and eventually leading to respiratory failure and death [3]. Current researches about pulmonary fibrosis more focus on anti-inflammatory, immunity, cytokines, genetic factors, etc. [4]. A small number of experiments were conducted at the level of molecules and gene [5-7]. The etiology of pulmonary fibrosis is varied, with an array of triggers including allergens, chemicals, radiation and environmental particles [4]. Such triggers are believed to impair the tight regulation of inflammation and repair, leading to excess production of collagen by fibroblasts and the subsequent formation of scar tissue [8]. However, the cause of IPF remains unclear [9].
It is vital that tissue architecture is restored to regain normal function. The early lesions of pulmonary fibrosis mainly appear in the alveolar walls accompanied by a large number of proliferated lung fibroblasts, causing extracellular matrix deposits in alveolar and interstitial excessively [10]. Then the repaired fibrous tissues result in structural disorder and replace the normal tissues [11]. The ultimate outcome is irreversible pulmonary fibrosis [12,13]. An important factor of pulmonary fibrosis occurrence is the function and number of AMs and IMs [14]. Analysis of the different roles of AMs and IMs in the pathological process of pulmonary fibrosis in the field will provide an explanation of the multiple mechanisms for treating pulmonary fibrosis with TCM.
Roles of AMs and IMs in the Pathological Process of Pulmonary Fibrosis
AMs and IMs are getting more and more attention in the treatment of pulmonary fibrosis. The basic functions of macrophages in the immune defence system are phagocytic and bactericidal activities, which is vital in resisting the invasion of pathogenic microorganisms. It is reported that AMs appeared to be better equipped for their antimicrobic task. Whereas IM, although also having antimicrobic potential, show a more pronounced capacity of immunoregulatory functions [15]. As the sole cell population exposed to air, AMs having phagocytic activity of clearing extraneous particles, which is the first barrier of the lung. AMs get damaged after phagocytizing the pathogenic particles, further cause lung damages. IMs in the lung tissue also play a very important role in inflammation and local immune defense reaction of the lung injury, which is the second barrier of the lung (Figure 1).
The form and number of AMs and IMs in the pathological process of pulmonary fibrosis
AMs and IMs are two critical subsets of macrophages. Pulmonary macrophages consist of AMs in the surface and internal of alveolar space, and IMs in pulmonary interstitial next to alveolar septa or next to bronchi and vessels. Normally, there are significant differences between AMs and IMs in morphology, structure, phenotype and function [16]. Under the light microscope, the diameter of AM is about (12.1±1.16) μm which is larger than that of IM with about (9.3±1.1) μm. AM is round or irregular while IM is round and uniform relatively in shape and size. AM HE staining shows the cytoplasm is pink with loose nucleus deviate to the side of the cytoplasm in an oval shape and the nuclear-cytoplasmic ratio is less than 50%. The surface of the AM is uneven with many protrusions and the cells contain more intracellular lysosomes. IM, HE is staining shows that the cytoplasm is dark red, with dense nucleus shape irregularly and the nuclear-cytoplasmic ratio is greater than 50% [17].
The surface of the IM is smooth with almost no protrusions and the cells contain fewer primary and secondary intracellular lysosomes. Differences between AMs and IMs in morphology and structure determine their differences in functions [18]. IMs only accounts for 3%-5% of the total number of various cells throughout the lung tissue, so the isolation of IM is totally a difficult task. Over 90% of the rat bronchoalveolar lavage fluid (BALF) samples are AMs, and a variety of cells including macrophages, neutrophils, endothelial cells and lymphocytes can be obtained by enzymatic dispersal of the lung tissue. Separated by the lymphocyte separation liquid and purified by adherent cell culture, 90% of the cells in culture liquid are IM cells. The number of AMs and IMs in lung tissues under normal physiological conditions is less than that of fibrosis pathological conditions. Studies have found that the number of AMs in BALF reached the highest level on the 7th day after bleomycin injection, and the number and HE stain intensity of positive AMs have reached its peak as well [19]. And AMs increased significantly in the BALF on the 14th and 30th day after Pingyangmycin injection, which is consistent with the pro-inflammatory and pro-fibrotic effect of AMs. The number of AMs on the 14th day of Pingyangmycin injection is more than that on the 30th day, which may relate to the serious inflammatory injury during the first 14th days. The number of AMs will continue to develop on the 30th day with the sustained progress of pulmonary fibrosis [20].
The cell function of AMs and IMs in the pathological process of pulmonary fibrosis
AMs and IMs in the lung are distributed in two different anatomical sites, which result in their different functions [21,22]. Located in the airways and alveoli, AMs are the only cell population exposed to air, which contributes to the first barrier of the lung to clear inhaled microorganisms during breathing [23]. The morphology of the permanent AMs in alveoli is changeable, while the AMs in normal lung tissues are similar to the mature macrophages of other organizations. The microvilli of normal AMs distribute on the cell surface uniformly. The cytoplasmic volume of normal AMs is large with a large number of lysosomes, phagosomes and enzymes [24]. Besides, normal AMs produce cell recruitment factors, active nitrogen and other factors, and result in macrophages and other inflammatory cells gathering. During acute inflammatory periods, AMs become larger and containing quantities of peroxidase with a diameter of 12μm, while they become mature and larger during chronic progress period with a diameter of 14-40μm. The cytoplasmic membrane of AMs under the electron microscope is irregular
The cytoplasm contains many mitochondria and lysosomes, and the nucleus is more leaflike. The expression and release of membrane receptors in AMs depend on different states. The main role of AMs is to kill pathogenic microorganisms, phagocytize water-soluble poorly organic particles, release inflammatory mediators, present antigens, and express different cytomembrane receptors at the same time. Many studies suggest that AMs are the key cells causing early biological effects on lung [25]. In the initial process of lung injury, cellular infiltration can also be found in AMs from the observation of lung tissue by biopsy. The degree of cellular infiltration is closely related to the degree of pulmonary fibrosis, which confirms that AMs have the function of promoting the inflammatory response. In the process of promoting inflammatory infiltration, it also increases lung damage and causes excessive repair of the tissues, then leads to fibrosis.
IMs also play a very important role in lung inflammation and local immune defence reaction. The IMs are a type of macrophages in the interstitial connective tissue forming the second line of the lung defence, which may have a greater immune function with its special location. But the location of IM can also make it difficult in extracting the cells. IMs in pulmonary interstitial contact with the extracellular matrix and other interstitial cells tightly thus affects pulmonary interstitial metabolism. IMs are often acquired from the pulping lung tissue digested by collagenase, but the separation methods reported in the literature are quite different. IMs have their own unique function and morphology compared with AMs. They have a smaller diameter of 6.6μm, a more folded cell membrane, irregular nucleus and larger nucleoplasm ratio. And the non-specific lipid stain results of them can be positive, less positive or negative.
The filar pseudopod of IMs cell can be seen under the electron microscope. The cytoplasmic membrane of IMs is pleated, and still not extended to its characteristics after cultivating for 24h. Because of the difficulty in getting IMs, more papers focus on the study of AMs. However, recent studies have shown that IMs may have a more important role in lung injury. As the important cells, IM’s ability to phagocytize particles, produce oxygen radicals and chemotactic complement is weaker than that of AM [15]. But IMs express more MHC II and they are more efficient in stimulating the proliferation of T cells [26].
The phagocytosis and secretory function of IMs are like that of AMs. Although the Fc receptor-dependent cellular phagocytosis capability of IMs is like that of AMs, the Fc receptor-independent cellular phagocytosis capability of IMs is lower than that of AMs significantly. So that IMs show more capable of respiratory immune responses. Existed in pulmonary interstitial, IMs can release inflammatory mediators and cytotoxic mediators, which may be a more direct cause of lung tissue damage [27]. There has also been reported that IMs make more sense in the progression of pulmonary fibrosis than AMs in biological behaviours and active effects [28]. More experiments should be carried out to confirm the function of IMs.
The relationship between AMs and IMs in the pathological process of pulmonary fibrosis
AMs and IMs are two critical subsets of macrophages, which are critical in the pathological process of pulmonary fibrosis process. From the perspective of cells occurrence, AMs are the ultimate development status of macrophages which come from the source of bone marrow monocytes. Blood monocytes grew into AMs in the development of end-stage, while IMs may be the transitional stage of that process [18]. But there are great differences between AMs and IMs in antigen presenting, cytokines secreting and other immune functions. And the effects of endotoxin attacks on them are discrepant. All the differences suggest IMs are not simply the precursor of AMs.
Evidence also shows that platelet-derived growth factor (PDGF) secreted by AMs cannot enter the alveolar interstitial through the epithelia completely. Therefore, it may be concluded that AMs located in the alveolar may have a stronger function of phagocytosis, and IMs in the interstitial are primarily related to the immune regulation. In vitro studies, Adamson found that short fibers (<1μm) and long fibers (> 20μm) asbestos could stimulate macrophages to produce the Fibroblast Growth cytokines. In vivo studies also found that AMs phagocytized almost all short fibers which did not enter the pulmonary interstitial without pulmonary fibrosis lesion when mice inhaled short asbestos fibers. While IMs were activated when the long fiber deposited on the bronchi furthered into the pulmonary interstitial and caused effectors accumulate in pulmonary interstitial. Then fibroblast multiplied quickly, eventually led to the formation of pulmonary fibrosis [29].
The Self-Regulation Mechanism of AMs and IMs in the Pathological Process of Pulmonary Fibrosis
Pulmonary fibrosis is characterized by the accumulation of fibroblasts. The deposition of inflammatory cells such as macrophages, lymphocytes, and granulocytes are also the hallmark of pulmonary fibrosis. The mechanisms responsible for the migration of fibroblasts and inflammatory cells to the lung in pulmonary fibrosis are not known, but cytokines and chemokines are essentially considered [30]. The self-regulation mechanism of AMs and IMs includes two parts: Firstly, the inflammatory factors stimulate macrophages and other immune cells to secrete chemokines [31], which allow AMs, IMs and other inflammatory cells to accumulate and release a large number of cytokines. Secondly, the release of cytokines stimulates myofibroblast, leading to the accumulation, proliferation and activation of fibroblasts, then pulmonary fibrosis occurs. By further activating signal transduction pathways at the same time, cytokines stimulate inflammatory cells to generate new cytokines and the process cycles [32] (Figure 2).
Chemokines assist in the migration and invasion ability of AMs and IMs
The CC family and CXC family are two big families of chemokines involving the pulmonary fibrosis. The transfer of fibroblasts and inflammatory cells in the lung requires the participation of various chemokines/chemokine receptors such as CXCL12/CXCR4, CCL21/CCR7, CCL2/CCR2, CCL3/CCR5 [32]. Many biological functions of macrophages play their roles in their cytomembrane mediated action. The cytomembrane receptors of AMs and IMs correspond with their specific binding ligand, triggering the cell signalling pathways. The binding force of the receptor on the cell surface and the number of receptors on the surface of the cytomembrane can affect the signal transduction [33,34]. Phagocytosis is one of the important functions of macrophages, and the interaction between effector cells and the membrane of the target cells is a key factor in macrophages to kill tumor cells [35].
Cell migration is an important reason for adjusting the number of cells. Monocyte chemoattractant protein-1 (MCP- 1) and macrophage inflammatory protein-1α (MIP-1α) (also known as CCL2 and CCL3) in-vivo are important chemokines participated in the chemotaxis of the cells, the main chemotactic cells and macrophages are concentrated in the inflammatory regions [36]. Studies have found that inhibiting the activity of MCP-1 and MIP-1α in the early pulmonary fibrosis can reduce the accumulation of alveolar macrophages [37]. MCP-1mRNA in the lung tissue of rats can be found mainly expressed in alveolar macrophages, airway epithelial cells in Bleomycin-induced pulmonary fibrosis rats [38]. Thus, MCP-1 alters the population of alveolar macrophages through recruitment of blood monocytes into the luminal airspace. MIP-1α can also mobilize the bone marrow monocytes into myeloid precursor cells and enhance the infiltration of macrophages in inflammation areas [39].
According to the general reasoning, the reason for the increase of AMs in the alveoli and IM in the pulmonary interstitial is likely to be under the chemotaxis of chemokines, blood monocytes cells infiltrate or migrate to the inflammatory sites and grow into the macrophages. The increased extent of AMs varies depending on the stage of the pulmonary fibrosis, while IMs increase more obviously in the early period. In vitro study of the macrophages migration and invasion chemotaxis of MCP-1 shows that MCP-1 can assist in the migration and invasion ability of macrophages. And the chemotactic efficiency of macrophages related to the concentration of MCP-1 [40]. The growing number of macrophages with enhanced invasion capability can contribute to the pathological process of pulmonary fibrosis.
AMs and IMs secrete cytokines to regulate fibroblasts and regulate cytokines secretion
Macrophages are gathered and activated under the chemotaxis of chemokines. AMs secrete platelet-derived growth factor (PDGF) and transform growth factor beta (TGF-β), which can promote the accumulation, proliferation and activation of fibroblasts in lung injury area, causing the extracellular matrix accelerating the synthesis. It can also increase fibroblast by increasing the transfer and adhesion of osteopontin, resulting in pulmonary fibrosis [41]. AMs secrete tumor necrosis factor-α (TNF-α), interferon (IFN), transforming growth factor-β1 (TGF-β1) and other active media that can anti-pathogenic microorganisms strongly, which can effectively kill the pathogens invaded the body. IMs have lower ability to produce these cytokines than AMs, while the ability to secrete cytotoxic medium and interleukin (IL) are high, which cause more direct damages to lung tissue and show higher MHCII class antigen expression activity and stronger supplementary ability.
Cytokines regulate fibroblasts and macrophages involved in a variety of signal transduction pathways such as the MAPK pathway, JAK-STAT pathway, Smad pathway, PI3K-Akt pathway, NF-κB pathway, etc [42]. TGF-β1, a powerful fibrosis cytokine, rely on Smads and MAPK signal transduction pathway to regulate lung fibroblasts to muscle fibroblasts, produce a large number of extracellular matrix proteins, and lead to pulmonary fibrosis [43]. IL, TGF-β1, IFN involved in the JAK-STAT pathway to regulate the proliferation of fibroblasts by regulating the gene expression. At the same time, cytokines further activate the signal transduction pathways and stimulate AMs and IMs to produce new cytokines. TNF-α stimulates MAPK/ERK pathway, increases transcription of the TGF-β1 Gene and stabilizes TGF-β1mRNA to induce the expression of TGF-β1 [44,45]. On the other hand, TNF-α activates NF-κB pathway to accelerate the new TNF-α secretion of macrophages [46]. The upgraded cytokines create new biological effects.
Disease-Modifying Therapy for Pulmonary Fibrosis Based on Intervening the Self-Regulation of AMs and IMs
Clinical medicinal therapies of pulmonary fibrosis including symptom-focused therapy and disease-modifying therapy. Randomised controlled trials show that various therapies (eg, prednisolone and azathioprine, acetylcysteine, and warfarin) were ineffective or harmful, but disease-modifying therapies with nintedanib and pirfenidone are effective [47]. Both drugs are currently approved worldwide. Thus, therapies focusing on modifying pulmonary fibrosis are promising.
AMs and IMs primarily regulate the pulmonary fibrosis with cytokines TNF-α and TGF-β. Clinically recommended medicines for the treatment of pulmonary fibrosis are related to these cytokines. TNF-α can induce the adsorption of inflammatory cells and promote the occurrence of the inflammatory response. It can also regulate the production of other cytokines, deposit collagen, and promote the proliferation of fibroblasts, which plays an important role in the progress of pulmonary fibrosis. TNF-α inhibitors include etanercept, infliximab and adalimumab [48]. TGF-β can cause direct and effective stimulation to collagen synthesis, which makes an important impact on the development of pulmonary fibrosis. It takes action by enhancing the activity of connective tissue growth factor (CTGF), promoting the formation of muscle fiber cell type, as well as producing collagen and proteoglycan. Its action mechanism is associated with stimulating the Smads protein pathways. Clinical antifibrotic drugs Pirfenidone can reduce the proliferation of fibroblasts and inhibits collagen synthesis through regulation of TGF-β [49]. And some under-developmental TGF-β inhibitors such as GC1008, BG00011 and STX-100 can take actions by inhibiting the TGF-β pathway [50].
The NF-κB and MAPK pathways are important pathways to cytokine upregulation. The inhibition of these two pathways can reduce cytokines cycle and ease the fibrosis reaction. SP100030 is a type of underdeveloped NF-κB pathway inhibitor. Experiments showed that SP100030 inhibit the protease isomerized to block NF-κB pathway and reduces the degree of inflammation and pulmonary fibrosis. Current p38MAPK inhibitors under clinical trials include BIRB796, SB203580, TAK715, etc. BIRB796 shows good inhibition of all p38 MAPK isoforms in-vitro and in vivo [51].
There are no clinical chemokine inhibitors in the treatment of pulmonary fibrosis. Experiments showed that fluorofenidone (a me-too drug of pirfenidone) can inhibit the expression of MCP- 1 and TNF-α in mice macrophages induced by dead cells, which show the anti-inflammatory action. And fluorofenidone has the influence on NF-κB and MAPK pathway as well [52]. CNTO 888 (Carlumab), an under-developmental human anti-CCL2 antibody, is a monoclonal antibody that binds and neutralizes CCL2, can reduce the migration of macrophages [53]. Binding of CCL2 to its receptor CCR2 triggers chemotaxis. Inhibition of the CCR2 can reduce macrophages migration and accumulation in experimental models [54].
The Effect on AMs and IMs of TCM Treatment of Pulmonary Fibrosis
Large quantity of experiments showed that TCM had an influence on the expression of cytokines such as TNF-α, TGF-β, PDGF, CTGF, HGF, INF-γ, etc. [55]. Studies have found that macrophages are main cells which secrete tumor necrosis factor (TNF-α) in bleomycin-induced pulmonary fibrosis [56]. Experimental results of the buyanghuanwu decoction effect on the AMs of pulmonary fibrosis rats were also found the model group had higher levels of TNF-α than that of the control group. The levels of TNF-α in the model group reached its peak on the 7th day, and fell on the 28th day, with higher levels than the control group. The result showed that TNF-α has an important role in the pathological process of pulmonary fibrosis. The experiment showed that buyanghuanwu decoction can inhibit AMs of lung fibrosis rats to release TNF-α. So we can conclude that the mechanism for buyanghuanwu decoction preventing pulmonary fibrosis may be associated with its function of suppressing the TNF-α releasing of AMs [57]. The level of TNF-α in AMs supernatant was measured in each group of different periods during the Lignstrazine study of on pulmonary fibrosis. The results indicated that Lignstrazine could inhibit the release of TNF-α in AM of bleomycin-induced pulmonary fibrosis rats. It can be inferred that the mechanism of Lignstrazine treating pulmonary fibrosis is related to TNF-α release inhibition of AMs [58].
In the study of discussing the mechanism of Pneumonia Mixture (containing ephedra 60g) in the treatment of pulmonary fibrosis, researchers found that after the formation of bleomycin-induced pulmonary fibrosis in rats, TGF-β1 mRNA expressed in AMs and IMs in the model group increased more significantly than that in the control group. Therefore, we can infer that the mechanism of Pneumonia Mixture interfering the pulmonary fibrosis process is possibly associated with the reduction of the TGF-β1 expressing in AMs and IMs. The main components of Pneumonia Mixture are Astragalus, leeches, Polygonum cuspidatum, etc. Combined treatments of these drugs in all aspects of pulmonary fibrosis remediation inhibit the aggregation of inflammatory cells and reduces the synthesis of TGF-β1, as well as reduces abnormal tissues repairing and fibrosis progression [59]. The pathological process of lung diseases including pulmonary fibrosis is called “Xuansu disordered in lung” according to TCM theory. Ephedra and Schisandra are commonly used in the treatment of lung diseases.
Our laboratory has completed ephedra and Schisandra drugcontaining serum on normal rat AMs and IMs secrete TGF-β1. In vitro experiments found that ephedra, Schisandra could inhibit the TGF-β1 secretion of AMs and IMs. Ephedra-containing serum has a stronger inhibition of AM secretions compared to ephedracontaining serum, whereas Schisandra-containing serum has a stronger inhibition of IM secretions compared to Ephedracontaining serum [60]. The results showed that ephedra and Schisandra may have different influences on pulmonary fibrosis. Ephedra may have a major role in the acute inflammation period while Schisandra may have a major role in pulmonary fibrosis period.
Many experiments also elucidated the mechanism of treating pulmonary fibrosis from the regulation of chemokines. Xuejun Li showed the concentration of MIP-1α and MCP-1 in the plasma of the Panax Notoginseng, the treating group began to rise on the 3rd day and reached the peak on the 7th day in rats of bleomycininduced pulmonary fibrosis, then gradually decreased [61]. The concentration of both MIP-1α and MCP-1 in the plasma of the treating group had been significantly lower than that of the model group since the 7th day. Zhanshuai Song used Yifei-Huaxian granules in the treatment of paraquat-induced pulmonary fibrosis in rats showed the concentration of MCP-1 reached the peak on the 7th day and kept lower than the model group all through the experiment [62]. The result suggests that Chinese medicine reduces the migration of fibroblasts and inflammatory cells by suppressing the macrophages to express MIP-1α and MCP-1, thereby reducing the degree of pulmonary fibrosis.
Conclusion
In conclusion, AMs and IMs are vital regulatory macrophages in the pathological process of pulmonary fibrosis. Because of the anatomical site and cell function of AMs and IMs, anti-fibrosis drug options related to them have higher targeting ability than anti-inflammatory therapy drugs. And AMs and IMs can also be used to explore the multiple mechanisms of traditional Chinese medicine treatment for pulmonary fibrosis.
TCM has made great progress in the experimental study of pulmonary fibrosis prevention. Drugs involving enriching yin and nourishing the blood, clearing up heat and toxin, fortifying the spleen to boost qi, invigorating blood to dissolve stasis, supplementing the lung to boost the kidneys, relieving a cough and panting and many other aspects, meanwhile, the effective components of Chinese medicine provide a larger space and treatment basis for the clinic. Single herb showed good results in fighting against pulmonary fibrosis. At the same time, traditional Chinese medicine decoctions and Chinese patent medicines can have significant effects on pulmonary fibrosis [63,64]. Overall, the mechanisms explanation of the Chinese medicines on pulmonary fibrosis is still in its infancy.
The current studies were largely restricted to animal experiments rather than clinical studies, which focused on anti-inflammatory, immune and cytokines without systematic measurements and standards [65]. Because of the complicated compositions of single Chinese herbs, there is no clear scientific research basis for the effective compositions in the treatment of pulmonary fibrosis. And some therapeutic mechanisms are built on the hypothesis with a lack of rigorous experimental verification. Small samples, different clinical diagnosis and efficacy evaluation criteria result in the no convincing results. Although the research on the molecular and genetic level has been increasing in recent years, it is still limited to a few kinds of Chinese medicines. In this context, some experiments from the perspective of AMs and IMs in the pulmonary fibrosis rats and the influence of some common herbs for lung diseases on the AMs and IMs by using drug-containing serum were conducted. Thus, we can explore the pathological process of pulmonary fibrosis and explain the multiple mechanisms of TCM to guide clinical medication better, which is conducive to the succession and development of traditional Chinese medicine.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Gastroenterology & Hepatology please click on: https://juniperpublishers.com/argh/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/argh/ARGH.MS.ID.555790.php
26 notes
·
View notes
Text
Hepatocurative and Gluco-stabilizing Potentials of Ethanol Extract of Stem bark of Flacourtia indica in Aluminium Chloride induced Toxicity in Albino Wistar rats | Juniper Publishers

Juniper Publishers-Open Access Journal of Biomedical Engineering & Biosciences
Authored by Idoko A
Abstract
Herbal therapies have been used to manage liver diseases resulting from hepatotoxicity and hyperglycemia. The study investigated the hepatoprotective and gluco-stabilizing abilities of ethanol extracts of stem bark of Flacourtia indica in albino Wistar rats. Thirty-one rats of mixed sex, weighing 165-285g were used and divided into five groups of A to E. Acute toxicity study of the plant’s stem bark was conducted on group E (20 rats). At phase 1, group A (negative control) was made up of 3 rats administered no AlCl3 and no leaf extracts while groups B (positive control), C and D (test) made of 4 rats each, administered 260mg/kg body weight AlCl3 only, for 7 days. At phase 2, groups C and D were treated with stem bark extract of Flacourtia indica for 7 days. Activities of Alanine aminotransferase, Aspartate aminotransferase, Alkaline phosphatase, concentrations of Bilirubin, Albumin, Total protein and blood glucose were assayed with histopathological study on euthanized rats’ liver.
Results of phase 1 showed significant (p˂0.05) increase in the liver function enzyme and blood glucose after induction with AlCl3 compared with (phase 2) values of liver function enzyme and blood glucose with significant (p˂0.05) decrease after treatment with stem bark extract. Histopathology results in phase2 showed regeneration and healing of damaged hepatocytes of phase1. In conclusion, the liver injury induced by AlCl3 was found to be effectively managed by the treatment with Flacourtia indica’s ethanol stem bark extracts, with blood glucose stabilized. This could be as a result of the antioxidants and phytochemical contents of the plant, with diver’s potency to scavenge free radicals and reactive oxygen species.
Keywords: Flacourtia indica; Gluco-stabilizer; Hepatic function; Hepatoprotective; Hyperglycemia; Stem bark
Abbrevations: ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; WHO: World Health Organization; BIL: Bilirubin; TP: Total Protein
Introduction
The liver, a reddish – brown heaviest and largest internal organ weighs about 1.5 – 1.6 kg in an adult male and is about the size of an American football [1]. It is located behind the ribcage on the upper right side of the abdomen and is divided into four lobes with multiple lobes containing hepatic cells (hepatocytes). A normal liver enjoys an adequate blood supply and ability to regenerate its own tissues within few days [2]. The liver is known to perform over 500 functions in the body which include detoxification, excretion, digestion, metabolism, storage and homeostasis. It detoxifies harmful substances that are toxic to the body such as drugs, chemicals, heavy metals, alcohol and pesticides [3]. The liver excretes toxic chemical substances in the bile as well as xenobiotics, hormones and other by-products [4]. The liver plays a major role in homoeostasis stability of trace elements [5]. The liver is a major store house of glucose (in form of glycogen), iron and vitamins such as vitamins A, folate (B9), B12 and D [6]. Enzymes such as alanine aminotransferase (ALT), Aspartate aminotransferase (AST) and hormones are synthesized by the liver [7]. However, the liver is adversely affected by overloaded toxic substances, resulting in hepatotoxicity [8].
Hepatotoxicity is implicated with chemical induced liver damage resulting in chronic and acute liver diseases. Over 800 chemicals causing hepatic injuries abounds. They include drugs used to suppress pain and reduce inflammation such as ibuprofen, acetaminophen or paracetamol, naproxen and aspirin (Non-Steroidal Anti-inflammatory Drugs), alcohol, industrial and laboratory chemicals such as Aluminum trichloride AlCl3 and carbon tetrachloride CCl4 and natural toxins such viruses, aspergillus flavus [6,9,10]. Meanwhile, AlCl3 has demonstrated high potency in exerting hepatotocity, the mechanism by which AlCl3 exert its injury on the liver is not yet clear [9]. These induced toxic chemicals in the hepatic tissue, render the liver disease with malfunction including hepatitis, liver cancers, fatty liver, primary biliary cirrhosis, primary sclerosing cholangitis, hemochromatosis, hyperoxaluria and oxalosis and Wilson’s disease [11,12]. The earth is made up of about 8.13% of aluminium. The metal has got wide utilization, therefore increasing the chances of exposure into the body through the intestinal tract and the lung. It is a used in manufacturing cosmetics such as roll-on and deodorant, cooking utensils, food additives and drugs such as antacids. In water purification, aluminium salts are also used [13].
The practice of traditional medicine, using plants and plants products for the treatment of ailments is an age long practice. Several medicinal plants with their herbal functions have been discovered and more are still be researched on [14]. Medicinal plants have been found to possess several activities such as hepatoprotective, nephroprotective, antimicrobial, anticancer, anti-inflammatory, hypoglycemic, antihypercholesterolemia, hypoglycemia, heamatinic and antioxidant activity [15-17]. These beneficial therapeutic properties and efficient pharmacological impacts of medicinal plants on man and animals are not farfetched from the numerous bioactive compounds they contain [18]. The availability of herbal alternatives for the management of liver disease and other ailments is been encourage by world health organization (WHO) to be better developed for improved efficacy, safety of use, cheap to purchase and accessible for patronage [19].
Flacourtia india is a wide spread medicinal plant, of Salicaceae family, tribe of Flacourtiaceae, genus of Flacourtia and specie of Indica [20, 21]. It is known as Governor’s plum in English, kondai or Katai in India, Cilimu in China and in Nigeria: it is called Akpuru in Igbo, Isada in Hausa and Iyeye in Yuroba [22]. The plant is tropical specie with a natural geographical occurrence in Africa and Asia. Predominantly, Flacourtia india is said to be a native to both Africa and East Asia [23]. Flacourtia indica is a bushy small shrub like tree, having a spiny, erect, rough, strong stem bark, that extend with branches. It spines branched and spread up to 12cm long and to a maximum height of about 15cm (50 feet) [22]. Several pharmacological abilities of Flacourtia indica have been exploited with the whole plant, leaf, seed, fruit, stem, bark and root. These include hepatoprotection against AlCl3, paracetamol and CCl4 induced hepatic damage [9,24], anti-diabetic, anti-anxiety, antimicrobial, anti-malaria, anti-asthmatic, diuretic, antioxidant, analgesic/anti-inflammatory and anti-hyperlipidemia [18,25- 27]. The plant has been reported by previous researchers in their phytochemical analysis to contain several bioactive compounds, including phenolic compounds, flavonoids, saponins, carbohydrate, Coumarin Glycosides [28].
Blood glucose concentration is an important index handled by the liver in monitoring and stabilizing blood glucose levels. In post absorptive state, the fasting blood glucose concentration of a healthy (normal) individual is 70 – 100mg/dl (4.5-5.5mmol/l). However, after eating a carbohydrate meal, the level of blood glucose may rise to 120-140mg/dl. It is generally established that the value for plasma concentration is about 15% slightly higher than the value of blood glucose. Hypoglycemia implies a decrease in blood glucose concentration from the normal and hyperglycemia is an increase in blood glucose concentration from the normal [29,30]. Plants have been reported to have herbal ability in reducing high glucose concentration, not necessarily causing an unhealthy hypoglycemia, but attempting to stabilize blood glucose level in albino wistar rats [30]. Thus, in view of these, it became imperative to investigate the hepatocurative and gluco-stabilizing effects of stem bark of Flacourtia indica using ethanol solvent extraction in order to ascertain the previous claim and establish new fact.
Materials and Methods
Chemicals
Aluminium trichloride AlCl3 was purchased from BDH Laboratories/Chemicals Ltd, Poole, England. Kits used for the liver function assay were obtained from Randox Laboratories Ltd, 55 Diamond Road, Crumlin, country Antrim, BT29 4QY, United Kingdom. They include; Bilirubin (BIL), Alanine Aminotransferase (ALT), Aspartate Aminotransferase (AST), Albumin (ALB), Total Protein (TP). All other chemicals used are pure and of analytical grade.
Collection and Preparation of Plant Samples
Fresh plant materials of Flacourtia indica (Governor’s plum) were collected from around Emene jurisdiction in Enugu state, Nigeria. The required plant stem bark was authenticated and a voucher number of PSB/109-12. A was given by Mr. Okafor, C.U., a botanist in plant tissue culture and biotechnology department, Faculty of Biological Science, University of Nigeria, Nsukka. The plant extract was prepared by pilling the bark from the stem of the plant and cut into pieces for easy air drying. The dried samples were ground into powder using an electric grinder. The powdered parts were soaked in ethanol and allowed to stay for 48 hours at room temperature after which they were filtered. After filtration, the samples were then taken and evaporated to dryness using water bath at 80oc. The evaporated extracts were reconstituted with distilled water relative to the weight of the evaporated extract. The volumes of the extracts to be administered were calculated according to the body weight of the rats using the formula:
Collection and preparation of blood sample
Three milliliter (3mls) of blood was collected from the rats by capillary pressure insertion into the side of the eye using capillary tubes into a plain bottle, for the collection of serum used for biochemical assay (liver function test). The samples in bottles were stored at room temperature.
Acute Oral Toxicity (LD50) Study
Twenty (20) rats were used for oral acute toxicity study (LD50) of the plant. The acute toxicity study of ethanol stem bark extract of Flacourtia indica was evaluated in two phases as described by [31]. In the 1st phase, doses of 10mg/kg, 100mg/kg, and 1000mg/kg were administered to 3 rats each. The body weight of rat was noted before and after extract administration. Single dose of ethanol extract was administered orally and observed from the time of administration, for toxic symptoms, such as behavioral changes, loco-motion, convulsion and mortality, then overnight and finally for a time period of five days. In the absence of mortality in the first phase, higher doses of 1500mg/kg, 2500mg/ kg, 3500mg/kg and 5000mg/kg were then administered on 1 rat each of which one mortality was observed in the 2nd phase of the experiment at 3500mg/kg body weight. LD50, the amount or lethal dose of materials given all at once, which causes the death of 50% of a group of test animals was calculated with the formula below;
Study Animals
Albino Wistar rats of 165-285g weight, of either sex were obtained from university of Nigeria Nsukka. Animals were housed at an ambient temperature and relative humidity in the animals’ house of natural sciences, Caritas University, Amorji – Nike Enugu. The rats were allowed to acclimatize for one week prior to the experiment and had access to standardized pelletized finisher feed and clean water within the period the acclimatization. The principle of laboratory animals’ care and ethical guidelines for investigation of experimental pain in conscious animals were followed respectively [32,33].
Experimental Design
Experimental design was carried out in two phases thirty five (35) Wistar albino rats were used, divided into A, B, C, D and E as follows; at phase 1,
Group A: Control (negative control) consist of 4 rats, no Aluminum chloride (AlCl3 were administered.
Group B: Test control (positive control) consist of four (4) rats, were administered orally with 260mg of Aluminum chloride (AlCl3) without extract given.
Group C: Consist of four (4) rats, were orally administered with 260mg/kg body weight of rats.
Group D: Consist of four (4) rats were orally administered with 260mg/kg body weight of rats. At phase 2, groups C and D were treated with ethanol stem bark as follows;
Group C: Consist of four (3) rats, were treated with stem bark extracts of 500mg/kg body weight of rats.
Group D: Consist of four (3) rats were treated with stem bark extract of 700mg/kg body weight of rats.
At the end of phase 1 and 2, one rat from each group was randomly selected and sacrificed by euthanization using chloroform and liver removed for histopathology study.
Induction of Liver Injury
Liver injury was induced in rats of group B – D by single oral administration with 260mg/kg body weight of AlCl3 respectively.
Liver Function Assay
After collection of blood sample from rats serum was collected by clot retraction. Serum ALT, AST, ALP, Albumin, Total protein and Bilirubin were assayed with the use of kits from Randox Laboratories Ltd, 55 Diamond Road, crumlin, country Antrim, BT29 4QY, United Kingdom, following the manufacturer’s procedure.
Histopathological Studies
The selected models were sacrificed and dissected after which the liver organs were excised and fixed in a buffer medium of 0.9% of formalin solution in plain tissue bottles. The tissues were embedded in paraffin, solid section was cut 5um and stained with hemotoxin and eosin, the sections were examined and analyzed by the distant Specialist of histopathology, University of Nigeria under high microscopy instrumentation having photomicrographic attachment.
Statistical analysis
Results were expressed as mean ± standard deviation and analyzed using one-way ANOVA (analysis of variance, p value (p<0.05) was considered significant. A component of graph pad instat 3 software version 3.05 by graph pad Inc. was employed [34].
Results
Acute toxicity results
The oral administration of ethanol extract of F. indica stem bark resulted in behaviour changes and mortality up to the dose of 3500 mg/kg body weight at the second phase. Though, the LD50 of F. indica ethanol stem bark extract was calculated to be 4183mg/kg (higher than 3500 mg/kg). Table 1 shows the result of the acute toxicity in phase 1 and 2. The liver function test of rats after induction with 260mg AlCl3, for liver injury is shown in Table 2. A significant (p<0.05) increase was observed in TP, ALB, BIL, ALP, ALT and AST of control compared to test control and test groups.
Table 3 shows liver function indices of rats administered various dose of stem bark (500mg and 700mg) extract of flacourtial- Indica for 0ne week. A significant (p<0.05) increase was observed in all parameters assayed in the test groups compared to the test control and control group. The significant increase (p<0.05) in Table 2 when compared to Table 1, reveals the potential hepato- healing effect of Flacourtia indica not necessarily in a dose dependent manner.
Results are mean ± standard deviation, Values in the same column bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups.
TP: Total Protein; ALB: Albumin; BIL: Bilirubin; ALP: Alkaline Phosphatase; ALT: Alanine Transaminase; AST: Aspartate Transaminase
Results are mean ± standard deviation, Values in the same row bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups; TP: Total Protein; ALB: Albumin; BIL: Bilirubin; ALP: Alkaline Phosphatase; ALT:
Alanine Transaminase; AST: Aspartate Transaminase
Table 4 presents the blood glucose concentration of rats after induction with AlCl3 and after Treatment with stem bark extracts of Flacourtia indica. After administration (treatment), with Flacourtia indica, the blood glucose concentrations of test groups (C and D) decreased significantly (p<0.05) compared to after induction with AlCl3 in a dose dependent pattern, thus acerbating induced hypoglycemia.
Results are mean ± standard deviation, Values in the same row bearing similar superscripts are significantly different at P<0.05. (n=4).
Key: A: Control Group; B: Test Control; C and D: Test groups
Result of Histopathology Analysis
The results of histopathological study of liver tissue of rats at induction (group A and B), after induction with AlCl3 and after treatment with F. indica ethanol stem bark extract (group C and D) as cross sections are shown in Figure 1 & 2. Photomicrograph of liver showed cytoplasm containing empty (black arrow) and fluid filled (red arrow) appearing vacuoles which pushed out the nucleus and then formed a signet-ring like appearance. H&E. mag. 400X (Figure 3). Photomicrograph of liver showed minor distortion of the hepatic cords leading to enlarged sinusoids (black arrow), also macrophages (red arrow) and focal necrosis (star) were also observed. H&E. mag. 100X (Figure 4). Photomicrograph of liver showed massive influx of inflammatory cells (black arrow), damaged hepatocyte (red arrow), degeneration of the hepatocyte cords and the affected hepatocytes are aligned in deformed cords which compresses the lumen of the sinuses. Zonal fatty changes occurred in the liver lobules, diffusely affecting the same zone. The fatty degeneration, vacuoles appeared in the cytoplasm around the nucleus, because the lipid content may be dissolved in the course of embedding. The vacuoles are empty with absence of inflammatory cells (black arrows) and regenerated hepatocytes (white arrows). H&E. mag. 400X.
Discussion
The significant increase that was observed in the liver function indices in Table 2 of groups C and D, as compared to Table 3 was as a result of aluminium chloride administration. This result is consistent with other researchers’ who reported that aluminium chloride is capable of inducing hepatic injury (hepatotoxicity), using a minimal dose of 34 mg/kg body weight administered in rats’ diet [35] and oral exposure in drinking water of 40 male Wistar albino rats of 0, 64mg/kg, 128mg/kg and 256mg/kg body weight AlCl3 for 120days, respectively [9]. AlCl3 induced toxicity has been reported to have toxic effects on liver, kidney, biochemical dysfunction and general health challenge [13]. A significant increase was seen in blood glucose concentration of rats after induction with AlCl3 compared to after treatment with Flacourtia indica (Table 4). This increase could have resulted from the inability of the liver to secret insulin owing from the hepatic damage caused by AlCl3. The mechanism through which this was done was taught to be linked to hepatic-stress related release of epinephrine, a factor inhibiting insulin secretion [36].
The potent inducement of liver injury by AlCl3 was supported by histopathology results (Figures 1, 2, 4 & 5). The underlying mechanism through which AlCl3 induces hepatic damage, as hepatic toxicant, as shown by the histopathology results could be associated to fatty liver incidence as a result of accumulated triacylglycerols and lipoprotein [36]. The histopathological results’ examination of liver tissues reveals intact hepatocytes, distinct architecture of kupffer cells and cytoplasmic aligning of the negative control group. Induction by AlCl3 in test groups revealed several degrees of hepatic injuries including; infiltration of mixed infiltrates in the sinusoid, diffused fatty changes, focal necrosis, massive influx of inflammatory cells, damaged hepatocyte, degeneration of the hepatocyte cords and the affected hepatocytes are aligned in deformed cords which compresses the lumen of the sinuses (Figures 2, 4 & 5). Treatment with Flacourtia indica’s ethanol extract stem bark with 500 mg/kg and 700 mg/ kg in rat’s liver revealed regeneration of hepatocytes, absence of inflammation, with almost healed hepatic architecture (Figures 3 & 6). This is also consistent with [28], supporting the claim that Flacourtia indica protects the liver against AlCl3 hepatic damage in treated groups with healing features, typified by absence of damaged and degenerated hepatocytes, necrosis and inflammation.
Treatment of the AlCl3 induced hepatotoxic rats with the stem bark extract of Flacourtia indica revealed a significant decrease in AST, ALT, BIL, TP, ALP and blood glucose concentration and a slight significant increase in serum albumin, implying that hepatic tissues are regenerating and healing. This observation was supported by the histopathology analysis of the liver tissues which shows recuperation of hepatic cells after administration of the stem bark extract. This is in support of the work of [28], who reported that Flacourtia indica prevents and protect AlCl3 and CCL4 induced rats’ hepatic damage through augmentation of antioxidant enzyme activity. Flacourtia indica appears to prevent the increase in the activities of the main liver function enzymes (ALP, AST, ALT, BIL and TP) by a counter and effective action against the hepatoxic damaging effects of AlCl3. This action might be due to Flacourtia indica’s potentials as an indirect antioxidant promoter and free radical scavenging abilities in preventing membrane failure and cellular necrosis [20].
Table 4 shows the blood glucose concentrations and effect of oral administration of the different doses after induction with 260 mg AlCl3 and 500 mg/kg and 700 mg/kg body weight of Flacourtia indica on blood glucose concentrations of rats. After administration of stem bark extract of Flacourtia indica, the blood glucose levels of test groups (C and D) decrease significantly (p<0.05) compared to after induction with AlCl3 in a dose dependent pattern, thereby bringing the concentration of blood glucose to a stabilized level from the AlCl3 induced hepatotoxic level. Reduction in blood glucose by Flacourtia indica’s stem bark could be due to the presence of both micro and macro mineral elements and phytochemicals, having antioxidant and blood glucose enzyme regulating and stabilizing control [19,28,37,38], reported the mineral elements composition in Flacourtia indica to include magnesium, manganese and zinc. Thus, the mechanism behind the stability of blood glucose by Flacourtia indica could be understood from the role of these mineral elements as cofactors to glycolytic enzyme especially hexokinase and phosphofructose [17]. The blood glucose level stabilizing effects of Flacourtia indica appears to be maintained by the constant furnishing of these mineral elements [37,38].
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Biomedical Engineering & Biosciences please click on: https://juniperpublishers.com/ctbeb/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/ctbeb/CTBEB.MS.ID.555971.php
28 notes
·
View notes
Text
Chemical, Photochemical Composition, Physical and Sensory Qualities of acha-Guava Flour Blends and Biscuits | Juniper Publishers
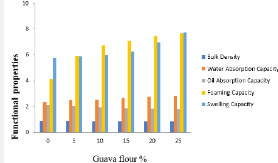
Juniper Publishers-Open Access Journal of Nutrition & Food Science
Authored by Ayo JA
Abstract
The study investigated the chemical, phytochemical composition, physical and sensory qualities of acha-guava flour blends and biscuit the work was aimed at ameliorating the quality of acha-based biscuits with the addition of guava flour. Flour blends were produced by substituting guava flour into acha flour at 5, 10, 15, 20, and 25%. Proximate composition, pasting properties, functional properties, phytochemical composition, vitamins and mineral of the flour blends were determined. Biscuits were produced from the flour blends and the physical properties and sensory qualities of the biscuits were analyzed. The carbohydrate and protein decreased from 81.60to 77.30 and 8.32to 7.70%, respectively. The moisture content, fat content, fibre and ash content increased from 8.08to 8.44, 1.28 to 2.63, and 0.21to 2.5and 0.20 to 1.62% respectively, with increase in the added guava flour (5-25%). Water absorption, foaming, and swelling capacity of acha flour increased from 2.35to 2.83ml/g, 4.13to 7.65ml/g and 5.75to 7.74ml/g, respectively. Bulk density and oil absorption capacity decreased from .89to .85/cm3 and 2.10 to 1.81ml/g respectively, with increase in the added guava flour (5-25%). The peak viscosity, trough viscosity, breakdown, final viscosity, and setback decreased from 2336.83 to 1107, 1535 to 935, 801 to 172, 3719.8 to 1863, and 2186.0 to 928RVS, respectively, with increase in the percentage guava flour. Iron, carotenoid, vitamin C and total phenol increased from 4.0 to 25.0ppm, 5.36 to 14.17mg/100g, 1.94 to 7.96mg/100g, and 0.22 to 0.86mg/100g respectively, while phosphorus decreased from 1110.10 to 814.3ppm with increase in percentage of added guava flour. There was an increase in break strength and spread ratio ranging from 1.35 to 2.64kg and 4.53 to 5.15 respectively, as a result of the increase in level of guava-flour substitution. The reverse was observed for the thickness, diameter, volume and weight of the biscuit which ranges from .88 to .60cm, 4.34 to 4.13cm, 13.05 to 8.00cm3, and 11.50 to 10.70g respectively. Sensory qualities evaluated were colour, texture, taste, odour, crispiness, and general acceptability with an average mean score ranging from 4.60 to 7.65, 5.50 to 6.85, 6.10 to 7.45, 5.80 to 6.85, 5.55 to 6.85and 6.20 to 7.95. The sample, 95:5% acha-guava blends is the most preferred and acceptable with average mean score of 7.95 and corresponding increment of 0.28, 2.22, 79.38, and 1.3% of ash content, protein, fat and crude fibre respectively.
Keywords: Water absorption; Foaming; acha flour; Peak viscosity; Trough viscosity; Breakdown; Final viscosity
Introduction
Biscuit and Cookies are usually produced from wheat flour and they are the same product since the British call them biscuit while the Americans call them cookies [1,2] identified an increasing tendency among children and adults to move away from traditional eating pattern of three meals a day to eating snacks instead of meal. Biscuits enriched with carrot generally have been found to be rich in carbohydrate and protein; they contain fat (14.10 ± 0.08%), carbohydrate (69.31 ± 0.12%), ash (2.32 ± 0.03%), and protein (8.10 ± 0.01%), fibre (0.93 ± 0.01) and moisture (6.17 ± 0.02) as reported by [3].
Cereal grains like wheat, corn, rice, barley, sorghum, etc. provide 68% of the total world food supplies. Wheat is mainly used as a dietary staple, averaging two-thirds of total consumption [4]. Owing to shortage of wheat, several developing countries have devised programs to assess the feasibility of alternative sources for substituting or blending of wheat flour with other cereals [5].
acha (D. exilis) is of considerable importance in Nigeria where it is commonly eaten, often in preference to other cereals, as many as three times a day as a porridge, couscous or non-alcoholic beverage, valued as a weaning food because of its low bulk and high caloric density with minimal processing requirement, it grows even where rainfall and soil fertility are poor and can be stored in closed containers for many years without need of preservatives [6].
acha contains high water absorption capacity that gives it capacity to be utilized in baked foods. It also contains pentosans which gives it the ability to form gel in the presence of oxidizing agents at room temperature with high residual protein coupled with high levels of Sulphur and hydrophobic amino acid residues which makes it useful in baking [7]. The recent finding of the unique properties of acha flour, particularly in relatively lowering the blood glucose level and which could subsequently reduce the diabetic populace have make researchers to focus on D.exilis [8].
Guava (Psidium guajava) is usually consumed as fresh fruit, being a flavorful and healthy alternative for a snack. It is also served with cream and sugar for dessert or combined with other fruits in cocktails and salads [9]. Guava juice is also very popular, being an excellent juice alternative for infant feeding or may be eaten with salt, pepper, vinegar, soy sauce or may be preserved into jam, butter, marmalades, relishes, and chutneys (Glaucia et al. 2012). Few studies have been conducted on the phytochemistry and total antioxidant capacity of guava, especially processed guava juice or puree. However, it is well documented that guava contains a very high amount of vitamin C, anthocyanin, lycopene, and carotenoids, [10].
The leaves of guava are used traditionally by many people to overcome a wide range of diseases, while the guava fruits are believed to overcome several of problems and a source of antioxidants [11]. Red guava fruit is also believed to help cure dengue hemorrhagic fever (DHF). Guava fruit contains vitamin C, two times higher than other fruits such as orange which makes it an important compound that has an antioxidant activity [12]. Other compounds in guava fruit are carotenoids such as betacarotene, lycopene, and beta-cryptoxanthin, and polyphenols [13]. Lycopene is associated with the prevention of cardiovascular damage due the LDL oxidationas the impact of dyslipidemia [14]. Antioxidant content in guava fruit can be used as a source of natural antioxidants; these include vitamins A, C, and E as well as numerous non-nutritive compounds such as polyphenolics, flavonoids, carotenoids, and thiol-containing compounds. Lycopene content in guava fruit is proven to prevent or delay the oxidative damage of lipids, proteins and nucleic acids caused by reactive oxygen species (ROS) [12].
Resent investigations in relation to the unrealized ability of acha to ameliorate the crises of diabetes and its deficiencies in some nutrient, have called for its fortification to bridge the existing gap. The abundance and perishability of guava with its high nutrient content calls for processing to reduce wastage and could be used as a fortifier or enriched food product with relatively low nutrient.
Fortification of acha biscuits with guava could improve the antioxidant, minerals, vitamin content and add value to the sensory qualities of food products. Also, the use of guava could reduce post-harvest losses, create more market for the raw material and increase the quest for production of nutritious food by food industries. The objective was to determine the chemical, phytochemical composition, physical, and sensory qualities of acha-guava flour blend biscuits.
Materials and Methods
Materials
Cream colored acha grains (D. exilis) purchased from Jos central market in Plateau state, Nigeria while the fresh guava (Psidium guajava (red colored) was obtained from Bayesa, Ussa Local Government, Taraba State, Nigeria. Other ingredients such as baking fat (Simas), baking powder (Omega), and salt (Dangote table salt) were purchased from Wukari New market, Taraba state, Nigeria.
Methods
Preparation of acha flour
acha flour was produced using the method described by Ayo et al. [8]. acha grains were winnowed to remove chaff and dust. Adhering dust and stones were removed by washing in water (sedimentation) using local calabashes and floating foreign materials by decanting. The washed and de-stoned grains were drained and dried in a cabinet drier (Model: CD0005, FT3) at 40°C to a moisture content of about 12%. The dried grains were milled using Attrition milling machine (Inch15HP Super 150-180 Kilogram Tw-HM-1016) and sieved (0.3μm aperture size). The flour was packaged inpolyethylene bag and stored at 5oC as acha flour for later use.
Preparation of guava flour
The procedure as described by Sanjinez-Argandona et al. [15] was modified and used in the preparation of guava flour. Fresh Matured and ripe guava fruit were obtained. Washed, sorted, peeled, sliced and steam blanched (Hughes Blancher Model #:02- 1471) for 3min. The sliced guava fruit were dried at 40°C in oven (San-Del Model 50) and milled using attrition mill (Inch15HP Super 150-180 Kilogram Tw-HM-1016) and sieved (0.3μm aperture size). Packaged in a polyethylene bag and stored (at temperature 5oC).
Formulation of flour blend
The guava flour was mixed with acha flour separately at different proportions (5:95, 10:90, 15:85, 20:80 and 25:75) while one hundred percent (100%) acha flour and wheat was used as the control. The flours were thoroughly mixed using a Kenwood blender to a uniform blend by Ayo & Gidado [3].
Production of acha-gauava composite biscuit
The recipe adopted for the work is shown in Table 1 as described by Ayo & Gidado [3]. The guava powder was substituted into acha flour at 5, 10, 15, 20 and 25% respectively. The sweet potato powder was beaten into the fat until fluffy and acha-guava composite flour and other ingredients were added, while mixing at a medium speed of Kenwood blender. The method described by Ayo & Gidado [3] was used to produce the biscuits.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Proximate composition determination
The proximate analysis of samples for moisture content, crude protein, ash, Crude fat, Carbohydrate and crude fiber was carried out on the flour as described by AOAC [16].
Determination of minerals and vitamin
The phosphorous, iron and Vitamin B1 of the acha-guava flour blends were determined as described by AOAC [16] methods while the Vitamin C content was determined by direct calorimetric method as described by Kalia [17].
Determination of phytochemicals
Carotenoids content of the acha-guava flour blends was determined as described by Krishnaiah et al. [18] method, while the total polyphenol was determined by Folin-Ciocalteu’s method using gallic acid as standard as described by Priyanka [19].
Functional properties determination
The functional properties: - bulk density, water absorption capacity, oil absorption capacity, foam capacity and swelling power of the acha–guava flour blends were determined as described by Onwuka [20].
Determination of pasting properties
Pasting properties of the acha-guava composite flour were determined using the Rapid Visco Analyzer (RVA-4, Newport Scientific, Australia and Thermocline for Windows programme).
Determination of physical properties
The breaking weight, volume, break strength and spread ration of acha-guava composite biscuit were determined using the method described by Ayo et al. [8].
Sensory Evaluation
The sensory quality of the acha-guava biscuits was evaluated using twenty untrained panelists, randomly selected from Department of Food Science and Technology Federal University Wukari, Nigeria based on their familiarity with the biscuit. The biscuits, appropriately coded (ACH, RJG, EYM, and AMD) and of the same size and temperature (29 ± 3oC) were placed in white plastic plates separated by compartment and placed in sensory laboratory. The panelists rinsed their mouths with bottled water after tasting each sample and were not allowed to make comment during evaluation to prevent influencing other panelist. A nine-point Hedonic scale with one (1) representing “extremely dislike” and nine (9) “extremely like” was used, presented as a questionnaire. The qualities assessed were color, texture, taste, flavor, crispness and general acceptability as described by Ayo & Gidado [3].
Statistical Analysis
All the analyses were conducted in duplicates in completely randomized design. The data were subjected to analysis of variance using Statistical Package for Social Science (SPSS) software version 23, 2017. Means where significantly different were separated by the least significant difference (LSD) test. Significance was accepted at p<0.05
Results and Discussion
Proximate Composition of acha-guava flour blends
Flours and flour blends were produced from acha and guava flour blend and proximate composition is presented in Table 1. The carbohydrate and protein decreased from 81.60±.39 to 77.30±.02 and 8.32±.03 to 7.70±.02%, respectively. The decrease could be due to poor protein content level in guava flour. The moisture content, fat content, fibre and ash content increased from 8.08±.02 to 8.44±.48, 1.28±.02 to 2.63±.03, and .21±.03 to 2.5±.043 and .20±.02 to 1.62±.06% respectively, with increase (0- 25%). The effect of adding guava to acha are significant, p>0.05. The 75:25% acha-guava samples had the highest value for moisture content, crude fibre, fat and ash, while the 100:0% achaguava samples had the highest value for protein and carbohydrate
The increase in moisture content could be due to the relative increase in the fibre content of the added guava as it is hygroscopic. Fibers have the ability of absorbing moisture. The crude fibre increased with increase in added guava powder. This could be due to the presence of high dietary fibre content in fruits and vegetables [21]. Accurately measuring the fibre content of foods is critical to making a sound benefit claim, whether it is a nutrient claim, structure-function claim, or health claim [22].
Ash content indicates the presence of mineral matter in food. Increase in ash content indicates that samples with high percentage of ash will be good sources of minerals. The carbohydrate decreased with increase in guava powder addition. The results obtained in this study are within the ranges earlier reported for acha [23]. Ayo & Gidado [3] reported similar range for biscuits from acha and carrot flour. Olapade et al. [24] also reported a similar range for biscuits from acha and cowpea flour. The carbohydrate contents of these samples are an indication that the products are good sources of energy.
Functional properties of acha-guava flour blends
The result of the functional properties of acha-guava flour blends are shown in Table 2. The effect of added guava flour (0- 25%) on water absorption, foaming, and swelling capacity of acha flour increased from 2.35±.07 to 2.83±.11ml/g, 4.13±.70 to 7.65±.16ml/g and 5.75±.02 to 7.74±.08ml/g, respectively. Bulk density and oil absorption capacity decreased from .89±.01 to .85±.014g/cm3 and 2.10±.141 to 1.81±.01ml/g, respectively (Figure 1). The 75:25% acha-guava samples had the highest value for water absorption, swelling and foaming capacities and lowest value for bulk density and oil absorption capacity. The increase in the WAC could be due to molecular structure of the guava flour [25]. The effect is significant different, p>0.05. Functional properties are the intrinsic physico-chemical properties that reflect complex interaction between the composition, structure, confirmation and physic-chemical properties of protein and other food components and the nature of the environment in which these are associated and measured.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
High WAC of composite flour suggests the potential of the flours in the formulation of foods such as sausage, dough and bakery products where hydration to improve dough handling is a preferred characteristic. The observed variation could be due to different protein concentration, their degree of interaction with water and conformational characteristics [26]. The increased swelling capacity of flours depends on the particle size, variety and type of processing methods. The results agreed with the reported quality attributes of biscuit from acha (digitariaexilis) flour supplemented with cowpea (vignaunguiculata) flour by Olapade et al. [24].
The decreased OAC of the flour blends upon addition of guava flour might be attributed to the molecular structure of starch which is loosely linked, allowing for more penetration of liquid materials. The blends could also be used in formulations for products such as ground meat, doughnuts and pancakes, where oil absorption is not of paramount importance [27]. The bulk density of flour is measured without the influence of any compression. This revealed that bulk density depends on the particle size and moisture content of flours. The high bulk density of flour could suggest their suitability for use in food preparations. However, low bulk density would be great significance in the preparation of complementary foods [28].
Pasting Properties of acha-guava flour blends
The results of the pasting properties are shown in Table 3. The peak viscosity, trough viscosity, breakdown, final viscosity, and setback decreased from 16.83±.50 to 1107±.50, 1535±.50 to 935±.50, 801±.50 to 172.±.50, 3719.8±.29 to 1863±.50, and 2186.0±.50 to 928.0±.50RVS, respectively, with increase in the percentage guava flour. The effect of adding guava powder are significant, p>0.05, for all the parameters except for peak time. The 100:0% acha-guava Sample had the highest values for all the properties. Pasting properties are dependent on the rigidity of starch granules, with consequent effect on the granule swelling potential and the amount of amylose leaching out in the solution [29]. The high content of starch in the 100:0% acha-guava (control) sample, compared to other samples may contribute to some extent, to the higher pasting viscosity observed which could be the resultant effect of decrease in viscosities with decrease in the acha flour proportion.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
High values of breakdown associated with high peak viscosities could be related to the degree of swelling of the starch granules during heat treatment. The peak viscosity often correlates with the quality of end-product and also provides an indication of the viscous load likely to be encountered by a mixing cooker (Sanaa and El-Sayed, 2004). The lower setback viscosities of acha starches could make the suitable for preparing gels with tendencies to synereses [30].
Pasting time of fonio grains (acha) reported by Jideani et al. [31] was significantly higher than that obtained in this study which could be due to climatic and soil factors. A higher pasting temperature indicates high water-binding capacity, higher gelatinization tendency and lower swelling property of starchbased flour due to high degree of associative forces between starch granules [32]. Pasting temperature is one of the properties which provide an indication of the minimum temperature required for sample cooking, energy costs involved and another components stability. Therefore, from the results obtained, 100% acha samples could be said to be more sensitive to heat treatment with less energy consumption, thereby saving time and cost. Ayo & Gidado [3] reported a similar range for pasting properties of acha-carrot biscuits.
Minerals, vitamins and phytochemical composition of acha-guava flour blends
The results minerals, vitamins and phytochemical composition of acha-guava flour blends shown are shown in Table 4. Iron, carotenoid, vitamin C and total phenol increased from 4.0±.50 to 25.0±.50ppm, 5.36±.04 to 14.17±.06mg/100g, 1.94±.05 to 7.96±.02mg/100g, and .22±.03 to .86±.02mg/100g respectively, while phosphorus decreased from 1110.10±.50 to 814.3±.50ppm with increase in percentage of added guava flour. The effect of adding guava to acha flour are significant, p>0.05 on the vitamin C and phosphorous content. The 75:25% acha-guava samples had the highest value for iron, carotenoid, vitamin C and total phenol. Iron and vitamins (vitamin C and B1) increased as the levels of substitution of guava flour with acha increased (5-25%). The findings agreed with that of Ayo et al. (2010) and Igbabul et al. (2014). Carotenoids are abundant in the red, yellow, orange, and green colored vegetables and fruits. They are, after chlorophyll, the second most widely occurring plant pigment found in nature (MacDougall 2002). The high degree of hydration and long carbon chain length of these molecules makes them hydrophobic and therefore fat-soluble molecules. The major purpose of carotenoids in the human diet is to serve as precursors to pro-vitamin A, a required nutrient for humans (MacDougall 2002).
* Average mean score with the same letter(s) on the same column are not significantly different, P=0.05.
The vitamin C is one of the most abundant antioxidants consumed, with fruits being the main source of the nutrient. Because L-ascorbic acid is an excellent reducing agent and is abundant in nature, it may help stabilize phenolics and other antioxidants during processing by the donation of hydrogen atoms. These compounds could also impart color, astringency, and bitterness and possible nutritional properties [33].
Physical composition of acha-guava blend biscuits
The physical properties of the acha-guava flour blend biscuits are shown in Table 5. There was an increase in break strength and spread ratio ranging from 1.35±.01 to 2.64±.01kg and 4.53±.01 to 5.15±.01, respectively, as a result of the increase in level of guavaflour substitution. The reverse was observed for the thickness, diameter, volume and weight of a piece of biscuit which ranges from .88±.02-.60±.00cm, 4.34±.0-4.13±.04cm, 13.05a±.07-8.00±.14cm3, and 11.50±.00 - 10.70±.71g respectively. The 85:15% acha-guava samples had the highest breaking strength and weight, 75:25% had lower values in volume, thickness and diameter, and 95:5% samples had the highest in diameter, thickness and volume respectively. The effect of adding guava powder are significant, p>0.05, for weight. The increased spread ratio observed in guavaflour substituted biscuit samples could be due to the difference in the particle sizes and characteristics of the constituent flours of guava and acha (Agu et al, 2007). Joel et al. [34]and Olapade et al. [24] reported similar trend in biscuits from wheat and full fat soya and biscuit from acha flour supplemented with cowpea flour. The spread ratio could be an indicator of biscuit quality.
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Sensory evaluation of acha-guava flour blend biscuits
The sensory qualities evaluated are presented in Table 6 The result showed that the average mean score for colour, texture, taste, odour, crispiness, and general acceptability ranged from 4.60±2.19-7.65±1.09, 5.50±1.76-6.85±1.09, 6.10±1.74- 7.45±1.09,5.80±1.39-6.85±1.38, 5.55±2.09-6.85±1.69 and 6.20±1.9-7.95a±.76. The effect of guava was significant, p>0.05, for colour, texture, taste, crispiness and general acceptability. The relative increase in the average mean scores for texture could be due to the increasing fibre content of the guava with effect on the crispiness of the biscuit. The value for odour of the biscuits was not significantly different (p˂0.05) from each other. The sample, 95:5 % acha-guava blends is the most preferred and acceptable with average mean score of 7.95±.76. This effect on the sensory could be due to inherent flavor compounds in guava. Ayo & Gidado [3] reported a similar range for sensory qualities of acha-carrot biscuits and Dabels et al. [35] also reported similar range of wheat, acha and mung bean composite biscuit (Figure 2).
* Average mean score with the same letter(s) on the same column are not significantly different, p=0.05.
Conclusion
In conclusion, enriched biscuit with guava-flour substitutions were found to be nutritionally superior in fat content, fibre, iron, carotenoid total phenol, vitamin C and B1 respectively. The sample with 5% guava flour was most preferred corresponding relatively high improvement in the ash, fat, fibre, iron, carotenoid, vitamin C, total phenol and vitamin B1 content of the acha based biscuits. The appearance and crispiness of the acha-guava biscuit were greatly improved and acceptable.
The use of acha-guava flour blends in biscuits will go a long way in enhancing nutrition, health and wellbeing of the consumers and reduce the dependence on wheat flour. The properties of acha-guava could also make it a good candidate for use as edible blend and as raw material for several domestic and industrial purposes and in medical sector, acha could recommended as a dietary supplement for diabetic patients due to its high fibre content minerals and vitamins as result of added guava flour.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.business.site/
For more articles in Open Access Journal of Nutrition & Food Science please click on: https://juniperpublishers.com/nfsij/
To know more about Open Access Journals Publishers
To read more…Fulltext please click on: https://juniperpublishers.com/nfsij/NFSIJ.MS.ID.555727.php
47 notes
·
View notes
Text
Rethinking the Hospital Pharmacist Service: Centralized Logistics– Ict Systems and Clinical Pharmaceutical Care Strategies as a Management Opportunity for Public and Private Institutions-Juniper publishers
For more articles in Juniper Online Journal of Public Health please click on https://juniperpublishers.com/jojph/index.phpFor more Journals in Juniper Publishers please click on https://juniperpublishers.com/index.phpTo know more details regarding our Juniper publishers please click onhttps://juniperpublishers.business.site/Juniper Publishers- Juniper Online Journal of Public Health

Abstract
In last year’s healthcare costs are increased constantly in logarithmic way and this conditions need an high efficiently resource management system more than past. Drugs, medical devices, diagnostics or medical errors are relevant voice in the public and private hospital current budget and healthcare Institution and government tray every day to control it. (U.S. HEALTH national expenditure amounted total 3.0 -3billion U.S. D. The total spending on medicine in the USA was about 6 more than 400 us dollars in 2015).An high performance HEALTHCARE org. Need today: deep innovations, right management of materials (LOGISTICS drugs and medical devices use), new technologies knowledge, risk management skills and other resource.
Keywords: Change management; Hospital pharmacy; Innovation; Strategy; Healthcare; Pharmaceutical care and Clinical pharmacy; Logistics; Medical error; Clinical outcomes
Go to
Introduction
Strategic, change, knowledge management approach, sharing economy philosophy and other new instruments as velocity management [1] gives improving the global results. (Economic but also clinical). Also Multi-professional medical equip with permanent presence of the clinical pharmacists give improving in global results (clinical - economic outcomes) [2]. Risk management Reduce total costs due by therapy and other kind of error And gives solution to related problems in preventive and proactive way .The clinical pharmacists complete the patient medical team Adding deep pharmaceutical and pharmacological competencies (To prevent ADR, therapy errors, and monitoring the PHARMACOLOGICAL therapy) resulting in more containing in medical error. Inefficacy HR management gives high contributed in the TOTAL results [3] make possible rapid introduction of the different healthcare professionals in EQUIP.
But Today we have also a powerful instrument to efficacy control the costs to be used: centralized logistics systems (to reduce GLOBAL costs of drugs and medical device). The centralized logistic (and regional buying center) make possible a great rationalization in costs and in hospital pharmacy working time.
This system Increase the AMOUNT of orders (Cumulative way) and this make possible to have more discount in drug prices by pharmaceutical industries. The ordering by the different hospital linked and associated in this way this contribute to containing total costs more versus without this strategy. More over This make possible reduce hospital pharmacy stokes (immobilized drugs costs, less expiration data problems) giving the same time continuity to the therapy to the hospital wards in safety way. This systems need a just in time systems and a great support by ICT (healthcare professionals with informatics and data management knowledge.)The rapid communication with the hub and spoke make possible To have the drugs in strictly time.(we can think to saving life drugs especially).The hosp. pharmacist clinical competences gives the correct priority (in ordering procedure) and this is a crucial fact in the global management of the systems.
With centralized logistic need a small stoke of drugs in the hospital pharmacy whit 60-80 kind of molecules (critical medical devices and drugs) and an emergency ICU Drugs Cabinets to cover emergencies (if not ACTIVE an h24 hospital pharmacist service.) The great amount of drugs and medical devices are stoked in central ware house. This approach needs high expertise by the clinical hosp. pharmacist To rationalize the systems without error: right classification of critical drugs and an efficacy risk management system to prevent dis- functions (root cause analysis, FMEA approach, total quality management and other strategy). We can say that the clinical pharmacists works must be an edge between ward the hosp. pharmacy and the hub. (ICT mediated). Other instrument to manage at the right level can be Dose unit drug systems, informative prescription with applied software, oncologic unit’s sterile robot, emergency drugs cabinet systems and some other. All this rationalize the hospital global request of drugs and med devices but also reduce in high way therapy error. ICT technologies provide scurrility system to transfer patient and other data. The total knowledge is increased using these ICT systems. (Biomedical database for prevent interactions, contraindications and other).
But what is relevant in this new process is the active role of hospital clinical pharmacist in more consultant activity versus the classic logistic Functions. (A cultural changes) from the classic logistic function towards more clinical new pharmaceutical consultant functions. This make possible in the same time to adequately monitoring the healthcare costs (drugs and med. devices) containing medical and therapy error, improving also the clinical outcomes [2]. The application of clinical pharmacist presence in stabile way in medical team results in about 35 % cost reduction (drugs, med dev.), costs due by medical errors, reducing recovery days. In example, an Italian practical experience: health ministerial project: “Ward clinical pharmacists in oncology”[29]. A collaboration of: SIFO (Italian Society Hospital Pharmacy), Italian Federation of professional Pharmacists’ Orders, Italian assoc. Of Medical Oncology), EAHP (European Association of Hosp. Pharmacist), a multi-center experience involving 5 public hospitals with the presence of clinical pharmacists in the oncology wards. The result was a reduction of ward drug and MD stokes from 32% to 88% and 30% less of drugs therapy errors [29].
Related to these results. The managerial competences and skills and knowledge of the clinical pharmacist are often requested by general manager office and by physician’s director of the many discipline to monitoring and control the global buying systems [5]. Antimicrobial stewardship [7] , med. Gases pharmacy management , high cost drugs management , medical dev.high competencies ,Toxicological equip with hosp. pharmacists presence ,oncology lab ,ICU, nutrition team service , pain management medical equip , and other involving clinical pharmacist create an high synergy. Other relevant role can be played in surgery field [23] nephrology, heart disease and many other .In ex. the total cost for innovative drug therapy are under an high increase (therapy of hepatitis c ) , antimicrobials meet great resistance ,oncology therapy do not present equal efficacy towards all neo plastic tissue the same .“The economic aspect is relevant on cost of drugs and payment by government and institution or insurance. (In example 35.000 euro/USD/ patient for some biological MABS).Even ministry of health in some countries (ITALY) not pay all some new innovative drugs but use a system that verify the results obtained. (Payment by results or risk sharing et other procedure)” [6]. This problems need a deep and continuous high activity by clinical pharmacist to create a more rational decision making systems in today therapy world.
Go to
Material and Methods
In this observational and research work we report some relevant publications ( in our opinion ) involved in this change and related to the results we have find we submit to healthcare institution a new systems to efficacy control and reduce the healthcare costs improving clinical outcomes .We observe the hospital pharmacy organization in different countries in order to verify The organizational way of works .We describe also a practical research experience involved in management of emergency drug in hospital setting [24]. Then after this research we analyze the total costs involved in this kind of organization change and the advantages that can be obtained.
Go to
Result
Observing the hosp. pharmacy organization in many countries we can say that the pharmacy service is more oriented to the classic function as logistic, galenic lab, nutrition lab, dispensing activities and other.
But only few hosp. pharmacy service are highly oriented to advanced clinical function as advanced center usually do the same the university course involved in hospital pharmacy are more focused on the classic pharmacist function and only in recent decades towards more clinical Functions.(only few cases really involved in improving the clinical outcomes in medical team and not only with monitoring tasks). Also technology applications are not equally available to all hospital places. (Small – large hospitals, rural or city et other). From literature we have find this results: “During 1930 to 2016 a progressive development of clinical pharmacy and pharmaceutical care was developed. We have observed a “general positive influence of the pharmacist’s presence as a part of the medical equip, on public health in various clinical outcomes”; this according to systematic reviews, clinical trials and meta-analysis” [8]. “The model of clinical pharmacy practice adopted by many pharmacy department hospitals is no longer appropriate for the demands of today’s health-care services. Reviews many new models proposed for clinical pharmacy practice including an integrated model for providing a pharmaceutical care management approach in the health-care system. This model is a response to the failures of traditional drug and pharmacological therapy.
It is an idea about how health professionals should integrate their professional work to obtain clinical outcomes important to patients and clinicians” [9]. “Hospital information system is widely used to improve efficiency of china hospitals. A novel clinical pharmacy management system developed by our hosp. was introduced to improve work efficiency of clinical pharmacists, by providing pharmacy information services and promoting rational pharmacological drug use. Taking prescription review in the dep. of surgery, work efficiency of clinical pharmacists, quality and qualified rates of prescriptions before and after utilizing clinical pharmacy management system were compared. Qualified rates of both the inpatient and outpatient prescriptions of the general surgery department increased, antibiotics use decreased. This system apparently improved work efficiency standardized the level and accuracy of drug use, which will improve the rational drug use and pharmacy info service in our place. The utilization of prophylactic antibiotics for the aseptic operations reduced” [10].
“Clinical Pharmaceutical Care “as a new discipline, to improve clinical and economic endpoint in pharmacological therapy reducing therapy errors with a more rational use of resource in medical team. This new approach take advantages by Management discipline and ICT principles. Core training must include Management, ICT new social media, psychological behavior and other skills and attitudes for team working added to the classic clinical pharmacy core programs. The knowledge in field of diagnostic discipline gives great advantages in this field for the high relationship with much drug therapy [11]. “Based on the results of this study, the observed achievements were due to medical lab.
And imaging knowledge and competencies of the clinical pharmacist, as part of the equipe in a hospital setting. Such expertise of the clinical pharmacist has resulted in a significant impact on therapy. For patients’ safety and health and cost reduction and for clinical pharmaceutical care purposes, it is incumbent upon the hospitals to engage and demand an active role from clinical pharmacists, especially in fields such as diagnostics (med. Lab. and imaging) [12]. “to obtain more efficient results in improving some clinical outcomes the clinical pharmacist must have an expert skill in the field of psychological and behavior aspects to use a practical settings when member of medical team .Rotation in different wards provide a a real good experience. This skill and attitudes is useful in pharmacistspatients’ relationship in order to have high patient’s compliance level...” [13]. Reduction of medication therapy errors is needed and demanded by: patients, health authorities, government, insurances companies. “Multi professional healthcare team is the right way of work in health care today. A WARD clinical pharmacist today contributes in many fields: hematology oncology, toxicology, infectious diseases, emergency med., nephrology, nutrition pharmacy service, pain management and others” [11].
The clinical endpoints depend also by the med. device used and pharmacist specialist represents a great resource in cost containment in every level (to use the right one in every different situation) in this specific use. Ph. care principles can correctly be applied in themed. Devices dedicated to the single patient. Consultant activities in properties, classification, legislation, Alternative products, logistic are the working filed in which hospital pharmacist play a relevant roles in medical equipe” [14]. “The innovation introduced with biomed. Databases and searching engine motors improved research works with rapid ways in all kind of scientific areas Internet, and professional social media have brought a great development in rapidly connecting with professionals. The researchers in last 3 decades has been great possibility to share their practical experience more than past with improving results.
They are playing a crucial and relevant role today working field through this rapid development. LinkedIn, Slide share, Research gate, Pub Med, you tube NCBI, Facebook, and other etc. The possibility to create new bridge researchers; with similar interests, discipline with more rapid development ,never seen in last 3 decades”[15]. “In ICU we can see reduction in mortality rate when pharmacist takes really part of the equip. [12]. “Clinical Ph care required more use also of social media to meet researcher in more efficient way. In the same time clinical pharmacist can be a scientific edge between professional in therapy filed. PH care management can be useful tools to have more rational therapy systems.
Drugs are registered for specifically indication, and at the same time every drug to be a rational therapy need a rational decision making system that require a multidisciplinary equipe that can cover all aspect of Pharmaceutical and pharmacological molecular metabolism (also kinetics andPharmacodynamics) this have great possibility for clinical pharmacist but it must increase expertise in field of diagnostic (lab medicine and imaging) for the high relationship whit pharmacological drug therapy. The old algorithm was “physicians - patients - classic pharmacist and drugs “today it must be “patient physicians - clinical pharmacists (as consultant) and drug [16].
“Physicians alone cannot cover all aspect of the pharmacological treatment (for example in the field of drug therapy monitoring, interactions, adverse drug reaction ADR, toxicology, novel delivery systems, immune globulin-based) therapeutics and other innovative drugs and medical devices systems, which have their pharmaceutical specific worlds. This article likes to improve the ph. care application in countries with an advanced healthcare system to provide more rational drug therapy to patients. When not possible, it would be a good idea using ph. care, in particular populations such as: severe disease, critically ill, patients with multiple illnesses, transplants, immunosuppressant, oncology or other serious conditions, at least when the treatments cost a lot” [2]. Using sharing economy instruments we can reduce healthcare costs about 38 -40 % and obtain this results in more rapid way .The results obtained with sharing economy time can be applied in healthcare: sharing of knowledge“ICT systems can reduce errors and waste materials, rotation drugs and med. devices stokes and reducing costs: Dose unit systems and programs reduce costs about 10-15% and ward clinical pharmacist presence in stabile way in medical team can reduce cost about 25-30%.” (8)In a lancet infection disease meta-analysis was reported” Our findings of beneficial effects on outcomes with nine antimicrobial stewardship objectives suggest they can guide stewardship teams in their efforts to improve the quality of antibiotic use in hospitals [17].
According to last editorial The Clinical Pharmacists Main Focus. J Appl Pharma 9: e114 we can see that one of the main focus of the clinical pharmacist “must be applied in priority way to the most critical patients in order to achieve the best results available [12]. In this condition even benefit of 1 life achieved in mortality rate is a real golden endpoint (we can think for example to a pediatric poisoning, or severe infectious disease in pregnancy or the effect of inefficacy immunosuppressive therapy in transplanted et other) [13]. This can be considered in example as reduction in NNT to improve a therapeutic strategy” [18].
We have also see in some practical experience that the introduce in daily works of some technologies make possible a right management (reducing total costs and with safety) in example in emergency drug cabinet systems [7] “no near miss event or other patient risk or even fatal event was observed and was covered the the emergency need of drugs in the 99% of cases, and only 1 time was necessary the central pharmacy call.” (The same results we have observed during One year), we can have also a reduction in total costs providing an efficacy system .( about 50.000 euro in 5 years in an Italian public hospital 700 beds) [24]. Other ICT instruments are in examples dose unit system to provide single Unit of drugs (preventing waste or expiration of pharmacological therapies- full therapy traceability), informatics prescription software (to detect interactions, allergy, toxicity ),Informatics management of narcotic drugs or antidotes for right logistics and other.
Go to
Discussion
Analyzing the literature reported in this work and the results of a specific practical experience [24,28] we can say that using drugs central logistics (hub and spoke pharmacy system) added to ICT instrument and clinical pharmaceutical care and amore clinical pharmacy approach we can have reduced costs about 40%.This result not only due by drugs and med. devices costs rationalized but also by the reducing of med. errors, days of recovery and especially by improving clinical outcomes. In example the costs for an expensive transplant can be lost easy if not applied efficacy pharmacological drug therapy .(the same thinking about complex cardiac surgery or other critical and expensive patients situation).The pharmacist competences/ skills added to ADVANCED ICT INTRUMENTS can improve the global clinical results .This is the reason to shift from the classic logistic competences and skills of clinical pharmacist towards more and deep clinical tasks and to make an intensive ICT use as requested today.
Go to
Conclusion
We think that this kind of change in pharmaceutical dep. is today needed and this shift of hosp. pharmacist competence from the classic logistic roles towards more clinical /economic management tasks.gives reduction of 35-40%in healthcare total costs The application of clinical pharmacist to strictly control the prescription of drugs an M .DEV. (according protocols, guidelines, central - local rules ) make possible an great appropriateness verify [17,18]. We think that the efficacy instruments to the clinical pharmacist and healthcare institution to manage healthcare costs can be:
Management principles and TQM
Clinical Pharmaceutical care (new health care discipline) [19]
ICT technologies
Sharing economy principles of applications
The total costs involved in this change in working activities of hospital pharmacist are included in the costs rationalized by this new management system.(we can say that is not a cost but a resource.)Pharmacy must be considered not only like a definite fiscal place but a complex world where the consultant clinical activities can make the difference in patient outcomes (clinical, economic, quality of life)The core process must be a rethinking in hospital pharmacy competences enhancing the clinical competences level and time dedicated to this specific tasks. This kind of process must involve politics stakeholders institution, healthcare org., decision making hospital general managers, universities and the same all healthcare Professional [20-25].
The principal goal is obtained if this change is accepted by all. The actors and professionals involved in healthcare management agree with this new approach. But is crucial that the same hosp. pharmacist know that in this new organization system other specific kind of responsibility are involved in direct patient clinical pharmacy and pharmaceutical care works .The experience we have see [7] can be usefully transferred to other hospital and other situations giving good results [26,27].
For more articles in Juniper Online Journal of Public Health please click on https://juniperpublishers.com/jojph/index.php
For more Journals in Juniper Publishers
please click on https://juniperpublishers.com/index.php
To know more details regarding our Juniper publishers please click on
https://juniperpublishers.business.site/
#public health#health journals#open acess journal#Online Journal of Public Health#journal of public health
0 notes