aisha-ot
OT Journey
Travel diaries with an OT spin
14 posts
Don't wanna be here? Send us removal request.
Last Seen Blogs

vampirechatroom
أوي شكد حلوة الحرية


hallowxiu
MAMMON'S GROWL

softestaura
softestaura

unidentified-walking-object
Unidentified Walking Object
Text
Hi friends,
My time working in the community is coming to an end and it's almost time for me to pass the torch onto the next round of students. So this week I thought it would be a good idea to discuss a few lessons I've learnt throughout my experience so that you also get to light a torch and join the community practice journey. I can clearly see how much I’ve grown and how my OT knowledge has both expanded and been consolidated at the same time. Although these past few weeks have been physically and mentally challenging, it has opened my mind to new concepts and ideas that will guide my OT practice for the rest of my career. Let's get into what I've learnt throughout my time in the community as I wrap up and hand over to the next group of students.
We already know I talk too much by now so I'm going to try and make this one a bit quicker by speaking on 4 different points.
Holistic approach
Ok, this one is going to be a quick one because I feel like I've spoken about it so often throughout my time in the community.
I came into community not knowing what was about to hit me. Little did I know, my physical, psych and pediatric theory was about to slap me in the face. We always talk about occupational therapy being a holistic approach but I never really understood it in practice until now. Community based practice really makes you consider every single aspect of a person. I needed to consider not only their physical problems but their mental and emotional state, their socio-economic status, their environmental context within the community and their culture and religion in order to determine an appropriate way of approaching them and developing interventions. Although we are taught to have a holistic approach throughout the OT curriculum, I feel as though working in the community is the turning point that really allowed me to understand what it means in practice.
Cultural competence
This is not to say that cultural competence is something new to me. I did come into the community knowing that I need to be culturally competent and sensitive. It's something that is part of our every day practice. But, my experiences have expanded this concept.
The culture and stigma related to certain things in the community is something I needed to experience first hand and wrap my head around. I knew that there is a lot of stigma attached to HIV but I needed to do a bit more research to fully understand why. In my research I came across this article that includes a first hand experience of a South African woman who was diagnosed with HIV. It explains that women face consequences of physical violence and abuse along with the mental and emotional factors that come with processing the diagnosis. The beginning of the article in particular is what caught my attention as it explained a story of a woman who stepped into oncoming traffic to kill herself as soon as she left the clinic and found out she had HIV due to the social and cultural consequences. That is the extent of HIV stigma for women in South Africa. I suggest you give the article a read, it really captures you and allows you to grasp the extent of the stigma attached to HIV.
Majority of the clients I had in the clinic were HIV positive. This means that I had to speak to them about HIV and health management and determine their compliance with medications etc. But most of the patients showed discomfort and panic when speaking about the topic. They would look around if others were listening because they didn't want people to hear. After reading the above article, my understanding of why this is was deepened. Although we do need to change the narrative about HIV in South Africa, as a therapist I needed my client to trust me and openly speaking about her HIV diagnosis was not how I was going to achieve that. Working in a setting with no privacy allowed me to learn from my mistakes. I did initially speak to a client about HIV with others around and observed her discomfort which I immediately regretted. But it did show me the extent of the stigma attached to HIV in the community and helped me change my approach so that I'm more mindful and ethical when addressing these topics.
3. Approaching men in the community
On the first day of clinic in the community I knew this was going to be a struggle for me. I had approached a number of men in the clinic line and every single man had either ignored me or brushed me off. At that moment I felt a bit defeated because I didn't know what to do. They had a very negative attitude towards addressing problems that they’re facing. They'd either laugh when mental health was brought up or they would make excuses so that they wouldn't need to speak to me. After collectively feeling defeated and recognising a need to address the issue, my group worked through it and we managed to get a group of men together to discuss the issues related to addressing men in the community.
I think this is one of the major takeaways from my block. I cannot get into every detail of what was spoken about but I do want you to understand why men struggle with addressing the issues that they are facing. I've attached a study below that focuses on the understanding of mental health problems to South African black men. Although it specifically speaks about depression, it touches on a number of points that were brought about during our men’s group session. I suggest you give it a read to further understand the complex reasoning behind the beliefs of African men regarding mental health.
Some of the main takeaways is that stigma and the cultural concept of masculinity in the community is a prominent barrier that holds black men back from seeking help. The men in our group explained that society expects them to be strong and fearless providers so they feel as though they cannot express any problems because it is seen as a sign of weakness. The group that we ran really helped be gain a better understanding of the burden of cultural expectations on men in the community. It's one thing to read about these issues but actually hearing them from the men themselves creates a more in depth understanding. It helped me develop a way of communicating with them in a way that can build trust by explaining that I understand the pressure they feel so that they do not feel as though I will judge them or make them feel weak. This lesson is not just something to use in communities. I know I will keep the lessons learnt from the group with me throughout my career so that my practice is multi dimensional. It's also such a great lesson for me to give to the other students entering the community in the next block. My experience of feeling defeated and my new understanding of how to approach men is going to be passed on and will help not only the students but the men in the community.
4. Intersectionality
Woah, big words. Before I explain, here's a picture that will help you visualise it.

(McPhetridge, n.d)
Intersectionality is something I've been exposed to in the community. It's really overwhelming to come into the community and find all these issues and problems that need to be addressed. But, the concept of intersectionality helped me visualize the overlap of issues and how it impacts an individuals life. Intersectionality looks at the interconnectedness of issues of inequality. These overlapping circles that you see are all issues that an individual can face that has an effect on the way that they live. During my time in the community I have witnessed how different factors such as socioeconomic status shapes the experiences of an individual. To give an example, a mother who is living off a grant from the government struggles to feed her child resulting in the child being underweight. This affects the child's development and functioning and also impacts the mother as she may feel hopeless and guilty for not being able to adequately provide for her child. The child support grant also does not give the mother access to quality healthcare so she won't even realise that the child is underweight and will not know how to solve the issue. Do you see the interconnectedness of poverty, mental health, the physical health of the child? Additionally, if we look at poverty there's a number of interconnected factors that cause the mother to live in poverty such as the fractured system of South Africa post-Apartheid and high unemployment rates.
This concept also somewhat falls hand in hand with a new model that was introduced to me called the Mona Lisa model which looks at peeling away layers of injustices and inequality that hinder a person from functioning optimally to be able to find and reveal the real person behind all these issues and to help the client “unbecome”.
After learning about and understanding the above concepts, the concept of critical thinking became clearer to me. I found myself questioning everything I saw and asking myself why that's the case and how can I use my skills to overcome these issues. A quick example is my observation of children in the primary school using pencils the size of a safety pin. I immediately picked that up to be a major problem seeing as its a great barrier to the child's handwriting development. At the time I just saw it as a one dimensional problem and changed the childs pencil. But, after a while in the community my practice had begun to shift and I started to think about the impact that it may have on other children and asked myself what are the consequences and how can I change it. I used critical thinking to understand that the school is severely under resourced due to poverty and the broken South African system. I then also found out that the school relies on the children’s parents to buy them pencils and if they don’t they have to make do with the short pencils. It then made me think about the dysfunction in many families in the community either due to poverty, GBV, cultural stigma’s etc. and how it affects the parents of the children. Will every single parent of the primary school children be able to buy appropriate stationary for their children? Do they know the importance of handwriting development at the child’s young age? Most parents and individuals in the community have numerous other burdens and issues in their personal life that their top priority will not be buying pencils for their children. This is why I took matters into my own hands and decided that I have the means and resources available to me in my community-based practice and I decided to use my role of advocacy to raise funds and have stationary and pencils donated for the primary school children to be given out by the student OT's when deemed necessary. I'll update you on how that goes later.
My learnings vary from both professional and personal growth but I'd also like to touch on the growth of my relationship with my team members. There have been multiple times where we have all been low and are not having the best time or experience (it's normal to have bad days). But my group members really held me up while I felt like I could be drowning and this taught me about the need for interpersonal relationships with your colleagues. The above mentioned points are just some of the key takeaways from this block so far. I've grown both professionally and personally and I know I have even more to learn. I can't wait to take you on the next journey with me. but until then, go have a cup of tea and ponder over some of these learnings, you will learn more than you think. See you next time.

References
For women in South Africa, HIV stigma still runs strong. AVAC. (2014, December 19). https://avac.org/blog/for-women-in-south-africa-hiv-stigma-still-runs-strong/#:~:text=Today%20an%20estimated%2019%20percent,including%20physical%20violence%20and%20abuse.
Masemola, H. C., Moodley, S. V., & Shirinde, J. (2022, July 28). Perceptions and attitudes of black men in a rural district of South Africa towards depression and its treatment. South African family practice : official journal of the South African Academy of Family Practice/Primary Care. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9350529/
McPhetridge, M. (n.d.). Research guides: FYS 101: Intersectionality. Intersectionality - FYS 101 - Research Guides at Syracuse University Libraries. https://researchguides.library.syr.edu/fys101/intersectionality
0 notes
Text
How can I contribute to the Social Development Goals?
Hey guys, I hope everyone’s week has been going well. It’s currently a long weekend for me so I’m feeling spectacular. And I’m more than ready to get into this week’s discussion, I hope you are too.
s we know by now, I’m in my 4th year of studying Occupational Therapy and this year I have a new block where I work in a community for 7 weeks. This is to introduce me to the practical aspect of community-based practice. The community that I am placed in faces many challenges regarding the social determinants of health such as poverty, inequality, lack of access to healthcare, poor water and sanitation and poor-quality education. The South African report on SDG’s 2023, despite the attempts of alleviating these issues, high levels of poverty, inequality and unemployment still prevails in South Africa and the unequal distribution of financial resources as well as the lack of job opportunities for the youth remain a concern. My role as an Occupational Therapist working in the community is to consider the above report and determine how I can go about alleviating the burden of poverty and inequality in South African communities. In doing this, I need to focus on the Sustainable Developmental Goals (SDG’s). These goals are developed by the United Nations and aims to call for action in ending poverty and inequality (United Nations, n.d). Let’s get into some specific SDG’s and how I can work towards them in my community-based practice during this block.
So what are Sustainable Development Goals?
The SDG’s are a set of goals that aim to provide global aims for countries around the world to work towards. According to the World Health Organization, it aims to transform our world (WHO, n.d). These goals are very ambitious and address areas such as poverty, hunger, education, gender equality, and economic growth. Here’s a list of them below.

Image : United Nations. (n.d.). The 17 goals | sustainable development. United Nations. https://sdgs.un.org/goals
In my opinion, these goals are a great blueprint for countries to follow and use as a guide in order to develop strategies to alleviate the burdens and problems faced by those living in poverty. By doing this, countries are forced to address the underlying issues of poverty such as poor access to healthcare services, high unemployment rates, and hunger etc.
Why is it important for us to address these issues?
The article that I’ve attached below explains it quite well, I suggest you give it to read to help you understand poverty and inequality. It also explains the link between poverty and politics and although it is not a South African article, the content is still relevant to our context.
It claims that the poorest people have less influence over political decisions as opposed to the wealthier people (Hardoon, 2022). This creates a vicious cycle that reinforces the division in our South African society seeing as the wealthy make decisions to benefit them leaving individuals who live in poverty to bear the brunt of corruption. This worsens the burden of inequality and the underlying issues of poverty such as access to healthcare, education, and unemployment rates which is why we need to address these issues to give the majority of the South African population a higher chance of overall well-being and to improve their quality of life.
But, when looking at the South African government and the way our country runs, do we really think we will get anywhere near reaching these goals by 2030? I’m not being negative; I’m just trying to be realistic. I read an article by Professor John C Mubangizi about corruption in South Africa. I’ll link the article below. It’s called “Corruption in South Africa: The politics, the law and all the shenanigans in between” and I really suggest you give it a read. The title itself tells you it’ll be a good read, trust me.
He puts the issue of corruption in South Africa in a very good way when he says that the Constitutional dream that our country has is likely never to happen due to corruption. This is because corruption is affecting the basic human rights of the people in South Africa and makes it very difficult to implement strategies and deliver services that will improve healthcare, education, clean water, housing, and social security for the people of south Africa. Why does this matter? Because the Sustainable development goals also play on the constitutional dream that our country has. This means that in the same way our government cannot implement effective strategies to achieve the goals of our constitution that was made post-apartheid, how are they going to achieve these ambitious SDG’s?
It is because of the way of our government and the inability of our country to create positive change for its people living in poverty that we need to step up and work towards these goals ourselves. An article by Maher and Cometto explains the importance of community-based practice in meeting SDG’s.
The article states that community-based health workers are important partners in health care delivery and that we play a critical role in promoting an expansion of preventive, promotive and curative services related to reproductive, maternal, newborn and child health, infectious diseases and noncommunicable diseases (Maher & Cometto, 2016). Let’s get into which SDG’s I can contribute to and how I can do it.
I have to be honest, I’m writing this as though I’m a professional, but between you and me, there are so many theories and concepts to consider when implementing community-based practice that I overlooked the SDG’s. So far, I’ve learnt how to use my understanding of the social determinants of health and implement programs within the community to address these determinants. Now, I can use the SDG’s to evaluate the aims of my projects and see what else can be done to meet this goal to the best of my abilities. After gathering sources and wrapping my mind around the importance of the SDG’s in implementing effective projects and strategies, I’ve added a new way of thinking to my practice. And I hope that as I’m discovering these new methods, you guys also get inspired.

This goal aims to “end the epidemics if AIDS, tuberculosis, malaria, and other communicable diseases by 2030”. It also aims to achieve universal health coverage, and provide access to safe and effective medicines and vaccines for all.” (Joint SDG fund, n.d)
This is a goal that is very clear to me when I work in the community. I work in the community clinic throughout the week and the prominence of HIV/AIDS is extremely high. Just today over half of the women that was screened were HIV positive and all of them have children who are susceptible to the disease as well. My role in this SDG is health promotion. Health promotion is a process that includes advocating for, educating or modifying lifestyles or environments of individuals in order to prevent disease, injury, or poor health choices so that we can enable individuals’ engagement in their occupations and promote their overall health and well-being.
Every day, my group members and I carry out health promotion speeches where we educate the patients at the clinic on the role of Occupational Therapy and speak to individual clients about the effects of HIV/AIDS and importance of medication compliance and health management. This goal also gives me ways of thinking about new strategies to implement that will create a greater impact on reaching good health and well-being for the members of the community such as giving health promotion talks about HIV/AIDS and making posters or pamphlets to hand out to the clients about how to practice safe sex and how to manage their health once diagnosed with HIV.
I can’t lie though, the thought of having to speak in public really scares me. Especially since I don’t speak isiZulu. I feel as though no one cares about what I’m saying and that they’re all judging me. But I recently joined a seminar about language and dialogue that opened my eyes to the possible reason for this. It brought up so many things to think about but one main thing I took away from it was the fact that there is always a dominant language of knowledge and the other languages are always silenced. In our South African context, English is the dominant language and isiZulu is often silenced in mainstream society as those that speak isiZulu need to learn English in order to thrive. I think that this is the reason I’m overlooked when I speak in English in an isiZulu dominant community. Because they are able to freely converse in their dominant language and I disrupt that freedom. Just my thoughts for you guys to ponder over.

Let’s quickly move on to the next few SDG’s that I work towards. SDG 4 is aiming for quality education and there are a few targets that I contribute to when I work with the children in the day care, creche, and primary school. Some of the targets aims for “equal access to quality pre-primary education” and for “universal literacy and numeracy”(The Global goals, 2024). I contribute to this goal because I use my knowledge of play with paediatrics and incorporate it into fun activities, songs and sessions that teach the children basic learning skills like their numbers, alphabets, shapes, and colours. For example, I used a DIY board with different colour shapes and made them take turns to hit the one that was called out. This builds the foundation of learning that all children need in order to succeed in their academic education. I also use my OT skills in the primary school and run group sessions with the grade 1’s, 2’s, and 3’s that are either behind in their academic learning or are struggling with grasping foundation educational skills like handwriting, spelling and comprehension. This SDG does not only focus on kids though. It also focuses on improving literacy and numeracy within the adult population and my group also has a project in progress that aims to provide classes for adults, who did not receive adequate quality education, who are looking to learn how to read and write. This gives them more opportunities for employment and alleviates their burden of poverty.

This SDG targets women in all spheres of life. It looks at ending discrimination against women, ending all forms of violence against women, and to give women equal rights to economic resources. Patriarchy is a big concept that affects women in all aspects of their lives. An article by Cody Peluso explains that patriarchy perpetuates gender inequality which leads to disparities in employment opportunities, education and earning and income leaving women to bear the brunt of poverty (Peluso, 2023). I’ve attached the link below because the concept of patriarchy is so detailed and complex and I don’t have the space to discuss it today. But give the article a read and maybe next week we can get into it.
In my practice within the community, I work with both men and women equally. There are some aspects where women need more attention. For example, maternal and child health. But within this intervention I don’t just focus on the mother taking care of the child. I focus on the mothers mental health, her employment status and her relationship with the father of her baby or her boyfriend or husband. I try and determine if there are any cases of GBV going on at home so that my intervention can include helping the women out of that situation. I also provide the same learning opportunities for both men and women as all the projects that are run within the community are open to men and women, meaning that women are equally able to upskill and find employment and earn and income as men.

I think we all know by now that I can go on with discussions forever. But let’s wrap this up and combine the last two SDG’s because in my opinion they work hand in had. As a matter of fact, all of the SDG’s that I’ve mentioned are connected to each other. But that’s a discussion for another day. Both SDG 8 and 10 target economic growth within our country and I have a number of projects and interventions running within my community that aim to address unemployment issues and inequality regarding employment. SDG 8 targets youth employment, education and training and full employment and decent work with equal pay. SDG 10 also focuses on economic growth and unemployment by targeting the promotion of universal social, economic and political inclusion and ensuring equal opportunities and ending discrimination.
How do I do this ? Let me list and explain the projects and interventions that are in progress or currently running within the community that I am working in.
Job skills and work readiness project
This project aims to provide adults who are struggling with finding jobs with skills and abilities that will increase their opportunities of finding employment which will work towards creating equal opportunities. Some of the skills within the group sessions are how to write a resume, interview skills, roleplaying interactions with the employer, sequencing and processing tasks to develop industry working skills, and advertising skills to showcase their abilities to potential employers.
Adult learning classes (still in the works and needs to get picked up off the ground)
This aims to provide basic academic learning to adults such as reading and writing to advance their skills and abilities and equalize their opportunities for employment in the private or public sector.
Youth study skills
This is a group that we run for older children who are struggling with their academics. This works towards SDG 8 as we are assisting in improving the education of the youth and preventing them from being left behind in society. This group also increases the chances of youth succeeding in their academics and integrating into the economic society to find employment or furthering their studies.
Vocational rehabilitation for people with disabilities
This falls under my every day practice as an OT. Vocational rehabilitation and providing interventions for people with disabilities targets goals within SDG 8 and 10. This is because I aim to improve specific body functions to enable them to function in their daily occupations and I also work on adapting their skills and abilities to allow them the same employment opportunities as those without disabilities. If we take one of my clients with right sided weakness for example, I aim to improve her muscle strength to allow her to function in her ADL’s and my second aim of my intervention is to train her to be able to still carry out her job with little to no difficulty. And if that is not possible, I am to equip her with the right skills to be able to work in a different job.
To wrap things up, I want us to ponder over the effect that corruption has on our communities within South Africa and what that means for our role as Occupational Therapists. Our country faces so many challenges in implementing strategies to try and meet these SDG’s which leaves the responsibility into our hands as community-based health workers to alleviate the issues of the social determinants of health and aim to achieve the SDG’s. We can also use the SDG’s to evaluate the outcomes of our projects and see if we are moving towards the SDG’s. I know this week’s discussion was a long one but I really encourage you to engage with the topics and the links and find ways that you can contribute to them. I’ve attached a link below that you can use to find ideas on how we can work towards the SDG’s. Let’s be the change that we wish our government could implement.
References
Goal 3: Good health and well-being. Goal 3: Good health and well-being | Joint SDG Fund. (n.d.). https://jointsdgfund.org/sustainable-development-goals/goal-3-good-health-and-well-being#:~:text=SDG%203%20aspires%20to%20ensure,medicines%20and%20vaccines%20for%20all
Goal 4: Quality Education. The Global Goals. (2024, January 23). https://www.globalgoals.org/goals/4-quality-education/
Hardoon, D. (2022, February 21). Inequality, measuring it and why it matters for poverty reduction. Development Initiatives. https://devinit.org/resources/inequality-measuring-poverty-reduction/#:~:text=Economic%20inequality%20is%20closely%20linked,making%20than%20the%20wealthiest%20people.
Maher, D., & Cometto, G. (2016). Research on community-based health workers is needed to achieve the Sustainable Development Goals. Bulletin of the World Health Organization, 94(11), 786–786. https://doi.org/10.2471/blt.16.185918
Mubangizi, J. C. (2020). Corruption in SA: The politics, the law and all the shenanigans in between. City Press. https://www.news24.com/citypress/voices/corruption-in-sa-the-politics-the-law-and-all-the-shenanigans-in-between-20201007
Peluso, C. (2023, November 8). The origins of Patriarchy. Population Media Center. https://www.populationmedia.org/the-latest/unmasking-the-patriarchy-its-origins-impact-and-the-path-to-equality#:~:text=The%20Impact%20of%20Patriarchy&text=Gender%20Inequality%3A%20Patriarchy%20perpetuates%20gender,are%20disproportionately%20occupied%20by%20me
United Nations. (n.d.). The 17 goals | sustainable development. United Nations. https://sdgs.un.org/goals
World Health Organization. (n.d.). Sustainable development goals. World Health Organization. https://www.who.int/europe/about-us/our-work/sustainable-development-goals#:~:text=The%20Sustainable%20Development%20Goals%20(SDGs,no%20one%20is%20left%20behind
0 notes
Text
How prepared are we to work in South African communities?
Hey guys, I’m back again. Last week I mentioned that community block was a rollercoaster of emotions. This week I want to get into why that was the case. Personally, I feel as though I was not prepared for the multidimensional approach to assessing and treating individuals within a poverty-stricken community in South Africa. And in an article to follow, you will see that other past OT students can also agree with my opinion. Let’s get into why I say this by taking a look at the OT curriculum and analysing whether or not it prepares us well enough to work at a community level.
I personally feel as though no one can ever be prepared enough to work at a community level. I certainly was not prepared. That is not to say that the OT curriculum didn’t teach me anything. I just think that hospital-based practice and community-based practice are two very, VERY different contexts that we as Occupational Therapists treat. And I feel as though the majority of the OT curriculum focuses on hospital-based practice instead of the multi-dimensional approach to clients in South African communities. It also does not place as much focus on adaptations of intervention according to the South African economic challenges of poverty, and the inability to meet basic needs such as food, housing, and healthcare. This is why I feel as if I was thrown into the deep end when I started my community block this year.
This is all my personal opinion though; I’d love to know what you think. Let’s get everyone’s opinions down below and we can discuss further in the comments.
I read a very interesting article about Preparing occupational therapy students for practice in rural areas. Although it didn’t specifically mention the OT curriculum, it did mention a very wild statistic that I think will give us some perspective on community based practice. It claims that the occupational therapy profession is maldistributed with more therapists moving into urban workplaces rather than working in rural areas (Hayes et al., 2024). It also stated that occupational therapists are very rarely found within marginalized rural populations, and yet, a core aim of Occupational Therapy is to work with people who are marginalized to help them engage in meaningful daily activities. I’ve attached the link to this article below because there’s a few things I want to address from it, give it a read if you have some time.
Let’s talk about what I’ve mentioned above. Isn’t it baffling?
Our South African context brings about so many people within the population that are marginalized and yet majority of therapists drift towards helping those that do actually have the means of obtaining quality rehabilitation. The community that I am currently placed in has so many areas that need Occupational Therapist’s intervention, and yet, once students leave, the community no longer has that support. It’s a very sad reality that needs to be addressed and there’s no other profession that’s better to address it than us. Why is this? Because our jobs are so multidimensional. We don’t just work with muscles and ligaments (my sincerest apologies to my physio buddies…); we work with the person as a whole. Our OT curriculum does look at the Social Determinants of Health and we are well aware of the issues that many disadvantaged South Africans face due to the looming shadow of Apartheid and the corruption within our South African government. This is why we look at their home environment, their support systems, the resources that are available to them, their mental health, their HIV status, or their employment status. We can intervene in every single aspect of an individual and we have so much to offer. Yet our incredible work is not being used in the place where it is most needed.
This brings me to another very interesting point that I’d like to take from this article because it gives a possible reason as to why OT’s move away from rural settings. It claims that there is a hidden agenda within the OT curriculum that glamorizes urban care and shows rural practice as less prestigious. This is why OT’s are turning away from working in communities. Don’t you agree with this? I mean let’s think about it, throughout my learning journey in OT, I’ve watched videos of cool therapy sessions where the client is participating in an ADL of cooking in a clean and organized kitchen. Or we’re taught about the fun paediatric play activities and sensory play with coloured rice and toys buried inside. I know you know exactly what I’m talking about, don’t play innocent.
*Trigger warning for my fellow community based OT’s*

(Barnes, 2023)
Yeah, I caught you red handed. Think about this in a community context. Are we really going to give children who sometimes don’t have adequate food to eat a box of dyed rice to use in sensory play? It’s a bit tone deaf isn’t it?
This brings me to the point being that we aren’t exposed to the reality that many South African’s are living in such as the kitchens in the informal homes within communities or the lack of basic toys for the children.
I think the paediatric aspect of community-based practice is what really slapped me in the face.It was a big reality check for me but also a major area of professional growth as an Occupational Therapist. For two weeks prior to my community block, I was learning all about paediatrics. I was in awe of all the cute and creative toys and games I could play with children in my intervention sessions. And then I start my community block and the first mother I speak to tells me she doesn’t have any toys at home that make a sound, like a rattle. This is what I mean when I say that I was not prepared for community-based practice. Yes, I know the importance of play for children and babies. But I needed to throw the idea that I had of paediatric care out of my head and re-learn a whole different approach so that I could be contextually appropriate in my interventions. I couldn’t just be like ‘oh you should go buy a rattle from Toys R Us’. And yes, it’s not to say that I didn’t realize that less fortunate homes do not have baby toys, it is something we are taught about in class when we talk about the Social Determinants of Health for example. But listening to a lecture about it and actually being in a situation that addresses it directly are two very different things.
An article that includes personal responses from past OT students on their ability to cope with Primary Health Care and rural practice is a great way to substantiate my point above. Have a look at the findings of this study and let me know what you think.
One of the common responses found from the study was that the participants reported that they found it challenging to practice within the realities of a rural setting because of the resource constraints and because the undergraduate programme and clinical skills development had mainly occurred in well-equipped tertiary hospitals (Naidoo et al., 2017). So if we had a client come into the hospital, we were able to use the hospitals vast range of equipment like the splinting station for flexor tendon injuries, or the standing frames for paediatrics or hand function boards for vocational rehabilitation. Whereas, in a community setting, we need to come up with ways to make these resources like finding recyclables and making a hand function board out of bottle caps and bottles.
Although I do have a lot to say about the OT curriculum not preparing us enough for community-based practice, technically, I am still studying in my fourth year. Which means that my community block is part of the curriculum. In this case, I would say that it is preparing me for community-based practice. But because of the sudden switch from always focusing on hospital-based practice to community-based practice in fourth year, I think a number of students will be thrown off resulting in more students moving away from rural practice. In my opinion, if we prepare OT students more prior to working in a community setting, we will be able to ease into the community-based practice without feeling like a deer in headlights. That way, less OT’s will run away in fear of the community but will rather embrace the multidimensional approach to the clients and community at large. I know that some of the reason as to why I was not completely terrified when I began my block is because I had some experience within the community for last year. So I hope that continues and I actually hope the introduction to communities gets pushed further to the first and second years. That way they are more accustomed to the way of thinking within the community context and can provide quality care and intervention that is contextually appropriate to the individuals within the community.
That's all from me today folks, I look forward to seeing you back here again next week.
References
Barnes, P. (2023, August 26). 30 sensory activities: For Kid’s Brain Development. Mom Loves Best. https://momlovesbest.com/sensory-activities-kids
Hayes, K., Dos Santos, V., Boyd, N., Connelly, B., & Lustig, K. (2024). Preparing occupational therapy students for practice in rural areas: A scoping review protocol. BMJ Open, 14(2). https://doi.org/10.1136/bmjopen-2023-075886
Naidoo, D., Van Wyk, J., & Waggie, F. (2017). Occupational therapy graduates’ reflections on their ability to cope with primary healthcare and rural practice during Community Service. South African Journal of Occupational Therapy, 47(3). https://doi.org/10.17159/2310-3833/2017/v47n3a7
0 notes
Text
Well hello there everyone, long time no see …
I’m back and I hope you’re ready because we’re about to catch the flight of a lifetime.
I’m currently in my final year of studying Occupational Therapy (I know right, I still can’t process it). This year entails a number of new experiences and I can’t wait to share it all with you.
This week I want to start off with something that I think is one of the most important things to talk about seeing as I’m in a block that deals with it directly. The health of mothers and children, specifically looking at mothers and children living in communities like the one I’m working in.
My first block this year is community block. And, let me tell you, WOAH. It is a big change and a lot of work and many things to wrap my head around. I cant lie, I’ve had around 4 crying sessions so far, but we all know that’s how I cope. Cry and get back to work. It’s a good tactic in my opinion.
Back to my point, maternal and child health within the community.
I read an interesting article when thinking about how to go about this discussion that I think would be a great way to understand a mother so that we can also then understand how it affects our work as OT’s. I’ll add the link below so that you can also take a look at it.
The main thing I wanted to take from the article was that a mother is seen in different ways at different levels (Common Good, 2022).
A mother as an individual has personal experiences, struggles and problems that plays a part in how they function in their day to day lives. This can speak to their identity, their self-esteem and their overall mental health. This is so important to understand because let’s take us for example, when we’re upset or we’re sad or if we aren’t feeling good in our own skin, we sometimes don’t feel like doing anything or we don’t feel like leaving our rooms. Let me know if I’m right or if I’m talking rubbish.
I hope that what I said makes sense. But now let’s think about mothers, imagine feeling all of what was said above and not wanting to do anything, but you have a whole human being to take care of that needs your support. I’m hoping that my point is starting to take shape in your minds at this point. When looking at a mother as an individual we have to consider how their personal health and mental health can be affecting the care and development of their child. A mothers poor personal and mental health in turn has a negative effect on the child’s overall health. This is one of the reasons at to why maternal health is so important, especially to Occupational Therapists. We need to focus on mothers and intervene in any way we can in order to prevent a domino effect of further issues developing as time goes on.

(Waters, 2022)
(PSA: this is not what a mum and child’s environment looks like in a South African community setting!!)
Before we move on to the other 2 levels of a mother, I do want to touch on something I’ve learnt this week that links to our role as Occupational Therapist’s. It’s so easy for us to get sucked in to stories from our clients and to feel an overwhelming sense of sympathy and need to help in any way we can. I think I can sometimes get a bit carried away in this aspect. I’ll be completely honest here and tell you that I forget my role as an OT and feel this need to just give them whatever they need to help them in that moment.
BIG MISTAKE.
From all the lessons I’ve learnt this week (which was a lot, might I add), I think the one thing that sticks out to me is that, yes, we do need to find out personal information about our clients and, yes, we do need to dig deeper and see the hidden meanings. But in a community context, when we’re trying to provide a service to so many people in need of it, acting like a counselor is not what is going to fix things. Listening to a mothers story about the trauma she’s been through and letting her cry for 20 minutes in our session is not going to change anything. What is going to make a difference is asking the tough questions, finding the root cause of the problems and developing solutions that is surely to show change.
However, I read an article that expresses a thought that somewhat contradicts what I’ve just said. The link is attached below for those of you that want to expand your knowledge.
Let’s get into it. Ann A. Wilcock wrote an article about occupational science and within it she explains that transformation is the path to well-being, especially because it doesn’t focus on the “mundane” aspects of a persons life but rather on their dreams of aspirations (Wilcock, 2005).
This is a safe space, so I’m going to outright say that I do not agree with what she’s said. That’s because when we look at our South African community, so many mothers and families are suffering from a number of problems. Poverty, gender based violence, HIV/AIDS and the list goes on. In my opinion, our role as Occupational Therapists is to improve their lives in any way we can, even if that means focusing on the simple every day needs and problems faced by the mother, not to “transform” their lives and help them achieve their biggest hopes and dreams. I feel like that concept is somewhat unrealistic. Let me know your thoughts in the comments, I’d love to hear if you disagree, let’s argue…
I think it’s time I move on to the other 2 levels of a mother and try to wrap this up.
Let’s talk about the last two levels together because I think they somewhat link. Level 2 is the mother within the household and level 3 is the mother within the community.
What does the home look like? Is the father present? Does the father treat the mother and child right? Is the mother exposed to HIV/AIDS? Does the mother have the resources available for her to raise her child? Is there an income that the mother is living off? Is she working? Where does she leave her child? Is she able to access a doctor when the child gets sick? Can she get HIV/AIDS medication in her community? Is there a stigma of HIV within the community? Is there violence in the community? Is she safe in her home?

(Stats SA, 2014/15)
As of 2014/2015, 49.2% of South African’s have been living in poverty (Stats SA, 2014/15), and it’s most likely increased from then. This statistic is so clearly prominent in the community that I’m based in.
Out of all the mothers and children that I have seen this week, I can tell you that more than half of them are HIV positive, majority are single mothers, gender based violence is an underlying factor that mothers are trying to hide, they are struggling with generating an income and some are living off government grants and the community that they live in often threatens their safety.
The same goes for children in our South African communities. There’s another blog post from the Sikunye blog I’ve linked above that briefly explains the tragic reality of our children in South Africa, I think it’s a great quick read to understand just how many issues our communities face. It highlights that poverty, malnutrition, infectious diseases (HIV), stress, violence, psychosocial risks and disrupted caregiving are all risks to a child’s development (Common Good, 2024).
These are all factors that we as Occupational Therapists need to consider as each factor impacts the well-being of both the mother and the child. And we as Occupational Therapists have an important role to play in using the community based approach to improve the mother and child’s well-being.
To end off, I want to reiterate that we cannot be superhero’s and help everyone achieve their biggest hopes and dreams. But what we can do is use our knowledge, use our theories and our experiential learning and growth to find the root cause of the problems we see and change the seed that is grown, the soil it’s planted in and the water that’s used to grow it (my sincere apologies, I just laughed at myself for being that cringe). But the analogy makes sense, our role as OT’s is to be client centered and to have a community based approach which means we need to focus on the mother and child, their environment and the macro factors that impact their development and growth.
That’s all for today folks. Please let me know your thoughts on the comments, let’s interact and learn together. I’ll be back soon with more stories and OT life lessons, I hope to see you back here again.
References
Five Facts About Poverty in South Africa. Statssa.gov.za. (2015). https://www.statssa.gov.za/?p=12075
Good, C. (2022, April 20). What is it like being a mother in South Africa?. Sikunye. https://sikunye.org.za/blog/what-is-it-like-being-a-mother-in-south-africa/
Good, C. (2024, January 21). The big why behind the sikunye model. Sikunye. https://sikunye.org.za/blog/the-big-why-behind-the-sikunye-model/
Waters, D. (2022, April 26). What is postnatal depression and what treatment is available?. GoodTo. https://www.goodto.com/family/postnatal-depression-115582
Wilcock, A. A. (2005). Occupational science: Bridging occupation and health. Canadian Journal of Occupational Therapy, 72(1), 5–12. https://doi.org/10.1177/000841740507200105
0 notes
Text
Hi guys, how’s everyone doing ?
It’s getting to that time of year where everything starts feeling like it’s going too fast and we’re all just aching for a second of work free, stress free peace. If you’re feeling like this right now, you aren’t alone, I’m right with you. Let’s get into todays blog though and see if we can all feel a little lighter. Use this as your few minutes of freedom before you need to get back to reality.
This weeks blog is going to be quite a personal one. We’re going to be talking about a problem that every single person faces all over the world. Mental health. But specifically, mental health problems faced by the youth due to academic stress. And yes, I will be speaking from personal experience because I am not that old guys I’m still part of the youth of South Africa even though I have the back problems of a 72 year old 🥲 I know there’s a huge number of factors that have an effect on mental health of the youth but I want to talk about this specific topic because I can give you first hand personal experience that can put this topic into perspective and help you understand it better.
Our youth in South Africa represent the future. We have a history of so much pain and suffering and our youth are here as the future generation to help solve some of this suffering be a shining light for us to lead us to a better South Africa. But, this light of the youth can easily dim. This is due to the number of mental health issues that our youth face which impact their well being and create a shadow over their light. In todays blog, we’re unpacking how mental health issues arise due to academic stress and how it affects the productivity and functioning of the youth of today.
The weight that academic pressure has on the youth in South Africa is intense. We’re all caught in a whirlwind of academic expectations and face the pressure of succeeding in a competitive education system which takes an incredibly tough toll on our mental health leading to a number of issues such as anxiety, depression and burnout.
Burnout. Please picture me standing on a chair and screaming this.

I feel this is the only way to get you guys to understand my passion behind this word. Burnout. I am burnt out. This is going to get a bit personal but I really hope sharing my experience with you will make you feel less alone. I really want this to be more of a personal rant so I’m attaching a link below for you guys to read up about academic burnout. It’s a lovely article that’s doesn’t use a whole lot of fancy words so it’s easy to read and you can give your brain a bit of a break.
As I mentioned in the beginning, it’s coming to that time of the year when everything is starting to feel like it’s too much to handle. Stress levels are off the radar and the work is just piling up and I can confidently say that I am reaching the brim of my sanity. This feeling is not something I want everyone to relate to but I know that a lot of you reading this will because it’s the reality of academics. And I hate this feeling because i can see and feel it affecting my work ethic. As we all know I’m working at an old age home for my psych placement this semester. And it is crucial to always keep your mood up and happy when dealing with the elderly in an old age home because majority of them experience symptoms of institutionalization meaning they have depressive symptoms, low mood, a monotonous routine etc. Here’s a quick read if you aren’t completely aware of what institutionalization is.
Us, being the occupational therapists need to use fun and meaningful activities to stimulate them and keep them active and elevate their mood. But it is so difficult to do all that when you personally feel drained. I do think that I have mastered the skill of covering up my personal emotions when it comes to dealing with my clients and I can put on a good face and carry out my treatments effectively. But once that session is over I feel the weight of campus crashing back down on me. A good example of this is actually over the past week. I’d say I am usually in a decent mood when I get to work in the morning, I’m making conversation, greeting everyone and starting off my day with getting my life in order. But looking back at this past week, I went to work extremely tired and not in the best of moods just ready to get the day over and done with. And that is not how I like to work. In fact, the activity I had planned for this week needed me to be energetic and active and in a positive mood but to be completely honest I was dreading having to do all of that when the only thing that was on my mind was the long list of deadlines, due dates and exam dates in my head that kept replaying over and over.

That is a visual representation of me this week. Thankfully I’ve mastered adapting my mood to the situation and the session was a success but I don’t think it’s fair that us students have to go through this in order to succeed and see good results.
South Africa needs the younger generation to bring new and innovative ideas and perspectives to the table. We need to drive the progress in a number of different sectors in this country such as the business, health care and technology sectors. We are the new generation that are going to contribute to the economic growth of the country by finishing our education, graduating and getting employed and increasing productivity. We have the energy and passion to advocate for a number of positive social changes in society such as equal rights and social justice. We are the generation that will carry our rich heritage and cultural traditions to the next generations. In essence, the youth of South Africa are the backbone on our nations future.

But how are we meant to find the motivation to do all of this when our brains feel like they’re going to explode just trying to reach the first goal of graduating. Of course we need to invest in the education of our youth and work on pricing equal opportunities to all in order to establish a foundation of strong and independent youth. But the moral of this whole story is that we also need to invest in the mental health of our students. Yes there are certain things that need to be done by a certain date in order to reach the next level of education. But why don’t we try and work on our organization skills so that they don’t have to worry about the stress and panic of logistic issues that may prevent them from getting to campus on time. Why don’t we invest more time and money in providing easily accessible mental health resources to students that are struggling to keep up with the work load. Why won’t we invest time and money on working on developing a more inclusive education system that focuses on the mental and emotional needs of the students.
I know that academics have always been this pool of pressure and stress and everyone always just brushes it off, sucks it up and says that this is the norm. But I seriously think we need to start thinking of a new approach to this. I’m not saying the work needs to change, I’m saying we need to try and change the system to adapt and better deal with the mental and emotional capacity of the students. Because there’s no point in having millions of students studying to finish a degree and get a job but they end up hating their degree and job by the end of it and don’t pursue a career because of the mental trauma it’s caused them. That is how we lose the youth of South Africa and that is how we destroy the hope for a positive future.
That’s my rant for today guys, I hope this give us all something to think about. And I hope my experience of burn out shows you that you’re not alone. It’s ok to feel like this. But it’s not ok to always feel like this. If you’ve been feeling this way for a long period of time now and you feel like there’s no end in sight, I highly recommend you try and reach out to your support system. Whether it be your family, friends or a therapist. Let it all out and show your emotions. Don’t hold it all in because I guarantee you it will come out at some point and it’s not going to be pretty. Let it out in a healthy way now and let’s work on moving forward and getting our lives in order. I’m here if you need anything.
Thank you for being here and for listening to my stories. I really appreciate you. And I Joel I see you again next time and that we’re all healed and full of life an energy. Keep well.
Aisha
0 notes
Text
Hey guys, Aisha here, back with another twist on this weeks blog. Look at me being all creative 🤌🏼
So I watched a movie over this so called “vacation” we had from campus, and it’s called ‘Love and Other Drugs’ with the main characters being the never aging Goddess Anne Hathaway and *trigger warning* Jake Gyllenhaal. Yes, I’m sorry my fellow Swifties but this week’s blog is gonna be talking about our least favorite ex of Taylor’s so I suggest everyone hold onto their scarves and sit tight because this is going to be an emotional rollercoaster…
Ok so, let me start by giving you guys a quick explanation of what the movie’s all about. Anne Hathaway plays the main female character named Maggie and Jake Gyllenhaal plays the main male character named Jamie. There’s a few subplots that you follow throughout the movie like the whole pharmaceutical industry plot line and of course the romance between Maggie and Jamie but the main subplot I’d like to touch on is about Parkinson’s disease. Throughout the entire movie, Maggie is struggling to cope with the recent diagnosis of Parkinson’s disease and it looks at how the diagnosis is starting to affect her mentally, physically and emotionally. Now I don’t want to sound like one of those movie review websites that explains the entire movie from start to finish so here’s a link that’ll tell you everything about the movie if you don’t want to watch it. If you do want to watch it I suggest you save this blog, watch the movie and then come back because there might be some spoilers lower down. Ooh and, before I forget, this is not a movie for kid’s due to some very … adult scenes … so please make sure your kids are playing with Lego’s or something, I don’t know, just keep them away from the tv please 🙏🏼
Back to the whole Parkinson’s story. Gosh, some scenes in this movie wrecked me. Anne Hathaway portrayed the role of Maggie with Parkinson’s so well it pulled at your heart strings whenever she was struggling. Now I know we’ve probably all heard of Parkinson’s disease but I’m sure some of us are just like oh that’s the disease with the shaky hands and think that’s it. Well my friends, yes it does include tremors and shaky hands but there are so many more symptoms and complications of Parkinson’s that are cognitive, emotional and behavioral along with physical. You can click the link below to have a quick read about it.
I think one of the reasons as to why I was so drawn to this movie is because of the fact that not even 4 days ago I was given a new client in the old age home I’m placed in who is diagnosed with Parkinson’s disease. And I could relate the movie back to the client but it gave me a much deeper insight and understanding into the emotional aspect of the diagnosis. I know Maggie and my client aren’t the same age but there was also a time when my client was going through what she was going through and my heart breaks to think about how the diagnosis must have affected my client. It also gave me so many questions that I’d like my client to answer that will help me understand him and his emotions better which will also help me facilitate and plan his intervention sessions well.
My client is so cool guys, he walks around with his walker and a little speaker playing music wearing his hat and sunglasses. I love it. But after watching this movie I can’t help but think about what’s deeper beneath the surface behind his sunglasses, behind his playfulness and socializing personality. There is so much I need to understand to help me move further in my intervention.
Throughout the beginning of the movie we see Maggie starting to slowly struggle with her symptoms. There is this specific scene where Jamie leaves Maggie’s apartment after being shot down after his confession of love and Maggie tries to pick up her glass of water but her muscle weakness and the tremors in her hand cause her to drop the glass and she just crumbles to the floor and breaks down sobbing and Jamie rushes back in to hold and comfort her. Wow guys. I think I finished one whole box of tissues after that scene. I know we all like to watch movies to switch off from reality but this entire movie just kept bringing me back to my placement and my client. Seeing how vulnerable Maggie was in that moment made me think about how my client may have had these moments in the past. He told me that it was his choice to come and live in the old age home but after watching this movie there are so many things I need to figure out behind his emotions and journey through his disease.

We can even look at how Maggie consistently tried and tried to push away any possibility of a relationship with Jamie and understand the emotional and psychological struggle of always feeling like a burden when you’re diagnosed with Parkinson’s disease. My client told me that it was his decision to move into the old age home but he didn’t go into any further detail. This got me thinking though, was it because he felt like he didn’t want to be a burden to his children ? His children live outside of Durban and they rarely visit him so there could also be a possibility that his children couldn’t or even didn’t want to take care of him. There are so many battles one has to face with Parkinson’s and I’m learning now that I need to dig so much deeper into my clients emotions to develop that foundation of empathy and trust between us.
We can also see in the movie that even after Maggie and Jamie get together, Maggie’s anxiety, depressive symptoms and her fear of being dependent on someone else places such a heavy strain on their relationship that it eventually breaks off. My client told me he was divorced from his wife but he didn’t mention anything more and in the moment I didn’t think to ask him further questions because the thought didn’t occur to me that his diagnosis may have played a role in it. Gosh, I don’t think you guys understand how stupid I felt after watching that movie. Not because of how little I knew about Parkinson’s but because I was so oblivious to just how much of an emotional toll it can take on someone.
Maggie also faces a lot of problems with her medication. I’m not going to bore you with the many medications available for Parkinson’s but I will mention that each and every single one of them have side effects. I’ll link a website below where you can read up on some of the medications and the side effects are there as well because there are way too many to list. It’s just another aspect of the movie that makes you understand the amount of struggles someone with Parkinson’s has to go through. I mean how many have I listen already ? Physical symtoms, emotional and psychological effects, anxiety, depression etc. the list goes on. And now we add their medication on top of everything. Taking medication should be helping relieve your symptoms yet in order to do that there still needs to be suffering with other factors like nausea, dyskinesia and hallucination.
💡Ooh this actually reminded me about a precaution I need to take when I see my client. I need to check up on his meds and any side effects he’s facing. Noted.
Then there’s the scene where Maggie goes to a sort of group session with many people that are diagnosed with Parkinson’s. Different people take turns to come up and diss the struggles they’re facing with Parkinson’s like buttoning up a shirt, brushing their teeth, drinking soup and tying their shoelaces etc. And then there’s also moments where some people come up and explain that being diagnosed with Parkinson’s is a daily struggle of trying to maintain a sense of dignity and grace in society. Oof. Tears. Tissues. Runny nose. All the works. It also panned to Maggie’s face every once in a while and showed her crying when she realized the pain and struggle that everyone goes through and also that she’s not alone. 💡 Maybe I need to work on something like that for my client. If there are a few residents that are diagnosed with Parkinson’s, the home can create a Parkinson’s group that runs once a week where everyone can come together to cry and laugh about their struggles which will also lift the burden of social isolation.
In the movie Maggie says "I can't sit around and wait for this to consume me. I can't let it rob me of the person I was meant to be” and I think this gives me such great motivation behind my planning for different intervention sessions for my client. Yes, I know he’s much older but that doesn’t mean he can’t live his life to the fullest and be the person he’s always wanted to be. Parkinson’s is like a disease that is always trying to eat away at someone’s cognitive, psychological, emotional and physical functioning but I know for a fact that I, as an Occupational Therapist can resist that toll through using meaningful activities that keep my client true to himself and that could maybe even reminisce to his younger days and make him feel more in control of his life.
I cannot explain to you how eye opening this movie was guys, I mean yes the love story was amazing as well and the acting was 10/10 but the number of connections I was making throughout the movie to my experience at the old age home with my client was insane. You’d just hear little gasps every time something clicked in my head and I was left contemplating my entire OT role. I hope you guys enjoyed the movie as much as I did and I’m sorry if you haven’t watched the movie and I gave you some spoilers. But I promise you, nothing I have said does the movie justice, give it a watch and come back to re read this you’ll see what I’m saying.
I hope this weeks blog was a good one. I certainly enjoyed it. And don’t stress guys, this isn’t turning into a movie review blog, I don’t think I’ll have any time after this week to even touch the tv remote 🥲 But I’ll be back next week with another theme and another long rant about who knows what. See ya there 🫶🏼
0 notes
Text
Well hello there again. Funny seeing you here.
I’ve been thinking I wanted to change things up a bit around here so today’s theme is going to be all about magic. Weird. I know. But trust me it’s a good one I promise.
I suggest everyone buckle up because today we’re delving into the realm of the therapeutic use of self.
Now I sat and started to think about how I could explain this in an easy way because I’m a little tired of definitions. Not to say they’re no good, I’ll link a website below for you guys to check out if you’d like a more clear explanation. But I’m gonna go further into it in my own way.
Cue the cringe.
Occupational therapists are the superheroes of well being. And our superpower is all about us. Hence, therapeutic use of self. It’s our secret weapon to make a real difference in our clients lives. In my case I use it to help my elderly clients in the old age home I’m placed at.
Let’s do it like this. I’m going to list a whole lot of superpowers that we as occupational therapists have in order to ensure “therapeutic use of self” with all clients. And for those of you who still don’t understand, don’t fear, Aisha’s here (the cringe gave me a shiver up my spine 😭) What I meant to say is that I have a million and one examples of how I use each of these superpowers in my therapy to make the most of myself as the therapist with my clients.
💥 Superpower number #1 : Building trust and a connection between us and our clients.
When our clients see that’s we’re on their side and that we’re only here to help they’re more ready to reveal their challenges and we create a safe haven where their voices are heard. According to a site I was looking through when I was struggling with this a few days ago, some ways of building trust is through remaining calm, being patient, avoid behavior that will humiliate the client and throwing your ego out the door. There’s a whole lot of ways to build trust and rapport with your clients and I’ll link it below for you to read.
Guys, I cannot explain how important this is. Especially in my case. Elderly people are sometimes paranoid when others come into their residence especially since it disrupts their routine and what they’re used to. And our clients often find it difficult to warm up to us. I think I should actually just put this out there that this superpower is so difficult to develop. You need to find the right things to talk about and the right things to build on and my client was hard of hearing so wow was it difficult to find that connection. There were moments where I wanted to give up and needed a few moments to collect myself because it’s so difficult to communicate with someone in an alternative way to what we’re used to. Here’s an example though, of how I used myself as a therapeutic tool. I used a whiteboard to communicate with the client which made her trust me more when she saw that I was making an effort to communicate with her. Since she began losing her hearing she hadn’t had contact with anyone. Can you imagine living without any social interaction ?? Gosh my heart broke. You could actually see how she opened up when I made an effort to build that trust. It was so heartwarming.
💥 Superpower number #2
Mind reading. I’m our words, empathy. This is where our telepathy skills come in. We don’t just hear words, we dig deeper into the thoughts and feelings of our clients. When we speak to our clients we don’t just hear their words and boom we have a fix. We need to ask more questions and add more value to the conversation to find out what is happening in their minds beneath the surface of what they’re outwardly showing.
💥 Superpower #3: Multicultural Awareness
We as the therapists need to understand their backgrounds, beliefs, and traditions and once we have that foundation built we need to adapt our approach to each therapy session. A shapeshifter of sorts. At the home I’m placed at, Christianity and Catholicism is a very prominent factor that plays a vital role in the residents lives. So many of them hang onto that as their life jacket that’s keeping them floating. Let me tell you guys, my interventions for my previous client was built on this superpower. It was *chefs kiss* if I may say so myself. For my first session I centered it around the Virgin Mary and as soon as I saw my clients eyes light up I knew I had to keep implementing these ideas into all my sessions. And guys … it worked so well I could cry. Although I have to admit, there were times where the line between understanding and accepting another belief and staying firm on my beliefs became slightly blurred. Speaking to someone through a whiteboard is ridiculously difficult and there’s only so much you can write. So when my client started to question my faith I found it so difficult to be able to get her to understand the difference in our religions. At some point it did worry me that I was just stringing along to everything she was saying and it sparked a sense of guilt within me. Because although I was doing it to make communication easier, I was also lying to my client in a way and going against my own beliefs which is definitely not part of this superpower. We need to use ourselves to add to the therapy whilst also maintaining our own values.
💥 Superpower #4: Adaptability (shape shifting)
Adaptability and flexibility are KEY in the therapeutic use of self. Needs if our clients can change in the blink of an eye. So you need to morph into whatever form is needed, always ready to tackle new challenges. Especially at the old age home, one second you’re in your usual OT role and the next you’re the clients new friend that’s learning all about their childhood memories. Side note, elderly people and their jokes and smiles are so precious. I saw a client get a new walker and I found myself stopped in my tracks just observing her little interaction with the nurses dancing and taking photos of her. Sometimes it gets a little overwhelming being in the same place all the time and I know I’ve been feeling it lately. The same routine and problems happening every day can take a toll on you and it’s like you’re just dragging yourself through the hours some days. But it’s moments like those that make you realize that the type of people were working with deserve all our superpowers and that it’s worth using ourselves as a therapeutic tool to achieve those smiles.
So here’s all my superpowers that explain the therapeutic use of self. If I think of any more I’ll be sure to let you know. But before we end off I think it’s important to mention that there will be times when you feel like your superpower isn’t super powering. Does that make sense ? I had a client this week that made me feel like my superpowers had just *poof* vanished and my word did it drain me. Just a little back story, I had received the name of my client and her file with all the necessary information I might need which I decided to look through before I met her. Now, keep in mind her file portrayed her to be a friendly, kind, sociable resident that communicates well etc.

Guys I went up to meet my client and I was practically dragged through mud and then sent back. It’s ok you can laugh, I’m at the stage where I’m laughing about it too. I won’t go into the details of what exactly happened because I don’t think it’s necessary to expose or make fun of elderly behavior seeing as there’s always a reason behind it, be it a psych disorder or general psych problems or problems due to institutionalization etc. The only thing I need to mention is that I had a plan when I went to meet my client with my superhero cape tied on securely and my superpowers ready to use myself as a therapeutic tool but when the session began, everything just left me. My client gave me a lot of trouble and in the moment I decided to scrap all the formal assessments and the planned activity etc. and just try and talk to the client to build that rapport. It still didn’t work out and I became a nuisance to the client which deflated my self esteem and confidence badly. I’ll get it back though I know I will, these things have to happen to be able to learn and I know that. I just felt like I needed to mention that your superpowers don’t always succeed seeing as human beings are very complex beings but the mere fact that we try and use ourselves to help our clients is all we need to be able to keep us motivated to push on.
Moral of the story guys, we’re not just occupational therapists, we’re the superheroes of well being, functionality and independence, especially at my old age home. We don’t just change lives, we save the day, one client at a time (maybe more if it’s a group session but you know I had to say that to be the cheesy little nut that I am)
Thank you guys for staying all the way to the end of my very strangely changed up blog post for the week. Come back again next week, maybe I’ll have another surprise theme going on. Should I make it a thing where I have a new theme every week ? Come back and find out 😉
0 notes
Text
Mental health is the Cinderella of Health Care
Well hello there again, Aisha here, I’m back and ready for the next leg of the OT journey and I hope you are too because we’re going to DisneyLand !
Ha, just kidding. I wish 🥲
Buttt what we are going to do is talk all about everyone’s favorite Disney Princess.
✨Cinderella✨
Ok I know what you’re thinking, what on earth does Cinderella have to do with Occupational Therapy. Let me explain.
‘Mental health is the Cinderella of Health Care’
It’s ok I’ll give you some time to process because it took me quite a while to wrap my head around it. Let’s take a deeper look into the statement and unfold the meaning together and I’ll use my prac over the past 2 weeks to make it easier for all of us to understand.
Firstly, let’s look at the Cinderella herself.
The forgotten child? The imaginary friend? The one that doesn’t matter if they’re not seen or heard, the one that anyone can do whatever they want with and get away with it? You seeing a link ? Yeah. Cool right. I hope you’re all having that ahhh moment as it all clicks because I sure did.
Mental health plays such an important role in shaping a persons behavior. It affects how we think, how we feel and how we act on a daily basis. And yet, it is the least advocated aspect of the healthcare system that we know of. I’m not going to go into much detail on mental health seeing as we did cover some of it in my last post but here’s a link to a site that talks about some pressing mental health issues and the importance of mental health care and I encourage you to read it to get a better understanding of the whole metaphor we’re going into.
There are so many residents at my current placement that present with mental illnesses such as Alzheimer’s disease, Parkinson’s disease and dementia etc. who have not received the necessary help and treatment they required. But they do have nurses who take care of all their physical needs and provide them with the necessary medications and interventions. We’re constantly hearing about new studies and breakthroughs regarding different vaccines, drugs or procedures to cure multiple physical illnesses but how often do we see news or breakthroughs on mental health issues? Now listen, I am in no way saying that there is anything wrong with the physical aspect of health care. Of course all the breakthroughs and discoveries are massive milestones that are helping millions of people across the world. But just to paint a picture for you to understand I’m going to have to paint them as the bad guys…

(my sincerest apologies to all my physical healthcare workers this is purely educational and for imagery purposes only ily 🫶🏼)
As we’ve already established, mental health is Cinderella and all the other physical health factors are the Evil Stepsisters. They’re dressed up, invited to balls and known to everyone just like physical health in the health care system. They’re in the spotlight, have tons of money that funds them and everyone’s talking about the latest updates. And yet where’s Cinderella ? All alone at home working tirelessly with barely any money to fix her clothes and build the life she dreams of. Exactly like mental health in our health care system. Mental health care providers work so hard trying to do the best they can with what they’ve got. And just like Cinderella, we don’t have the funding we need to build up our name nor do we have the status to be the sector we have so much potential to be. At this point we need a fairy god mother to sprinkle some magic on us and transform us into the Princess we were destined to be. Lol.
Ok, I think nows a good time to pause for a second just for me to say that I am in no way directly comparing the Evil stepsisters to our physical health care or health care workers because they clearly deserve every inch of good that comes their way unlike the Evil stepsisters. The problem comes in because mental health is seen as less than when it in fact should be seen as equal to all other aspects of healthcare and we deserve the same recognition and advocacy as the rest of them.
Let’s be honest though, how many of us are guilty of turning a blind eye to our own mental health? How many of us run to the doctor the second we feel a slight stomach ache or fever coming on ? All of us right ? But what do we do when we’re drowning in all of our problems, having panic attacks and struggling to stay afloat because our mental health is plummeting? Nothing right? This is our problem. We’re giving into the Cinderella metaphor.
Actually, before we continue, I myself know how difficult it can be when you’re struggling with your mental health. Trust me, these past few weeks have been a whirlwind with regards to deadlines, tests and other personal issues and I can feel my mental health not being as healthy as it should be. I think something that I’m also struggling with a little is being in an old age home as my placement for this blocks fieldwork. The institutionalization I can see the residents facing is something I find hard to process and cope with seeing as I have not been as exposed to it as I am now being there twice a week. The slow paced, quiet and monotonous atmosphere of the elderly living in the home can be quite draining as a student who is mostly active and stimulated throughout their days. But I’m working on it, I’m journaling and speaking to those close to me to let out my emotions. As of now, I’m not going to let neglecting our mental health slide. Here are some amazing links to sites that allow you to reach out and seek support if you’re struggling with your mental health and I’ll also add contact details of some good therapists that I’ve heard of for any of you that need that support.
“If you’re feeling anxious, confused, hurt, depressed, if you are wondering whether life is worth living … contact the Befrienders today. The service is completely free and confidential”
https://befrienders.co.za
”Worldwide fellowship for alcoholics supporting those choosing to be sober.” - Alcoholics Anonymous South Africa : 0861 435 732
This site lets you take a quiz to help you decide which therapy you’re in need of and then matches you to an online therapist catered to your specific needs. It’s amazing and I highly recommend!

Ok and now back to my point. These past few weeks have given me so much time to sit and reflect on some of the conditions that the residents of the old age home are affected by and it actually shocked me as to how much their mental health has been neglected. In fact, what has brought me to this realization is my own patient. She is a resident at my fieldwork placement this semester and she has been living there for two years now. Nowhere in her social work documents does it give a diagnosis or any medications for mental illness to my client. But after further reading through her file it can be deduced that she experiences delusions and hallucinations that should be a full mental illness diagnosis. When I tell you I was shocked beyond belief. She seemed perfectly healthy for the first 20 minutes that I spent with her but as my sessions with her continued, she showed more and more signs that indicated she has problems with her mental health and yet she was not even referred to a psychiatrist let alone given a diagnosis. My heart broke when I began to think about how this woman has been living her life all these years with these voices and feelings plaguing her every day life. Is this not a perfect example of how mental health is the Cinderella of healthcare? A clients mental health completely disregarded yet her physical reports are very clearly visible in her files numerous times. Cinderella and her Evil step sisters.
I think I’ve made the whole metaphor pretty clear so let’s finish this off. Just like the clock struck 12 and Cinderella returned to who she used to be, we need to ensure we advocate for mental health so much so that we don’t let our clock strike 12 so that mental health can continue flourishing through our conversations and advocacy. We need to be the voice for people like my client and so many others who aren’t receiving the help they need and maybe even through one conversation we can change a life.
Thank you guys for being here, I hope you enjoyed your in-flight entertainment of Disney’s Cinderella and I hope to see you again on the next flight. 🤍
0 notes
Text
Hi there everyone,
I’m back and ready to update you guys on this new journey.
If you thought the last trip had some turbulence I don’t think you are ready for this one …
So this semester is all about psych. Get used to the word because you’re going to be seeing it quite a lot over the next few weeks.
This semester we’re working in John Conradie old age home. Which is a HUGE difference from working on physical aspects in a high turnover hospital like King Edward. The switch from physical to psych may be tough to follow but don’t worry we’re all on this journey together and I know we’ll wrap our heads around it eventually. Oh and not only are we in an old age home, we’ve also started something new where we visit a community in Durban every Monday and trust me when I say there is so much to talk about so fasten your seatbelts as we’re about to takeoff.
In this weeks blog we’re going to be looking back at our journey over the past few years and reflecting on how I’ve grown as a person and how I see myself growing in this new block. First and foremost I want to talk to you guys about the community we’re visiting and how it has already shifted my perspective on this degree and on my life personally.
As of 2022, around 18.2 million people in South Africa live in extreme poverty (You can find a table of the statistics below).
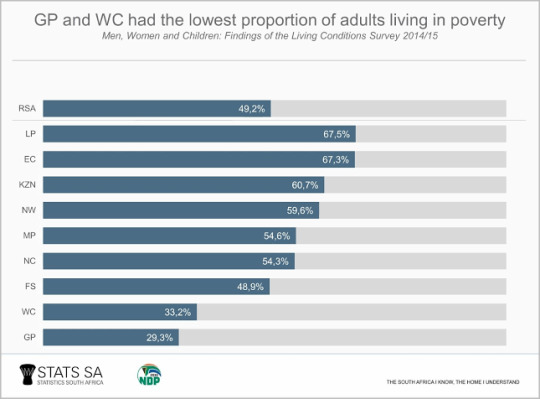
We always drive around and see these communities around Durban and South Africa in general and I know we always feel a pang in our hearts as we drive past thinking about the living situation of those living in the shacks. But let me tell you, nothing, absolutely nothing will prepare you for actually going into these communities and seeing how our own South African people are living. My heart shattered going into the crèche and seeing little kids with such bright smiles and hearty laughs in such poor conditions. Although community block has been such a common conversation amongst us ot students since first year, it was always just a conversation in my head I never actually processed what we were going into. It was as if the second we walked into the community my eyes began to see a whole new perspective on life and I cannot be more grateful that the degree I chose is pushing me to see these things and not keep me closed up in a little box. I cant lie, I am absolutely terrified for what’s next and more so for next years community block like this flight is about to crash. But I know that everything I’ve learnt over the past few years and everything I’m about to learn is what steadies us along this journey and I cannot wait to use my abilities to uplift these communities.
Moving onto the last two days at John Conradie. My word is it a change. I have been in hospitals like King Dinizulu or King Edward since we began fieldwork in second year and although it was difficult and a lot of work I thoroughly enjoyed it. But moving to an old age home has turned my OT world upside down. I’m working with new patients that are elderly and I’ve never worked with them before so their behaviors and their difficulties and problems is something that’s going to take some getting used to. It’s not that theres anything wrong with the facility at all, in fact, TAFTA is doing such incredible things for elderly people in South Africa and just being at John Conradie for 2 days has made me learn so much about them. Their staff are amazing and so kind, they look after the elderly and are so patient with each and every one of them. Below is a link that will lead you to TAFTA’s website which tells you all about their projects and about all the good they’re doing for our elderly South African’s and I suggest you give it a read because it’s honestly so heart warming knowing that there’s organizations like this that care for our people.
Seeing as first year was online, I had no idea what Occupational Therapy actually was. I was terrified that I wouldn’t know what I was doing or that I was doing everything wrong but looking at where I am now makes me so much more confident in my skills. Personal growth often comes from facing challenges and learning from experiences. It's about embracing change, adapting to new situations, and gaining a deeper understanding of yourself and looking back I can confidently say I’ve improved. I’ve learnt about my strengths and weaknesses and found areas that I need to improve in. At this point I can say I’m stronger when it comes to more physical OT aspects compared to psych. At the moment I feel lost starting this new psych block because my brain isn’t wired to think as quickly for a solution to the different problems I’m seeing. But don’t worry guys, this is day 1 of many to come. By the next blog or actually maybe a few later we’ll be seeing a whole new Aisha. My confidence has definitely skyrocketed since psych block last year. I know how to confront my clients and how to adapt to a change in situations but I know from now that I need to work on my interaction with elderly people because their behavior is different to what I’m used to. It’s nothing to worry about, just a little turbulence on our journey but as we already know, no flight on this journey is smooth but we get there eventually. I’ll see you guys on the next leg of this journey with your skills bags packed and ready to take on the next flight. 🫶🏼
0 notes
Text
*airport jingle* Attention, please may all passengers traveling to the End of Fieldwork proceed to boarding gate 6 for flight OT3.
I’m sorry that was so cheesy but I had to add some spice to the last blog of Block 1 for my fieldwork pracs. What a journey it’s been … I’ll admit there were moments where I was ready for an emergency landing because I was ready to give up but I am so proud of myself to pushing through and I know I’ve improved so much since when I first started. I feel like I came into fieldwork completely blind and anxious about failing but here we are all ready to end of fieldwork on a good note.
Let’s get into the last topic for my fieldwork blogs which is all about cultural humility. Which is pretty ironic seeing as I was just exposed to a perfect client to be able to showcase and explain what cultural humility is and why it’s needed in OT. Let’s get the boring stuff out of the way and start by giving you guys a factual definition. The first one is pretty straightforward in explaining that “cultural humility is a practice of self-reflection on how one’s own background and the background of others, impact teaching, learning, research, creative activity, engagement, leadership, etc.” If you’re interested in a more detailed explanation I’ll add the link to guide you guys to learn more about it. Taking a look at my client that I spoke about in last weeks blog, I had an opportunity to practice cultural humility and understand just how important it is to learn from others.
My client is a 33 year old male who practices the Islamic religion. Initially, upon first meeting my client I was not focusing on his religion or culture, I was mainly focused on getting formal assessments done and out of the way. This is where the first mistake I made comes in. Looking back at the way I approached the session I know that I need to improve my cultural awareness of all my clients. In my head I just assumed that he’s Muslim and then pushed those thoughts aside to make space for all the information I needed to gather. I also assumed that, since the client struggled with communication, I was going to have a hard time getting information from him so I didn’t focus too much on his religion and culture. Now if only I could go back in time and shake some sense into myself I would’ve made my life so much easier. If only I went into my initial session with the cultural humility I initially explained to you guys. I know that yes I am a Muslim and you guys are probably like “Aisha why wouldn’t you focus on his religion when you believe the same thing” and yes I completely agree with you. But at the same time cultural humility isn’t just understanding the clients culture, religion and background. It’s understanding how one’s culture can impact a therapy session and how it can impact the clients behavior, learning and participation in the sessions and I did not understand that by me speaking more about and learning more about my clients view of his culture and religion I would be helping to build good rapport and making my sessions much easier regarding his participation.
I first used a grooming session for my clients treatment. Which yes it did have some aspects of meaning to it but nowhere near as much meaning as the next session where I actually took the clients culture and religion into mind and practiced cultural humility by analyzing the meaning it has in his life. After the first treatment session I became more aware of the effect that the clients religion has on his life which then got the ball rolling in my head asking a million and one questions that peaked my interest and got me wanting to know more because I could see the success of my next session improving the more I learned about my clients culture and religion. I didn’t even have to ask about his religion because he would say little prayers in Arabic before every action which showed me how strong his beliefs are. On one hand it made my heart swell because I realized we believe in the same things but on the other hand I felt so guilty that I didn’t even think about his culture before. Not just thinking about cultural humility, I’m talking about being an OT in general. I should have taken the initiative to somehow find out more about his culture instead of ignoring it. This made me begin to reflect on how it affects his recovery and his cognitive abilities which helped me to create and plan my next intervention session which was religious observance.
The first thing I immediately noticed was that my clients participation in the treatment session of religious observance improved drastically. I remember being so surprised when my client was able to upgrade effectively and participate on his own volition which was a huge improvement from his initial assessment. This is evidence enough for you to learn the importance of cultural humility. I barely did anything. Yes ok I did plan my session with a lot of detail by making him take part in the prewashing routine and prayer but I swear as soon as my client stood in the correct way and heard the words of the Quran playing it looked like he was transported to his safe haven. There are no words to explain just how at peace my client seemed. In that initial moment of hearing the words of the Quran “All praise is to God, Lord of the Worlds” I could see my clients body and face calm down and become less tense for the first time since I had met him. From being so tense and tired and looking like he just wanted to give up he now looked more like he was in control again. I feel like him doing something that came so naturally to him and hearing the words that he usually goes to for comfort gave him that sense of normality that he needed once again. In that moment I knew I had a new tool to use as an OT in order to create and carry out successful sessions. He did still have difficulties and struggled with some aspects of the prayer but overall I could see and understand just how important it was for me to take that step towards learning cultural humility. Just a side note that if any of you guys want to listen to the recitation of the Quran that I played for my client I’ll add the link below. There’s a Spotify link and I’ll add a YouTube link in case. You don’t have to be Muslim to be able to feel that sense of serenity. Give it a listen and let me know your thoughts.
youtube
Another aspect of cultural humility that I’d like to touch on is the fact that it’s not just the ability to understand someone else’s culture and the impact on their lives. Cultural humility is a commitment from the therapist to be able to evaluate and critique ones self regarding not just the clients culture and religion but their own as well. This is so that the therapist is not disrespectful and disregarding of the something that means so much to the client. As spoken about above I needed a bit of a wake up call in order to allow myself to reflect on my own beliefs and culture. Yes, I am a Muslim but the effect that Islam has in my life versus the effect it has on my clients life are two very different things. “Cultural humility involves understanding the complexity of identities — that even in sameness there is difference.” That last part really speaks to me. “Even in sameness there is difference”. My client and I may both be Muslim but our journey to finding our faith and the meaning it has in both our lives may be completely different and that is what cultural humility is meant to make you think about. I’m also much younger than my client and we both have been through different things in life. He has just suffered a TBI due to a traumatic accident and I’m a student learning how to treat him. My faith helps me through tough times in my degree when I can feel myself slipping under and not being able to cope with the stress that comes with all my work. But my client on the other hand uses his faith and religion to give him a sense of peace in his world that was just turned upside down. It reminds me of a quote I read that states that “two people can look at the exact same thing and see something totally different” and it’s so true. We can even take a random example to show you guys what this quote means. For example, I can look forward to my birthday because I’m still young and I see my birthday as an exciting milestone in my life but someone else could view their birthday as a burden or as something they aren’t looking forward to because it just means they’re getting older. It’s the same when it comes to cultural humility. Yes I understand my clients culture but do I really understand what it means for my client or am I making assumptions based on one basic idea ?This is why I needed to take a step back and focus on reflecting on my own beliefs whilst I was creating my treatment session. I needed to be able to differentiate between my own faith and my clients faith because I didn’t want to force my way of thinking on him and just assume that he thought and felt the same way I did because I could say something that may make my struggles appear the same as his which will show such entitlement on my part. I knew that I valued my prayers and reading the Quran and that it gave my heart a sense of peace and serenity but I did not know how my client felt about this and how he views these aspects of his religion. So I used this as a learning opportunity and a teaching opportunity to be able to learn about different views on Islam and the different impacts it has on others lives and to teach myself how to implement cultural humility into my every life but also into my service and therapy with my patients. I then also realized that cultural humility is not something that can just appear out of nowhere. Instead it is a form of lifelong learning that requires constant reflection and awareness of others.

Although I’ve been speaking about religion and relating it to cultural humility, I think it’s vital that you understand that cultural humility does not only look at religion and culture. It looks at the clients socioeconomic status, his gender, race, social needs and many other factors. This is something I also had to learn recently. In my head whenever someone mentions culture I always jump to religion which is something that caused my mind to be restricted. After researching cultural humility I felt I needed to open my mind to be able to acknowledge and understand a wide variety of a clients personal life and the impact it has on therapy. I know that as OT’s we need to have a holistic understanding of the client which yes definitely that’s a no brainer. But sometimes we forget to empathize with our clients seeing as we are only focused on creating a treatment session. After realizing my mistake of not having cultural humility I made sure I took moments to myself in the treatment sessions to gather my thoughts and to refer back to the meaning of cultural humility.
Initially I have to admit I was quite upset with myself for making an assumption about my client and sticking with it. If I had just opened my mind and realized the importance of cultural humility I would have had much more success in my treatment sessions from the start because it was so clear that once I became aware of my clients culture and implemented open discussions and added it into my session my clients participation improved ten fold. So here’s my last tip for you guys to take with you on your journey in reaching your destination. Practice cultural humility. Don’t just sit and think “oh it’s fine I already know this client” and then worry about all the facts. Yes, of course the theory is important but once you reach that level of critical thinking and being able to self reflect and analyze your clients lives as well as your own you will unlock unlimited potential and see so much success. This journey has been absolutely amazing and I’m so glad you guys were with me every step of the way. We’ve finally reached our destination. Sala kahle, hamba kahle, totsiens.
1 note
·
View note
Text
Hello there. I hope everyone’s doing well, I know it feels like it’s been an endless journey of long haul flights and some turbulence but here we are almost at the end of our entire journey. I can feel the jet lag already setting in … but let’s push through it and get into this weeks discussion.
What is evidence based practice? I had no idea either up until a few seconds ago when I researched the definition but then I realized it’s something we as OT’s and everyone in the health sciences faculty and professions use in our every day practice. To quote an exact definition, evidence based practice is “a problem-solving and decision making approach in practice that involves the conscientious use of current best research evidence and clinical expertise”. In simpler terms, it’s using research and the results and evidence from research to guide intervention to ensure a successful and meaningful outcome. As we all know there is so much to read up on the internet about absolutely anything and everything and as soon as we type in a question there’s hundreds of articles that pop up giving us all sorts of information. As OT’s we focus a lot on evidence based research seeing as we desire the best possible result from our interventions and because Occupational Therapy is changing every day meaning we need to constantly keep up to date. In todays post we’re going to reflect on my most recent treatment session with a new patient I had this week in order to understand evidence based practice in a practical example.
Just a quick bit of background on my client so you guys have a clearer picture, he suffered a TBI after being hit by a car as he was walking on the side of the road. Initially h experienced right upper and lower limb weakness however, as of the most recent treatment session I had with him he has gained most of his strength back and can mobilize with moderate assistance. He has very low psychological endurance and slow thought processes and he spaces out quite often when being spoken to or when doing an activity. If I’m being honest I have to tell you guys that I was pretty scared of treating my client when I first met him not because of anything else other than the fact that his scars made him look a little intimidating. He’s been through a brain surgery to remove pressure from his brain meaning he had many stitches on his head and severe facial swelling when I first met him. I’m human guys, we all have our own personal demons that we’re fighting and trying to overcome and it’s normal for us to form judgements about someone before we actually meet them. In fact, I remember learning in school that it takes 7 seconds upon seeing a person to make an initial judgement. Sue me, I’m guilty of being human. I admit it, I was pretty anxious going into my initial assessment session not knowing what I was going to find but boy can I tell you my judgement was completely wrong. Although my client didn’t want to talk much and I struggled to get most information from him, as soon as I got over the initial anxiety I could see the pain and utter exhaustion on his face from his experience. This was exactly the wake up call I needed to shake me back to reality and realize that I have the ability to make his life slightly less painful. So I did my assessments, tried as hard as I could to get any information as possible and then left my client to rest because I didn’t want him to be frustrated with me as that would’ve had an impact on our future sessions.
As a therapist there can be frustrating moments when you aren’t getting exactly what you want from a session but you learn to overcome it and find other ways of building that relationship with the client. In my experience I found that religion was the one way I could relate to him and build that rapport in order for him to trust me. After carrying out a grooming activity for my first treatment session I could see I didn’t have my clients full attention and willingness to participate in my session which planted thoughts in my head as to how I should move forward. I was happy with his progress in his physical functioning but I knew I could make his treatment sessions more meaningful to him if I could just figure out the one thing to focus on. That’s when he began saying little prayers in Arabic throughout the session which immediately put off alarm bells in my head as to what I could do for my next session. I came to find out that my client was Muslim and that his prayers meant a lot to him. You can already guess that I got home that day and immediately started on my treatment plan. I have never been more excited for a treatment before because I finally found a way to relate to my client on a deeper spiritual level that I knew would open so many doors for a successful treatment. The only problem was that I had never carried out a treatment session focused on religious observance which once again welcomes back Aisha’s anxiety… I know, I’m just as tired as you guys 😭
But, here’s where we start to look into evidence based practice. Although I did know that there were chances of success if I planned an IADL session around religious observance, I needed factual evidence to back me up and make me feel more secure in my decision and in my treatment. I often second guess myself and as soon as I think i have a good idea I need to run it by people and research in order to make me feel more confident. Sometimes that can be a bad thing in every day life to need validation from people but in OT, the need for evidence to back up my decision is vital, not only for my client but for myself as a therapist and for my service. And so, I went on to research religious observance and how it affects clients participation in treatment as well as the overall success of intervention.
I don’t want to bore you with all the details of my research so I’m just going to touch on a few points that I found important and how it affected my thoughts and planning but I’ll keep the links below for you guys to check out if you’re interested in learning more.
“Research shows that religious and spiritual beliefs influence a person’s health and quality of life.” You hear that ? That’s the sound of success. That’s the first sentence I had read about religious observance and you best believe I was overjoyed seeing as I could already see my treatment plan heading in the right direction. This is not to say that I didn’t have my doubts and worries about my session but the thing with evidence from research is that the practice/treatment idea has been tested and analyzed from a variety of different people which increases the chances of success.
Here’s another example of just how important research is for a therapist. I explained before that I had to wait for my client to utter a prayer in Arabic for me to realize that he was Muslim and so that I could delve further into his religious beliefs. That same study I mentioned above stated that “there is a hesitancy among the respondents to ask the client about religious observance and that therapists are waiting for the client to raise the topic.” Is that not creepily accurate looking at my approach regarding my clients religion ?? Evidence based practice guys, evidence based practice. That’s all I’m saying. Let’s actually touch on that point though. I knew in my second session that I had to start thinking of another session that was more meaningful to my client but for some reason I was scared to try and bring up religion. My clients name is a very common Muslim name which I did pick up on but for some reason I was hesitant to ask him about Islam in case I was just making assumptions and I didn’t want to make a fool of myself. Once again, yes guys, I’m human. I have thoughts that hold me back some times and this was one of those times. If it doesn’t make sense to you then think of it like this. What if I assumed that my client was Muslim and started using Arabic phrases and prayers throughout the session only to later find out that he is no longer Muslim for personal reasons that affected him emotionally. I didn’t want to be the one to bring up any negative past experiences because I was scared it would ruin the relationship I was trying to build. Which I mean now that I’m looking back at it, I still do understand why I thought what I did but the whole religion thing turned out to be such a life saver for my success in the following treatment session. I really do make my life harder sometimes. But I blame my brain for the millions of thoughts that run wild, it’s a blessing and curse 😭.
As you can probably already guess, my treatment session was quite a success in my books. In prior assessment and treatment sessions he could barely concentrate and didn’t seem very interested in my treatment but as soon as I told him about the treatment session being about his prayer I could already sense the shift in his willingness to participate. Seeing as we are currently in the month of Ramadan and it is a month where Muslims increase in their prayers other than just the 5 daily prayers I could sense the urge for my client to want to carry out this occupation. As a Muslim myself, I also know the feeling of peace and comfort you get when carrying out these prayers and I could immediately see my clients entire body relax and be at peace when I began playing the prayers for him and when he was reciting it himself. I’m going to get a little deep here and say that my heart swelled at the sight of someone looking like they were wrapped in a blanket of peace as soon as the prayer began. There’s a specific verse in the Quran that states that “God does not burden a soul beyond that it can bear” which always brings me comfort knowing I can get through whatever it is I am dealing with and in the treatment session this is the verse I had been repeating to my client to assure him and provide more comfort seeing as he has been through such a traumatic experience and is having to deal with a difficult recovery. I have recently been exploring my faith and trying to strengthen my relationship with God and increasing my prayers and I too have felt just how incredible it is knowing I can turn to my religion whenever I’m anxious or whenever I need those moments of comfort and peace and seeing my client in that same feeling brought tears to my eyes knowing I was able to bring that sense of normality back into his life.
Going back to the topic of evidence based practice, there was another moment after my session and evaluation that I found the need to research a different topic. This being how therapists and doctors communicate with their patients. After my evaluation it came to my attention that there were moments where I spoke to my client in a tone that was not necessarily appropriate for an adult. This was a hard pill for me to swallow because I didn’t realize it at all during my session and I am usually the one who gets frustrated with doctors when they speak to their patients like children so this feedback kind of made me upset with myself for a bit. But of course, I’m still a student, there are going to be moments where I mess up and need to learn and although it is frustrating thinking back on it and knowing I can’t change it I know I am definitely going to use this as a lesson going forward. This is why I began to research and look into the effect that “baby talk” (although I was not using complete baby talk I knew that was a risk for future sessions) with clients and found the following “many people, who are often already struggling with negative feelings of self-worth as they begin to lose their independence, feel degraded by baby talk” and “the recipients of baby talk were perceived to be less satisfied with the interaction.” I’ll link the websites below for you to read into this a bit more because I found it quite interesting but the above information was the wake up call I needed to be able to adjust my handling of my clients in future sessions.
Looking back at my approach to my clients treatment from the beginning of the week to now I’d say there’s a huge improvement not only in my approach but also with my relationship with my client. Of course as stated previously there are things I need to work on but overall in my opinion I think this week was a success. I feel like the past weeks have been amazing in preparing me for this client and I know I used past experiences and feedback to improve which I’m proud of. And before I end off todays post I just wanted to reiterate the fact that yes we are all human. There’s personal feelings that pop up in moments of anxiety and that’s normal, it took me a while to be able to process that and not to attack myself for those thoughts and judgements but I hope that me admitting my faults and acknowledging my weak spots I can be an example to you guys that are also trying to navigate your way through this journey. I’ll see you guys again one last time for our final flight of this whirlwind of a journey to our final destination next week.
0 notes
Text
Hi everyone, welcome aboard the OT flight to our final destination. After what feels like an extremely long stopover due to external influences like the strikes and protests that were going on we can finally begin our last leg of this journey.
In today’s post I’m going to be talking about working as an OT within a multidisciplinary team (MDT). As OT’s we work with a number of different health professionals in hospitals such as doctors, physiotherapists, nurses, speech therapists, audiologists and other OT staff etc. To quote a theoretical definition of MDT’s “it bring(s) together the expertise and skills of different professionals to assess, plan and manage care jointly” and “are expected to work proactively to support individuals’ care goals”. This means that we all need to work together in order to provide the best possible care for our patients as possible. I’ve provided a link below where you can read more about MDT’s if you’d like a deeper theoretical understanding but in today’s post we’re going to look at my experience and my understanding of MDT’s as well as my approach and feedback to the recent treatment of my client.
In my opinion, working in an MDT at a public hospital is a lot harder than working in a private practice. This is because the patient turnover at these hospitals are extremely high meaning that doctors and other health professionals don’t have a lot of time to sit and communicate and plan interventions with others. It’s more of a quick referral or a quick word or two in passing to determine what the client needs and then off to the next patient which is completely understandable seeing as there are so many patients to see in one day and more patients are waiting to be admitted. However, although these communications are quick and brief it provides a lot of information on what needs to be done and it also lets the therapist know that we need to move fast before the client is discharged.
Looking specifically at my experience of working in an MDT I can say there is one problem I find dealing with quite often that I’m sure many OT’s can relate to and that is the constant question of “what do OT’s do?” or “what is Occupational Therapy?” Within the past few weeks I’ve had a number of other health professionals like doctors and physiotherapists asking me these questions and to be honest I find it so difficult to put just one answer to the question. As an OT student I’m still learning myself which makes it quite difficult to put the words together to explain the deeper meaning of Occupational Therapy because most people often confuse us with physiotherapy. To be completely honest I get quite frustrated when trying to explain the meaning of OT to others because I can see that they don’t exactly understand it fully or that they understand one aspect and not another when I actually want them to be able to understand the effect that OT’s can have on patients lives. It means a lot to me but it’s so difficult to use the correct words to convey the meaning effectively. This is definitely something I know I need to work on and I’ve already started to make a little note on my phone from the different articles I read with what to say when someone asks those questions. If anyone’s interested I’ll link a few websites at the end of today’s post to give you a better understanding into OT and so maybe you won’t be the one that asks every Occupational Therapist about what their job is … 🤣

I don’t know if this makes sense but having others question your field of work feels quite degrading especially in a professional setting. I had an encounter with a doctor whilst I was assessing my first patient and him being in my session and watching what I do and then questioning what OT was not only made me nervous but it also made me feel like my abilities were being undermined seeing as he only focused on one aspect of OT being fine motor skills. Although I definitely understand where the question comes from I can’t help but feel anxious knowing I need to explain it perfectly so that I can be seen in the same light as other health professionals. Another problem that I personally face when it comes to working in a multidisciplinary team is the fact that I have social anxiety. I feel like everyone is judging me when I say something and I overthink everything that comes out of my mouth after I’ve said it. I remember meeting one of the medical interns on my first day at the hospital and wanting to kick myself afterwards because I felt like I was not confident enough and that I looked too nervous to be in a professional setting. When I first started working in hospitals in physical block I knew this was something I needed to work so hopefully being exposed to a bigger social network and a number of health professionals in the MDT will help me get over my social anxiety and become more confident in my ability to speak and communicate with others.
Despite my own personal feelings related to working in an MDT there are without a doubt so many benefits of working in a multidisciplinary team that create the best possible outcome for the patient. I’ve heard many stories from my friends working with me at King Edward Hospital that they’ve had to work with a physiotherapist in the same session and they explained how interesting it was to see other fields of work and that it was a great way to work as a team to gain the same good session outside. Working in an MDT requires teamwork and it allows us to provide a holistic and integrated approach to treatment through looking at the clients needs, strengths and personal goals. Looking specifically at my treatment from last week with my patient I spoke with her doctor in order to determine if there were any precautions I needed to take during my clients session. I then also had a little conversation speaking about the clients discharge and her way forward regarding her treatment and medications seeing as she will still be recovering from disseminated TB. This gave me a very good understanding of what to look at and focus on during my session and it also made me realize that I needed to get as much as I possibly could done in the session seeing as the client was being discharged the day after. Although I do have my own personal hurdles that I need to jump over regarding working in a multi disciplinary team I can without a doubt say that it is so beneficial not just for the client but for the therapist as well as it assisted me in gaining a better understanding of my client.
After speaking with the doctor and carrying out my session with the necessary precautions there were somethings I needed to improve on and add to my session in order to make it more client centered. I used all the information I received when planning my treatment session and looking back at last weeks blog I’m sure you guys know I was very happy about the outcome of the treatment session which is pure evidence of the positives that come with working in an MDT. However, after this weeks feedback of my session it was brought to my attention that I could’ve implemented the exercise session into the daily routine of my patient so that I could ensure that she has time to fit it into her busy day. My supervisor also explained that I could add her needing to take her medications into my treatment plan as well which makes so much sense now that I’m reflecting on working in an MDT. Speaking with the doctor and understanding the importance for the client to take her medications every day on time meant I should have assisted the client in ensuring she has a set time in the day to take her medication by making her do her exercise routine immediately after taking her tablets in the morning. This way she would remember to take all her medication and she would fit the exercise routine into her busy school day. I found such a cute template online that I could’ve written up for my client and I’m so devastated that I didn’t get to use it but I’ll attach it below for anyone that would like to use it and hopefully I’ll remember to use it myself next time. There’s also a few people I’ve seen on Instagram that make personalized templates for routines and schedules I’ll add their Instagram handles below as well.

https://instagram.com/design_ink_?igshid=YmMyMTA2M2Y=
I hope today’s post gave you a bit of insight into working in a multidisciplinary team as an Occupational Therapist and please don’t take my personal experience as your own. Each person feels a different way and looks at situations differently. Things may be frustrating for me and there are things I need to work on to better myself and my service as an OT but if you’re reading this and you feel differently I one hundred percent understand and I’m sure there are other hurdles you feel you need to jump over. This journey is tailored differently for each person and I hope you can take some good points away from todays post and use it in your personal growth and journey. I’ll see you guys have here again for the next flight of this journey taking us to our final destination.
Don’t forget here’s a list of OT websites if anyones looking at learning more about OT.
0 notes
Text
Hello again and welcome to the next leg of this very turbulent journey. Today we’re going to be speaking all about clients and what OT’s need to focus on in order to ensure the best quality service.
There’s a term used by many therapists across the board that’s used to describe the mindset and method behind treating patients. This is called ‘client centeredness’. It’s basically explaining that the service you provide needs to revolve around the client and they need to be the ones to decide and guide your therapy session. There’s a number of different articles explaining the term client centered which I’ll link below if anyone wants to gain a deeper factual understanding of the term. However, the way I understand the term ‘client centered’ is meaning that the therapist needs to be empathetic towards the client instead of sympathetic and think about what would make the clients therapy more meaningful to them whilst looking at their context and background etc. The client’s beliefs, values, interests, routine and goals etc. all need to be taken into account and prioritized when creating a treatment plan to ensure that the client not only enjoys the session but to ensure that the client is able to understand the benefits and meaning behind the aim of the session and so that they are motivated and can easily implement the outcomes of the session to their daily lives.
In order to better understand this term let’s take a look at my client and my treatment session from this week. My client is a 16 year old girl who was diagnosed with disseminated TB last year December and she has been in the hospital ever since. She had been recovering well and was able to carry out full ROM with full muscle strength and all her major physical client factors were intact except for her cardiovascular endurance. Now it may seem that my client is good to go and can be discharged. However, I knew that as an Occupational Therapist I needed to take a deeper look into my clients life and determine any psychological problems coexisting with her physical problems. That’s when I decided to focus on her self esteem and confidence as well as her anxiety. I knew that as a 16 year old being in the hospital for so long would most definitely have an effect on her mental well being and not just her physical. Throughout the different sessions with her I formed a strong bond that made her comfortable enough with me to share personal feelings and emotions which deepened my knowledge and understanding as a therapist and allowed me to mentally plan and think about what to focus on in my treatment session. Looking back at the different times I visited my client I can see such a clear change in her behavior and her comfort since the first session. When I first met her I knew that there was a barrier that needed to be broken because she probably saw me as a doctor and didn’t feel like she could trust me or talk to me. However, within the last few sessions I could feel such a major shift in our relationship. Although it still remained a therapist-client relationship I could feel that she was a lot more open and trusting of me which not only made my job a lot easier but it personally gave me such an intense feeling of fulfillment and pride in my degree and my future job.
Seeing as my client became more comfortable with me I was able to gain a deeper understanding into her life. I learnt about her interests and about the different things that make her happy and excited and about how she was feeling being a young girl in hospital for a long period of time. She loves reading and playing chess and the most exciting thing that she was looking forward to once she was discharged was to return to school and catch up on her studies in grade 11. This is now where my focus for a client centered treatment session came into my head. Immediately as she mentioned that she was excited for school the thoughts that went through my head was “how will she manage all the walking?” “Will she be able to run to class if she’s late?” “Will she be able to carry all her books and her heavy backpack?”. There was also another problem standing in my way of creating a session write up. I was not sure on how exactly I was supposed to improve cardiovascular endurance. I have to admit I was a little scared to ask my supervisor on advice because I thought that I should know this already but my anxiety was easily diminished when Ms S helped me without question and guided me to research and come up with a treatment. Here’s a link below on cardiovascular endurance and how to improve it. I know it came in extremely handy for me when I needed to learn about it so I’m hoping it can help some of you as well.
However, other than just my clients cardiovascular endurance I couldn’t help but put myself in her shoes and feel what it’s like to be so young and away from your family and friends for so long. Being stuck in a hospital bed with nothing else to do other than walk around and see other sick people is emotionally draining and a child her age would be finding it so difficult to keep a positive attitude. I remember the thoughts and emotions raving through my mind and I couldn’t wait to sit and plan a treatment session for this client because there were so many things I could bring into my session that would not only make her excited but also ensure I maintained the principle of being client centered.
So off I go to sit and plan a treatment session for my demo that I was going to be assessed on by Ms S. Although it was meant to be a daunting experience I remember sitting down to write up a session plan with absolutely no anxiety for the first time in my life. Imagine that, Aisha not feeling anxious. I know right, I’m surprised myself. I was so excited to create a fun but therapeutic session for my client. With both her physical problem of poor cardiovascular endurance as well as her low self esteem, mood and confidence in mind I decided to plan a session that would target all these factors. But … How will I make the session client centered ?? How do I aim at treating cardiovascular endurance but also keep the session client centered ?? My brain was all over the place. However, all my clients points about her interests in going back to school and her values of the importance of family suddenly got me thinking. I could see that her eyes lit up every time I mentioned going back to school and being back at home and playing with her siblings. My heart swelled at the hope that she will be discharged and will be able to continue life as normal without feeling so alone and secluded. I also knew that my client would be grateful to be able to leave the ward and do something different for once. She looked so excited every time I went to see her because she knew I wasn’t there to poke her with needles or get tests done and give her bad news etc. which is why I felt so at ease going to see her knowing she appreciates me and my work as an occupational therapist. So off I went writing up a session to prepare my client to back to the real world far away from the hospital setting because I know she never wants to see ward N5A again. The only thing left to do once I write up a session plan was to carry out the session.
I have never been more happy with how a session turned out than this session with my client. I planned an exercise routine to demonstrate and explain to my client so that she can improve her cardiovascular endurance. But I made it focused around her going back to school because I remember being in school and the intense amount of running to and from classes and the numerous flights of stairs I needed to walk up to reach a different classroom. Let’s just say I felt absolutely exhausted just thinking about it so I can’t imagine how difficult it would be for my client to go back to school when she was struggling to walk up one flight of stairs without running out of breath. In order to make my session more client centered I constantly related every exercise and even the breaks in between the exercises back to my clients school life. I could see her facial expression brighten every time I reminded her why I was doing the session which made me even more aware of the importance of a session being client centered.
Although I felt a great sense of fulfillment after my session and my client was excited and in a good mood there were a few things I could’ve done to improve on the principle of being client centered. One comment that was made by my supervisor was that I should’ve made the exercise routine less of a chore and more of an exciting activity that the client would want to take part in every day. Since she had to repeat the routine at home in her own time I should’ve taken into account that she may get bored or she may not want to carry out the task because she was getting too tired or she just didn’t feel like. This is where I could’ve focused the session more on the client and brought in music that she liked so that she could enjoy carrying out the full routine and so that she can focus on something other than her feeling tired and needing a break. Once the realization hit me that I should’ve included music in my session I literally wanted to hit myself. Every single song I could think of ran through my head and I kept thinking “omg that would’ve been such a perfect song”. That was such a simple yet clever idea I cannot believe I didn’t think of that. I could’ve even gotten my client to make a playlist on her tablet so do the exercises to. My client is a young teenager of course she liked music and of course it would motivate her to carry out her exercise routine. There are so many incredible people that speak about how magic can transport you and take you to a different place and how it’s their safe place. I remember seeing a quote by Elton John that said “music has a healing power. It has the ability to take people out of themselves for a few hours” and I seriously cannot agree more. Of course my client would only need a few minutes to do her exercise routine but it would be such a great escape for her to let out her emotions and focus on something other than her being tired and out of breath. I know that when I go to the gym or when I do any sort of exercise my mind feels so at ease and I can let out all my emotions whilst I’m listening to my music which is why my feedback was so important to me for my future therapy sessions. I was actually quite bummed when I realized I missed such a good opportunity. But immediately after my evaluation was over I went back to my client to explain to her that she could add music into her routine and I felt a weight lifted off my shoulders. At least I didn’t completely waste the opportunity. It still bothers me now that I didn’t make the session more fun because I know it would’ve motivated my client more but everything happens for a reason and I know that I was meant to learn from that so hopefully I’ll be able to implement this lesson with a different client later on.

I knew that I had decided to study Occupational Therapy for a reason but after a rough time and struggling with my studies I began to forget why I had chosen this field of study. After the number of different sessions with my client and especially after my final treatment session, all my motivation and reasons as to why I’m in this field finally came back to me. That sense of fulfillment knowing I made a difference in someone’s life and that I formed a good professional relationship with my client is an unmatched feeling and I cannot wait for more chances to learn and for more experiences like this. Now onto the next leg of this trip, the final destination for this semester. I’ll see you guys again next week, let’s hope it’s a smooth ride…
1 note
·
View note
Text
Hi there, and welcome to my first ever blog post on my Occupational Therapy experience as a third year student.
This first blog post is going to be one of many steps in my journey to finding myself as an occupational therapist. Along the way we’ll be looking at my experiences at my hospital placement which is at King Edward Hospital as well as my emotional and psychological growth and development throughout the weeks. There may be some turbulence along the way but I can assure you that this flight is going to reach its destination come rain or shine.
Let’s begin by taking a look at my first week at King Edward Hospital. As I’ve been told many times before my anxiety is written on my face so let’s picture 3rd year student Aisha walking into hospital looking absolutely terrified. Walking into an unfamiliar place with the pressure of needing to understand both assessment and treatment for the first time can be a lot to handle. There’s also the added pressure of needing to cope and do well under real life circumstances with real patients which can be very daunting at first. However, despite the anxiety, I can also say I was quite excited to be stepping into a new environment ready to learn and grow. Along with being in a new environment I was also exposed to meeting new people within the Occupational Therapy field. This includes the OT’s in the department as well as the students completing their com serve and last but certainly not least my new supervisor Ms S. Correct me if I’m wrong but when I said supervisor I’m sure you immediately assumed the worst. Don’t worry, I did too. But I can gladly say that my assumptions were exceptionally wrong. Ms S’s first meeting with us at the hospital went much better than I expected. Although Ms S is going to be assessing and evaluating us on our demo’s and presentations and judging our clinical performance it was a huge pressure lifted off my shoulders after the first meeting with her as she explained that she is here to guide us and help us learn and that she wants to be the supervisor she’s always wanted. She clearly went through all the expectations of the students and the supervisor and she cleared up all confusion. Every day you can feel the tension in the room dissolve throughout our meetings which is honestly a lovely start to the day and a great way to ease the clear panic that’s written on all our faces.
Moving onto assessments. As OT’s we need to assess a wide range of client factors and performance skills of our clients in order to determine which aspects need improvement and to determine which occupations the clients deem meaningful so that we can build on those during the treatment sessions and improve their overall functioning and independence. Throughout second year we focused only on assessments meaning we should have been quite confident when assessing our clients. However, prior to meeting my client I was worried on how I was going to get all the information from him in a short span of time and upon meeting my client and finding out that he was in critical condition my anxiety skyrocketed. My initial interview and informal assessment sessions went well and I gathered as much information as possible despite the communication difficulty. However, once it came to the formal assessment session I was very nervous. This is when Ms S swoops in and saves the day as she called us into one of the OT rooms to observe her assess a patient and we could assist her along the way as well. I somehow volunteered to assist in transferring the patient from the wheelchair to the plinth even though I’d never done it on a patient before but looking back I’m so glad I gathered up the courage to assist as it gave me a chance to practice and learn being fully hand on with a patient. After that session, despite still being a little nervous, I was more confident on how to go into the formal assessment session with my client. I mustered up as much confidence as I could and assessed my client to the best of my ability and in my opinion I can say that the session went pretty well. Of course there are always troubles and problems along the way. In my case, my client was seriously critical. He was constantly groaning in pain and sometimes refused to carry out a task due to the pain and due to his severe cough and chest and abdominal issues.
After looking at my assessment findings and getting to know my patient better, I decided to carry out a treatment session that focused on a basic ADL of eating which incorporated transfers and mobility into the session. In OT we have something called Applied Frames of Reference’s (AFR’s) which uses different theories to guide therapists in evaluating, assessing and treating our patients. I’ve attached a link below for those that want to get a better understanding into exactly what AFR’s are and how they work. I have to be completely honest here and say that I did not know how to apply my AFR’s as well as I should and I did not know how important they were until we started to look at treatment this year when I noticed what a big role it plays in developing a treatment session. When getting feedback from Ms S on my treatment write up I was shocked to see how unaware I was of just how important AFR’s and models are in understanding how to assess and treat my patient. It came to my realization that if I been exposed to them more and did my own work behind the basics that were taught I would have been able to improve greatly, not only with this years treatment write up but also looking at last years assessment block. Going forward, I know now to always reference my AFR and to dig deeper into understanding the why of what is being assessed and treated in order to further improve my occupational therapy service to my clients daily. It can be hard seeing so many markings on your work that you thought would’ve done well but I can gladly say that I love constructive criticism and I try to improve to the best of my ability which is exactly what I will be doing for the rest of today once I get my very well-deserved nap in.
Although as stated before, I was quite excited to jump into things last week. This week came as more of a slow start seeing as Mondays prac was cancelled due to striking. I was extremely tired and quite honestly not in the mood to wake up early this morning and head to prac. However, once I managed to get myself there and after seeing my friends all ready to take on the day I felt myself ease up and feel more lively. The meeting with Ms S this morning also helped to clear my head and organize everything that needed to be done for this week and the next. So on we go to begin our treatment session with our original client and our next assessment session with another client.
*Alert: bad news incoming*
Unfortunately my client passed away earlier this week and I was unable to carry out my treatment session. It’s a very strange feeling having a client pass away and it may be difficult to understand but it’s heartbreaking for me as a therapist to know that my client had so much potential but he is no longer here to fulfill those treatment goals. As occupational therapists you look into the life of your client and gain an understanding into who he is and where they come from etc. which is why it is a tough pill to swallow knowing your client has passed. Seeing as this is the first time I’ve experienced a client passing away I was unaware of how I should feel and move forward which is why I turned to trust ole Google to research the effects and way forward after a patient passes. One of the points I read was to take time, even just a moment, to yourself and to talk with your peers to allow yourself to process the situation (Paul, 2021). Which is exactly what I did, I stepped out of the ward after finding out about my clients passing just to take a breath and process the information. I then went to my friends from my group to let them know and found comfort in their words. If there’s anyone reading this that’s facing a patient passing away, I’ve attached a link to the post for you to read and hopefully it’ll help you too.
Studying OT also means you turn into an OT nerd and I remember scrolling through Ot quotes last year to find the motivation to work hard. I remember coming across a quote that said “You treat a disease: you win, you lose. You treat a person: I guarantee you win — no matter what the outcome.” By Dr Hunter played by Robin Williams from a movie called Patch Adams. It really made me realize that despite my patient passing I know as an OT I treated him as a person and I know that I added even a speck of hope or joy in his life prior to his passing.
Despite being a little sad and down, I decided that I am not taking this as a bowling ball that just knocked me down. Instead, I am using this as a learning experience and pushing forward to focus on meeting and assessing my new patient which was done today and will hopefully be used as my client for my case study. This client is not as critical as the previous client however there are complications to her assessment due to her post stroke impairments and since she is quite old but after learning so much last week and from today as well I’m ready to face the next session with as much confidence and skill as I can.
In conclusion, as you can clearly see there was a bit of turbulence on the first leg of this journey. However, I’m ready to head into the next part of the trip with new skills, a newfound confidence in the field and a little chant in my head screaming “AFR’s, AFR’s, AFR’s” as I go along with the rest of me sessions. I hope you enjoyed my reflection into the past week and todays session and I look forward to traveling with you again soon. See you next week ;)
0 notes