
indy-gray
Great Hall of Unfinished WIPs
Indy | she/her they/them | wlw fantasy and scifi is what I do | tag friendly, if you want to show me something tag me in it | no concept of the passage of time so I'm always horribly late to the party | adult so some of my content is not suitable for minors
2040 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

automaticlanddreamer
Tanpa judul

clyches
cly

archivemagic
Cheshire

baublefobbersleuth
Shed Down By The River

lilypadmomentum
A certified Zoro simp
Text
"we need less sanitized queer stories" yall keep saying fucking she-ra romanticizes abuse. you couldnt possibly handle less sanitized queer stories
67K notes
·
View notes

Text
Writing Mental Health With Compassion
I've gotten a few questions regarding depicting characters with mental health challenges and conditions and I wanted to expand a little more on how to depict these characters with compassion for the real communities represented by these characters.
A little about this guide: this is, as always, coming from a place of love and respect for the writing community and the groups affected by this topic at large. I'm also not coming at this from the outside, I have certain mental illnesses that affect my daily life. With that, I'll say that my perspective may be biased, and as with all writing advice, you should think critically about what is being told to you and how.
So let's get started!
Research
I'm sure we're all tired of hearing the phrase "do your research," but unfortunately it is incredibly important advice. I have a guide that touches on how to do research here, if you need a place to get started.
When researching a mental health condition that we do not experience, we need to do so critically, and most importantly, compassionately. While your characters are not people, they are assigned traits that real people do have, and so your depiction of these traits can have an impact on people who face these conditions themselves.
I've found that reddit is a decent resource for finding threads of people talking about their personal experiences with certain illnesses. For example, bipolar disorder has several subreddits that have very open and candid discussions about bipolar, how it impacts lives, and small things that people who don't have bipolar don't tend to think about.
It's important to note that these spaces are not for you. They are spaces for people to talk about their experiences in a place without judgment or fear or stigma. These are not places for people to give out writing advice. Do NOT flood subreddits for people seeking support with questions that may make others feel like an object to be studied. It's not cool or fair to them for writers to enter their space and start asking questions when they're focused on getting support. Be courteous of the people around you.
Diagnosis
I have the belief that for most stories, a diagnosis for your characters is unnecessary. I have a few reasons for thinking this way.
Firstly, mental health diagnoses are important for treatment, but they're also a giant sign written across your medical documents that says, “I'm crazy!” Doctors may try to remain unbiased when they see mental health diagnoses, but anybody with a diagnosis can say that doctors rarely succeed. This translates to a lot of people never getting diagnoses, never seeking treatment, or refusing to talk about their diagnosis if they do have one.
Secondly, I've seen posts discuss “therapy speak” in fiction, and this is one of those instances where a diagnosis and extensive research may make you vulnerable to it. People don't tend to discuss their diagnoses freely and they certainly don't tend to attribute their behaviors as symptoms.
Finally, this puts you, the writer, into a position where you treat your characters less like people and story devices and more like a list of symptoms and behavioral quirks. First and foremost, your characters serve your story. If they don't feel like people then your characters may fall flat. When it comes to mental illness in characters, the people aspect is the most important part. Mentally ill people are people, not symptoms.
Those are my top three reasons for believing that most characters will never need a specific diagnosis. You will likely never need to depict the difference between bipolar and borderline because the story itself does not need that distinction or to reveal a diagnosis at all. I feel that having a diagnosis in mind for a character has more pitfalls than advantages.
How does treatment work?
Treating mental health conditions may appear in your story. There are a number of ways treatments affect daily life and understanding the levels of care and what those levels treat will help you depict the appropriate settings for your characters.
The levels of care range from minimally restrictive and minimal care to intensive in-patient care in a secure hospital setting.
Regular or semi-regular therapy is considered outpatient care. This is generally the least restrictive. Your characters may or may not also take medications, in which case they may also see a psychiatrist to prescribe those medications. There is a difference between therapists, psychiatrists, and psychologists. Therapists do not prescribe medications, psychiatrists prescribe medications after an evaluation, and psychologists will (sometimes) do both. (I'm US, so this may work differently depending where you are. You should always research the specific setting of your story.) Generally, a person with a mental illness or mental health condition will see both an outpatient therapist and an outpatient psychiatrist for their general continuing care.
Therapists will see their patients anywhere from once in a while as-needed to twice weekly. Psychiatrists will see new patients every few weeks until they report stabilizing results, and then they will move to maintenance check-ins every 90-ish days.
If the patient reports severe symptoms, or worsening symptoms, they will be moved up to more intensive care, also known as IOP (Intensive Outpatient Program). This is usually a group-therapy setting for between 3-7 hours per day between 3-5 days a week. The group-therapy is led by a Licensed Professional Counselor (LPC) or Licensed Professional Social Worker (LPSW). Groups are structured sessions with multiple patients teaching coping mechanisms and focusing on treatment adjustment. IOP’s tend to expect patients to see their own outpatient psychiatrist, but I've encountered programs that have their own in-house psychiatrists.
If the patient still worsens, or is otherwise needing more intensive care, they'll move up to PHP (Partial Hospitalization Program). This can look different per facility, but I've seen them to be more intensive in hours and content than IOP. They also usually have in-house psychiatrists doing diagnostic psychological evaluations. It's very possible for characters with “mild” symptoms to go long periods of time, even most of their lives, without having had a diagnosis. PHP’s tend to need a diagnosis so that they can address specific concerns and help educate the patient on their condition and how it may manifest.
Next step up is residential care. Residential care is a boarding hospital setting. Patients live in the hospital and focus entirely on treatment. Individual programs may differ in what's allowed in, how much contact the patients are allowed to have, and what the treatment focus is. Residential programs are often utilized for addiction recovery. Good residential programs will care about the basis for the addiction, such as underlying mental health issues that the patient may be self-medicating for. Your character may come away with a diagnosis, or they may not. Residential programs aren't exclusively for addictions though, and can be useful for severe behavioral concerns in teenagers or any number of other concerns a patient may have that manifest chronically but do not require intensive inpatient restriction.
Inpatient hospital stays are the highest level of care, and this tends to be what people are talking about when they tell jokes about “grippy socks.” These programs are inside the hospital and patients are highly restricted on what they can and cannot have, they cannot leave unless approved by the hospital staff (the hospital's psychiatrist tends to have the final say), and contact with the outside world is highly regulated. During the days, there are group therapy sessions and activities structured very carefully to maintain routine. Staff will regulate patient hygiene, food and sleep routines, and alone time.
Inpatient hospital programs are controversial among people with mental illness and mental health concerns. I find that they have use, but they are also not an easy or first step to take when dealing with a mental health condition. Patients are not allowed sharp objects, metal objects, shoelaces, cutlery, and pens or pencils. Visitors are not allowed to bring these items in, staff are not allowed these items either. This is for the safety of the patients. Typically, if someone is involuntarily admitted into the inpatient hospital program, it is due to an authority (the hospital staff) deeming the patient as a danger to themselves or others. Whether they came in of their own will (voluntary) or not does not matter in how the program operates. Everyone is treated the same. If someone is an active danger to themselves, then they may be on 24-hour suicide watch. They are not allowed to have any time alone. No, not even for the bathroom, or while sleeping, or during group sessions.
Inpatient Hospital Programs
This is a place of high curiosity for those who have never been admitted into inpatient care, so I'd like to explain a little more in detail how these programs work, why they're controversial, but how they can be useful in certain situations. I do have personal experience in this area, but as always, your mileage may vary.
When admitting, hospital staff are the final say. Not the police. The police hold some sway, but most often, if someone is brought in by the police, they are likely to be admitted. They are only involuntarily admitted when the situation demands: the staff have determined the person to be an imminent danger to themselves or others. This is obviously subjective, and can easily be abused. A good program with decent staff will do everything they can to convince the patient to admit voluntarily if they feel it is necessary, but ultimately if the patient declines and the staff don't feel they can make the clinical argument that admittance is necessary, the patient is free to leave. It should be noted that doctors and clinicians have to worry about possibly losing their licenses to practice. They don't want to fuck around with involuntary admittance if they don't have to, and they don't want potentially dangerous people to walk away.
Once admitted, the patient will have to remove their clothing and put on a set of hospital scrubs. These are mostly made of paper, and most often do not have pockets, but I have seen sets that do have pockets (very handy, tbh). They are not allowed to take anything into the hospital wing except disability-required devices such as glasses, hearing aids, mobility aids, etc. Most programs will require removing piercings, but not all of them, in my experience.
The nurses will also do a physical examination, where they will make note of any open wounds, major scars, tattoos, and other skin abrasions that may be relevant.
The patient will then be led to their bed, where they will receive any approved clothing items from outside, a copy of their patient rights, and a copy of the floor code of conduct and rules, a schedule, and any other administrative information necessary for the program to run efficiently and legally.
Group sessions include group-therapy, activities, coping skills, anger management, anxiety management, and for some reason, karaoke. There is a lot of coloring involved, but only with crayons. A good program will focus heavily on skills and therapeutic activities. Bad programs will phone it in and focus on karaoke and activities. Most hospitals will have a chaplain, and some will include a religious group session. I've never attended these, so I can't speak for them.
Unspoken rules are the hidden pieces of the inpatient programs that patients tend to find out during their first visit. There is no leaving the program until the doctor agrees to it. The doctor will only agree to it if they deem you ready to leave, and you are only ready to leave if you have been compliant to treatment and have seen positive results in the most dangerous symptoms (homicidal or suicidal ideations). Noncompliance can look like: refusing your prescribed medications (which you have the right to do at any time for any reason. That does not mean that there won't be consequences. This is a particularly controversial point.), refusing to attend groups (chapel is not included in this point, but that doesn't mean it's actually discounted. Another controversial point.), violent or disruptive outbursts such as yelling or throwing things, and refusing to sleep or eat at the approved and appointed times. All of this may sound like the hospital is restricting your rights beyond reason, but I've seen the use, and I've seen the abuse. Medications are sometimes necessary, and often patients seriously prefer having medication. Groups are important to a person's treatment, and refusing to go can be a sign of noncompliance or worsening symptoms. If someone is too depressed or anxious to go to group, then they're probably not ready to leave the hospital where the structure is gone and they must self-regulate their treatment. Violent or disruptive outbursts tend to be a sign of worsening symptoms in general, but even the best of us lose our tempers from time to time when put into a highly stressful situation like an inpatient hospital stay. The hospital is supposed to be a place of healing, for many it is. But for many more, it is a place of systematic abuse and restriction.
Discharge processes can be long and arduous and INCREDIBLY stressful for the patient. Oftentimes, they won't know their discharge date until the day of, or perhaps the day before. Though the date can change at any time. The discharge process requires the supervising psychiatrist to meet with the treatment team and then the patient to determine if the patient had progressed enough to be safely discharged. Discharge also requires a set outpatient plan in place, such as a therapy appointment within a week, a psychiatrist visit, or admittance into a lower level of care. This is where social workers are involved. Patients are not allowed access to cell phones or the internet. They cannot make their own appointments with their outpatient care providers without a phone number and phone access. Some floors will have phone access for this reason, others will insist the social worker arrange appointments and discharge plans. Social workers are often incredibly overworked, with several patients on their caseload.
The patient cannot be discharged until the social worker has coordinated the discharge plan to the doctor's approval. Most often, unfortunately, the patient rarely receives regular communication regarding the progress of their discharge. I've been discharged with as much as a day's notice to two hours notice.
Part 2 Coming Soon
This guide got longer than expected! Out of respect for my followers dashboard, I will be cutting it here and adding a Part 2 later on.
If you find that there are more specific questions you'd like answered, or topics you'd like covered, send an ask or reply to this post with what you'd like to see in Part 2.
– Indy
154 notes
·
View notes
Text
My face is having uncontrollable spasms. Great. It hurts really, really, really bad.
I think part of why I have trouble explaining pain to the doctor is when they ask about the pain scale I always think “Well, if someone threw me down a flight of stairs right now or punched me a few times, it would definitely hurt a lot more” so I end up saying a low number. I was reading an article that said that “10” is the most commonly reported number and that is baffling to me. When I woke up from surgery with an 8" incision in my body and I could hardly even speak, I was in the most horrific pain of my life but I said “6” because I thought “Well, if you hit me in the stomach, it would be worse.”
#relevant to my life right now with this migraine#they keep asking me about my pain scale and i keep saying 5 or 6#and they kind of roll their eyes#but according to this scale im at an 8 mever dropping below a 7. huh
338K notes
·
View notes
Text
never let anyone tell you that trawling through mediocre victorian poetry isn't worth it. we just happened upon an absolute BANGER of a worm poem. go read it or else 🪱🪱🪱
#this is the poem that made poetry click in my brain#i never understood poetry and always felt so stupid for it but this poem#this poem changed everything i think
63K notes
·
View notes
Text
Writing Mental Health With Compassion
I've gotten a few questions regarding depicting characters with mental health challenges and conditions and I wanted to expand a little more on how to depict these characters with compassion for the real communities represented by these characters.
A little about this guide: this is, as always, coming from a place of love and respect for the writing community and the groups affected by this topic at large. I'm also not coming at this from the outside, I have certain mental illnesses that affect my daily life. With that, I'll say that my perspective may be biased, and as with all writing advice, you should think critically about what is being told to you and how.
So let's get started!
Research
I'm sure we're all tired of hearing the phrase "do your research," but unfortunately it is incredibly important advice. I have a guide that touches on how to do research here, if you need a place to get started.
When researching a mental health condition that we do not experience, we need to do so critically, and most importantly, compassionately. While your characters are not people, they are assigned traits that real people do have, and so your depiction of these traits can have an impact on people who face these conditions themselves.
I've found that reddit is a decent resource for finding threads of people talking about their personal experiences with certain illnesses. For example, bipolar disorder has several subreddits that have very open and candid discussions about bipolar, how it impacts lives, and small things that people who don't have bipolar don't tend to think about.
It's important to note that these spaces are not for you. They are spaces for people to talk about their experiences in a place without judgment or fear or stigma. These are not places for people to give out writing advice. Do NOT flood subreddits for people seeking support with questions that may make others feel like an object to be studied. It's not cool or fair to them for writers to enter their space and start asking questions when they're focused on getting support. Be courteous of the people around you.
Diagnosis
I have the belief that for most stories, a diagnosis for your characters is unnecessary. I have a few reasons for thinking this way.
Firstly, mental health diagnoses are important for treatment, but they're also a giant sign written across your medical documents that says, “I'm crazy!” Doctors may try to remain unbiased when they see mental health diagnoses, but anybody with a diagnosis can say that doctors rarely succeed. This translates to a lot of people never getting diagnoses, never seeking treatment, or refusing to talk about their diagnosis if they do have one.
Secondly, I've seen posts discuss “therapy speak” in fiction, and this is one of those instances where a diagnosis and extensive research may make you vulnerable to it. People don't tend to discuss their diagnoses freely and they certainly don't tend to attribute their behaviors as symptoms.
Finally, this puts you, the writer, into a position where you treat your characters less like people and story devices and more like a list of symptoms and behavioral quirks. First and foremost, your characters serve your story. If they don't feel like people then your characters may fall flat. When it comes to mental illness in characters, the people aspect is the most important part. Mentally ill people are people, not symptoms.
Those are my top three reasons for believing that most characters will never need a specific diagnosis. You will likely never need to depict the difference between bipolar and borderline because the story itself does not need that distinction or to reveal a diagnosis at all. I feel that having a diagnosis in mind for a character has more pitfalls than advantages.
How does treatment work?
Treating mental health conditions may appear in your story. There are a number of ways treatments affect daily life and understanding the levels of care and what those levels treat will help you depict the appropriate settings for your characters.
The levels of care range from minimally restrictive and minimal care to intensive in-patient care in a secure hospital setting.
Regular or semi-regular therapy is considered outpatient care. This is generally the least restrictive. Your characters may or may not also take medications, in which case they may also see a psychiatrist to prescribe those medications. There is a difference between therapists, psychiatrists, and psychologists. Therapists do not prescribe medications, psychiatrists prescribe medications after an evaluation, and psychologists will (sometimes) do both. (I'm US, so this may work differently depending where you are. You should always research the specific setting of your story.) Generally, a person with a mental illness or mental health condition will see both an outpatient therapist and an outpatient psychiatrist for their general continuing care.
Therapists will see their patients anywhere from once in a while as-needed to twice weekly. Psychiatrists will see new patients every few weeks until they report stabilizing results, and then they will move to maintenance check-ins every 90-ish days.
If the patient reports severe symptoms, or worsening symptoms, they will be moved up to more intensive care, also known as IOP (Intensive Outpatient Program). This is usually a group-therapy setting for between 3-7 hours per day between 3-5 days a week. The group-therapy is led by a Licensed Professional Counselor (LPC) or Licensed Professional Social Worker (LPSW). Groups are structured sessions with multiple patients teaching coping mechanisms and focusing on treatment adjustment. IOP’s tend to expect patients to see their own outpatient psychiatrist, but I've encountered programs that have their own in-house psychiatrists.
If the patient still worsens, or is otherwise needing more intensive care, they'll move up to PHP (Partial Hospitalization Program). This can look different per facility, but I've seen them to be more intensive in hours and content than IOP. They also usually have in-house psychiatrists doing diagnostic psychological evaluations. It's very possible for characters with “mild” symptoms to go long periods of time, even most of their lives, without having had a diagnosis. PHP’s tend to need a diagnosis so that they can address specific concerns and help educate the patient on their condition and how it may manifest.
Next step up is residential care. Residential care is a boarding hospital setting. Patients live in the hospital and focus entirely on treatment. Individual programs may differ in what's allowed in, how much contact the patients are allowed to have, and what the treatment focus is. Residential programs are often utilized for addiction recovery. Good residential programs will care about the basis for the addiction, such as underlying mental health issues that the patient may be self-medicating for. Your character may come away with a diagnosis, or they may not. Residential programs aren't exclusively for addictions though, and can be useful for severe behavioral concerns in teenagers or any number of other concerns a patient may have that manifest chronically but do not require intensive inpatient restriction.
Inpatient hospital stays are the highest level of care, and this tends to be what people are talking about when they tell jokes about “grippy socks.” These programs are inside the hospital and patients are highly restricted on what they can and cannot have, they cannot leave unless approved by the hospital staff (the hospital's psychiatrist tends to have the final say), and contact with the outside world is highly regulated. During the days, there are group therapy sessions and activities structured very carefully to maintain routine. Staff will regulate patient hygiene, food and sleep routines, and alone time.
Inpatient hospital programs are controversial among people with mental illness and mental health concerns. I find that they have use, but they are also not an easy or first step to take when dealing with a mental health condition. Patients are not allowed sharp objects, metal objects, shoelaces, cutlery, and pens or pencils. Visitors are not allowed to bring these items in, staff are not allowed these items either. This is for the safety of the patients. Typically, if someone is involuntarily admitted into the inpatient hospital program, it is due to an authority (the hospital staff) deeming the patient as a danger to themselves or others. Whether they came in of their own will (voluntary) or not does not matter in how the program operates. Everyone is treated the same. If someone is an active danger to themselves, then they may be on 24-hour suicide watch. They are not allowed to have any time alone. No, not even for the bathroom, or while sleeping, or during group sessions.
Inpatient Hospital Programs
This is a place of high curiosity for those who have never been admitted into inpatient care, so I'd like to explain a little more in detail how these programs work, why they're controversial, but how they can be useful in certain situations. I do have personal experience in this area, but as always, your mileage may vary.
When admitting, hospital staff are the final say. Not the police. The police hold some sway, but most often, if someone is brought in by the police, they are likely to be admitted. They are only involuntarily admitted when the situation demands: the staff have determined the person to be an imminent danger to themselves or others. This is obviously subjective, and can easily be abused. A good program with decent staff will do everything they can to convince the patient to admit voluntarily if they feel it is necessary, but ultimately if the patient declines and the staff don't feel they can make the clinical argument that admittance is necessary, the patient is free to leave. It should be noted that doctors and clinicians have to worry about possibly losing their licenses to practice. They don't want to fuck around with involuntary admittance if they don't have to, and they don't want potentially dangerous people to walk away.
Once admitted, the patient will have to remove their clothing and put on a set of hospital scrubs. These are mostly made of paper, and most often do not have pockets, but I have seen sets that do have pockets (very handy, tbh). They are not allowed to take anything into the hospital wing except disability-required devices such as glasses, hearing aids, mobility aids, etc. Most programs will require removing piercings, but not all of them, in my experience.
The nurses will also do a physical examination, where they will make note of any open wounds, major scars, tattoos, and other skin abrasions that may be relevant.
The patient will then be led to their bed, where they will receive any approved clothing items from outside, a copy of their patient rights, and a copy of the floor code of conduct and rules, a schedule, and any other administrative information necessary for the program to run efficiently and legally.
Group sessions include group-therapy, activities, coping skills, anger management, anxiety management, and for some reason, karaoke. There is a lot of coloring involved, but only with crayons. A good program will focus heavily on skills and therapeutic activities. Bad programs will phone it in and focus on karaoke and activities. Most hospitals will have a chaplain, and some will include a religious group session. I've never attended these, so I can't speak for them.
Unspoken rules are the hidden pieces of the inpatient programs that patients tend to find out during their first visit. There is no leaving the program until the doctor agrees to it. The doctor will only agree to it if they deem you ready to leave, and you are only ready to leave if you have been compliant to treatment and have seen positive results in the most dangerous symptoms (homicidal or suicidal ideations). Noncompliance can look like: refusing your prescribed medications (which you have the right to do at any time for any reason. That does not mean that there won't be consequences. This is a particularly controversial point.), refusing to attend groups (chapel is not included in this point, but that doesn't mean it's actually discounted. Another controversial point.), violent or disruptive outbursts such as yelling or throwing things, and refusing to sleep or eat at the approved and appointed times. All of this may sound like the hospital is restricting your rights beyond reason, but I've seen the use, and I've seen the abuse. Medications are sometimes necessary, and often patients seriously prefer having medication. Groups are important to a person's treatment, and refusing to go can be a sign of noncompliance or worsening symptoms. If someone is too depressed or anxious to go to group, then they're probably not ready to leave the hospital where the structure is gone and they must self-regulate their treatment. Violent or disruptive outbursts tend to be a sign of worsening symptoms in general, but even the best of us lose our tempers from time to time when put into a highly stressful situation like an inpatient hospital stay. The hospital is supposed to be a place of healing, for many it is. But for many more, it is a place of systematic abuse and restriction.
Discharge processes can be long and arduous and INCREDIBLY stressful for the patient. Oftentimes, they won't know their discharge date until the day of, or perhaps the day before. Though the date can change at any time. The discharge process requires the supervising psychiatrist to meet with the treatment team and then the patient to determine if the patient had progressed enough to be safely discharged. Discharge also requires a set outpatient plan in place, such as a therapy appointment within a week, a psychiatrist visit, or admittance into a lower level of care. This is where social workers are involved. Patients are not allowed access to cell phones or the internet. They cannot make their own appointments with their outpatient care providers without a phone number and phone access. Some floors will have phone access for this reason, others will insist the social worker arrange appointments and discharge plans. Social workers are often incredibly overworked, with several patients on their caseload.
The patient cannot be discharged until the social worker has coordinated the discharge plan to the doctor's approval. Most often, unfortunately, the patient rarely receives regular communication regarding the progress of their discharge. I've been discharged with as much as a day's notice to two hours notice.
Part 2 Coming Soon
This guide got longer than expected! Out of respect for my followers dashboard, I will be cutting it here and adding a Part 2 later on.
If you find that there are more specific questions you'd like answered, or topics you'd like covered, send an ask or reply to this post with what you'd like to see in Part 2.
– Indy
154 notes
·
View notes
Text
I like how I said a while ago I was thinking about returning to Tumblr and then I like... didn't
Anyway what's up homies I'm about to rebrand in a little bit I think. I've had some weird gender fuckery going on and I've decided that I probably will not be transitioning sooooo I'm just gonna like, pick a different pen name that may or may not be my actual name? Idk yet we'll see I'm at work
4 notes
·
View notes
Text
Psst reblog this and describe a scene you're looking forward to writing in the tags
#okay so like the scene im looking forward to most is when Anya and Bo reunite#for the first time after bo's first 'death'#its going to be so angsty and good#bo doesnt know she died in Anya's arms with only half a face#and anya is terrified to be hopeful that bo is real#and bo is bo is so real#but bo doesnt remember anything from their escape its just blank#anya is cursed to remember while bo is cursed to forget#and they love each other so dearly#bo would die for anya but thats not saying much at all because bo would die for anybody or anything#and so anya can never know how much it tears bo up inside to leave her behind every time
109 notes
·
View notes
Text
Shadow's speech is actually so interesting like he'd be a speech-language pathologist's wet dream. His accent is complicated because he barely has a primary language. He learned Russian and English at about the same time as a young child and the other languages he speaks followed very closely/simultaneously after that. He has an American accent when he speaks languages other than English except for Russian in which he doesn't have much of any accent besides like. Russian. To Americans though he sounds like a blend of some kind of European accent and what's best described as a Disney Channel vibe, mainly from watching a lot of the disney channel to learn English.
Then there's his speech patterns which I won't go into too much but an interesting one is that he has a habit of repeating a word with a synonymous phrase.
Ex: "We did things equally, the same amount." Or "My fucking phone disappeared, it was here and then it wasn't."
He does this (subconsciously) in case he used the first word wrong, which he does do frequently. So it saves time just to add on what he means.
#i log on. i see something about shadow. i become more intrigued by this weird little guy.#this is a cool set of character traits to give a character tho and its interesting to see it come to life#the detail is exquisite
16 notes
·
View notes
Text
If there's anything that'll turn me into a toxic man-hating lesbian it's women's athletics.
Like okay yeah ball size in women's rugby is the problem and totally not the prevalent misogyny in the way women's sport is marketed, shown, and trained. Sincerely fuck all of you.
Like world rugby guidelines talking about "right brain" and "left brain" gender research old enough to vote but refusing to put any thought or nuance into trans player policies and just outright banning trans players altogether? Fuck you.
Sports institutions would rather the "problem" of women's sports to just go away rather than lean into the MASSIVE market there is for women athletics. I mean, Caitlin Clark in collegiate US athletics has made a bigger impact on the world of sports than any big name male international soccer player idgaf.
Like, shattering records and skyrocketing to fame as an athlete in men's sports is like a drop in the bucket of importance to sport than it is to be such a prolific athlete that viewership statistics stagger marketing experts around the world for singular women's games in tiny (comparatively) country specific sports.
What's more impressive, an international soccer superstar jumping viewership by 44% but not even topping number of viewers total from a game that happened 13 years ago, or a college-level basketball player drawing such a huge crowd that she eclipses viewership of the most popular sport in the world debuting the most popular athlete in the world in a new league by 18.5 million viewers?
Over and over and over again women's sports are proving that there's a huge audience here, and yet there's still shit stain men out here claiming women's sports are still "boring" like tell me you never have been and never will get laid without telling me you're a raging misogynist.
Women's MMA is floundering with lack of athletes, women's soccer athletes are struggling to pay their bills, the Dallas area of the US has lost 70% of their adult women's club rugby teams in the last five years. The problem is not that women's sports aren't interesting, it's that men are actively sabotaging women's sports. I'm tired of the distracting discoursers and the stupid rule changes and the insincere concern for athlete safety.
You want athlete safety? Fuck off about trans players and start ousting the sexual predators on coaching staffs and executive boards. Want a faster game? Invent one idgaf. Want advertising money? TELEVISE WOMENS SPORTS.
Women have been screaming into the void for decades about all the issues with women's sports and none of them involved trans athletes or rule changes. Talk about rule changes when you've handled the sexual harassment and assault, the pay disparities, the air time disparity, the funding disparity, the discrimination, the racism, the disregard for world class athletes thriving in their sport.
🖕🖕🖕🖕
#im just so fucking done with men rn#brought to you by: i couldnt close the instagram comment section fast enough after i accidentally clicked the wrong damn button
2 notes
·
View notes
Text
i love being a hater of media that i’ve never seen or listened to. no i will not give it a chance. it’s called listening to my heart
25K notes
·
View notes
Text
Some of yall are weirdly comfortable assuming there's malice when there is none and that harm can only be imposed intentionally. Your life will be better and you will be way less angry if you acknowledge that you can't read minds.
3 notes
·
View notes



Text
Unpopular opinion: the "i never actually write"/"wrestling with a blank page" memes are barely funny and deeply unhelpful
I'll throw in a follow-up for free: qualifying your community engagement with interaction statistics is a non-starter because that's not how social media works
UNPOPULAR WRITEBLR OPINIONS go go go
I'll start: editing the first draft is fine, actually
429 notes
·
View notes
Text
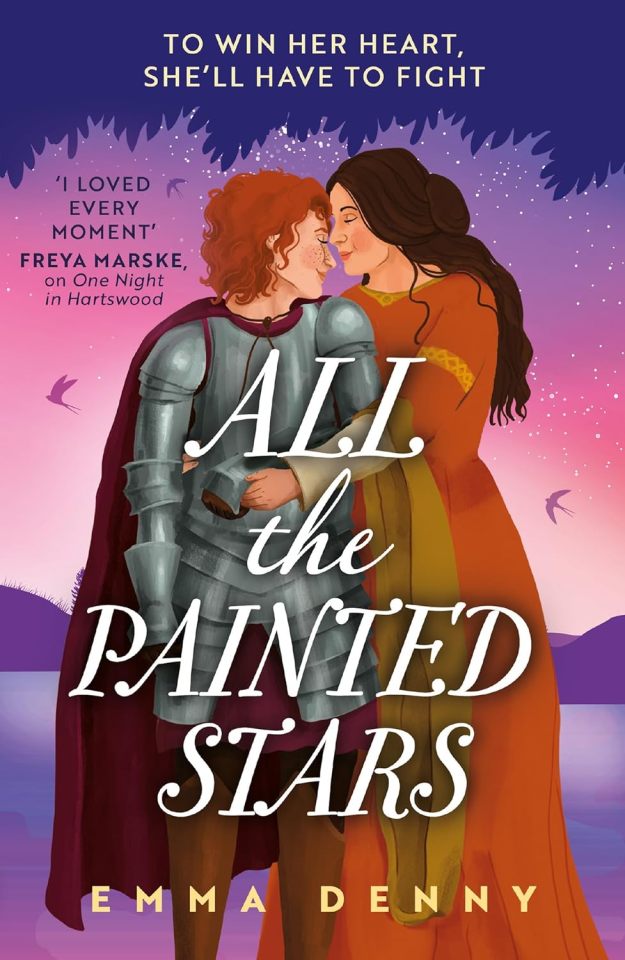
What do you do when you hear your best friend's hand in marriage is the grand prize in a tournament? You steal your brother's armour, cut off all your hair, and enter in disguise to rescue her. Obviously.
All The Painted Stars is a sapphic, medieval romance novel with...
⭐ Knight's Tale Vibes
⭐ Women in armour
⭐ Skinny dipping
⭐ Ruining arranged marriages
⭐ The pain of being in love with your best friend
It's OUT NOW wherever books are sold in paperback, ebook and audiobook!
Bookshop.org / Waterstones / Blackwells / Amazon / Kobo
Full blurb & content warnings under the cut.
Oxfordshire 1362
When Lily Barden discovers her best friend Johanna’s hand in marriage is being awarded as the main prize at a tournament, she is determined to stop it. Disguised as a knight, she infiltrates the contest, preparing to fight for Jo’s hand. But her conduct ruffles feathers, and when a dangerous incident escalates out of Lily’s control, Jo must help her escape.
Finding safety with a local brewster, Lily and Jo soon settle into their new freedom, and amongst blackberry bushes and lakeside walks an unexpected relationship blossoms. But when Jo’s past catches up with her and Lily’s reckless behaviour threatens their newfound happiness, both women realise that love must always come at a cost.
Content warnings:
ATPS contains mention of past emotional and physical abuse, and some mild violence.
It also contains explicit on-page sex scenes.
2K notes
·
View notes

Text
The bridge that collapsed today in Baltimore is the bridge by my childhood home. My family and friends are okay, but this is a major catastrophe for my community. I hope they can still find survivors but knowing that water, I'm doubtful
1 note
·
View note