#prophylaxis
Text

Test My PrEP! 💊
4 notes
·
View notes
Text
When it comes to good oral health, professional teeth cleaning is essential to avoid common dental problems. Your dentist will likely recommend a dental cleaning during your routine checkup. Knowing the various types can be helpful when discussing your options with your dentist.
0 notes
Text
EMS Airflow Prophylaxis
EMS AIRFLOW PROPHYLAXIS
GBT (GUIDED BIOFILM THERAPY)
-PIEZON® HANDPIECE
-AIRFLOW® MAX HANDPIECE
-PERIOFLOW® HANDPIECE
-CAPSULE – The AIRFLOW® powder capsule is made from a polymerized impact & chemically resistant material, offering significant gains in efficiency and ergonomics with a high-volume capacity.
-PRESSURIZATION TOWER – New state-of-the-art pressurization system pressurizing and depressurizing within seconds with an integrated magnetic connection.
-BOTTLES – Equipped with 2 transparent bottles: PIEZON® and NIGHT CLEANER. The PIEZON® bottle comes with the ability to use specific disinfection solutions as well as distilled water. The NIGHT CLEANER bottle provides end of the day waterline cleaning & disinfection.
-INTERACTIVE TOUCH PANEL – Simple and ergonomic, the new EMS touch panel comes with a 10 level responsive interface that regulates and manually adjusts the AIRFLOW® and PIEZON® power level. It also includes an adjustable temperature and volume control feature with operating sound notifications and maintenance reminder.
-NEW CORD – Durable and more efficient, the new EMS cord has a ‘plug-and-play’ system that is easily detachable and simple to service. Powder tubes are made with surgical stainless steel for longer lifespan. An all-in-one robust Handpiece holder with integrated water supply system.
-PEDAL – Wireless stainless steel foot-pedal with boost mode. 360º power activation access.
-EXTERNAL FILTERS – transparent air & water filters allowing for an easy check at a glance.
0 notes
Text
Thick black gay big assTwerk
Virgin teen masturbation A Taste Of The Holidays
Ffm threesome anal sex in public
Hottie goes impure with a handsome fellow in a bang bus
Brunette gf loves deep anal for the first time
Cojiendo A Una Mami
TS Alisia Rae hard ass penetration by Eli Hunter
Porn For Women Hot Real Couple Have Passionate Sex On Stairway with Orgasms
Boy nude in public free s hd gay xxx hot gay public sex
Hot Latina sucks and gags on her toy
#worky#scawtite#polymorph#prophylaxis#rumblement#horometrical#gaitt#archae-#wirra#Melrose#pentachenium#paralysing#rhinenchysis#osteogen#curie#disestablismentarian#glottitis#nectar-streaming#higuero#renatures
0 notes
Text
Influenza Persists by Uday Jain in Journal of Clinical and Medical Images, Case Reports (JCMICR)
Introduction
In the US, influenza (flu) causes 9 to 45 million illnesses, leading to 12,000 to 61,000 deaths annually (10.1001/jama.2020.14772). World Health Organization estimates that worldwide annually there are about one billion infections, 3-5 million severe illnesses, and 300,000-500,000 deaths (10.1038/s41572-018-0002-y). Influenza is caused primarily by influenza A and influenza B viruses. Influenza A is the cause of pandemics. A schematic diagram of influenza A virus is presented in (Figure 1). Influenza will continue to be prevalent because its current vaccines are safe but only 30-60% efficacious. In contradistinction, COVID-19 vaccines have an efficacy of about 90%. Additionally, new zoonotic influenza strains intermittently migrate to humans. Influenza is a major part of “The New Normal
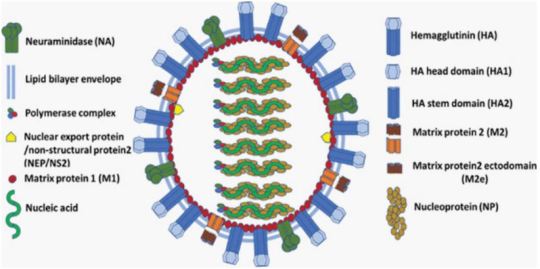
Figure 1: A schematic diagram of influenza A virus.
Coinfection
Since the start of COVID-19 pandemic, influenza is of greater concern. Overlapping spread of both diseases is a major strain on the health care system. Their coinfection is not common but may cause more severe disease. Influenza vaccination and therapy are important in addition to COVID-19 vaccination and therapy, especially in persons at increased risk.
Incubation
Influenza’s median incubation period is 2 days. Patients are infectious for a day before and 5 to 7 days after symptoms. COVID-19 has an incubation period of 4-12 days, a median of about 5 days. Patients are most infectious from 2 days before symptom onset. Influenza symptoms peak in 3-7 days. COVID-19 symptoms peak in second or third week. The spread of both viruses is facilitated by transmission by asymptomatic patients.
Transmission
About one-half of influenza A cases are due to aerosol transmission (10.1038/s41598-019-38825-y). Adequate ventilation can reduce it. Precautions utilized during the COVID-19 pandemic reduced the incidence of influenza in 2020. Used appropriately, surgical masks reduce the concentration of aerosolized influenza virus by about ten-fold and are adequate for prophylaxis against influenza (10.1016/j.jhin.2013.02.007; 10.7326/M20-3213). Transmission by respiratory droplets can also be reduced by masking. Transmission by direct contact can be reduced by hand and general hygiene. COVID-19 is transmitted in a similar manner. Social distancing reduces transmission by all the mechanisms. Influenza is less contagious and causes less severe disease than COVID-19. Quarantine recommended for COVID-19 patients is not necessary for those with influenza. Children play an important role in transmitting influenza. Healthcare providers should take precautions to avoid infecting themselves and others.
Influenza-Like Illness (ILI)
The Centers for Disease Control define ILI as fever 100°F (38°C) or greater and cough or sour throat that is not due to another known cause including streptococcal pharyngitis (strep throat). ILI’s causes can be benign such as common cold (nasopharyngitis caused by rhinovirus or other viruses) or severe including sepsis, meningitis, COVID-19, and SARS. Often there is an abrupt onset. SARS leads to severe disease in most of the infected. Influenza and COVID-19 cause mild disease in most of the infected (10.1016/S1473-3099(20)30484-9). SARS is currently not prevalent. Severe disease due to COVID-19 and SARS occurs primarily in the elderly. Influenza is more evenly distributed across the age groups. ILI can cause immunosuppression, leading to bacterial pneumonia, necessitating antibiotics (10.1097/QCO.0000000000000347).
After general anesthesia, children with influenza have a longer hospital length of stay and increased risk of requiring intensive care (10.1186/1471-2253-11-16). Routine surgery should be postponed for about four weeks in a patient with ILI. Unvaccinated patient should be offered influenza vaccination after the acute phase of ILI has passed and before the surgery. Before performing urgent surgery, severe causes of ILI should be excluded
Upper Respiratory Tract Infection (URI) Excluding ILI
In cold weather URI is common, especially in children. Often it is due to common cold, or noninfectious allergic or vasomotor rhinitis. Less commonly, it can be early presentation of more serious illness including ILI, COVID-19, strep throat, and herpes simplex. Early in infection it is difficult to distinguish between different etiologies of URI.
URI may cause sneezing, coughing, headache, malaise, rhinorrhea, sore throat, sinusitis, and bronchitis. Subsequently, bronchi may be hyperreactive for about six weeks. Pulmonary complications associated with surgery in a patient with URI are bronchospasm, laryngospasm, coughing, breath holding, postintubation croup, episodes of desaturation, atelectasis, and pneumonia. Anticholinergics and bronchodilators may not be beneficial. Perioperatively, adequate hydration and humidification should be maintained. There are no pediatric or adult anesthesia closed claims that implicate URIs including influenza with serious adverse events. There is a very small incidence of viral myocarditis in patients with URI including ILI. It may lead to serious arrhythmias and refractory heart failure (10.1016/j.jcrc.2018.06.001; 10.1038/s41569-020-00435-x).
Diagnostics Tests
These include nucleic acid amplification via polymerase chain reaction (PCR) and antigen-based immunological assays. A PCR test can be performed even at the point-of-care with results available within an hour (10.1016/S2213-2600(20)30469-0). This can facilitate infection control and utilization of antiviral therapeutics. It is especially useful for patients who have severe symptoms or are hospitalized. Test for COVID-19 may also be performed if indicated.
Influenza Vaccine
It is the best preventive measure. Although not very efficacious, it substantially reduces morbidity and mortality because of high prevalence of influenza. It is recommended for anyone over 6 months of age. It is especially beneficial in the presence of age <2 years or >65 years, pregnancy, and pre-existing conditions (10.1001/jama.2020.14772). Lack of vaccination in pregnancy not only increases the risk to mother but also increases the risk of preterm birth, fetal death, infant respiratory infection and hospital admission. The T cell response vaccines elicit is substantially weaker than the antibody response. Children may need two doses of vaccine, at least four weeks apart. The vaccine should be administered at least one week before surgery. It takes two weeks to develop full effect. As the protection wanes over time, mid-September to mid-October is preferred for vaccination. Influenza and COVID-19 vaccines may be administered together. The vaccine may be administered to surgical inpatients (10.7326/M15-1667).
Available Vaccines
The influenza virus mutates frequently. Quadrivalent vaccines protect against four of the currently most prevalent strains of influenza. The vaccines are altered every year for the predicted prevalent strains. Nine vaccines from four manufacturers are available in the US. Inactivated influenza vaccine is most commonly used. It is approved for persons above 6 months of age. As older individuals have a reduced response, vaccines that have a higher dose or are adjuvanted are recommended for persons above 65 years of age. The vaccine is usually administered intramuscular, but a lower dose intradermal vaccine is non-inferior (10.1001/jamanetworkopen.2020.35693).
Live-attenuated influenza vaccine is administered via nasal spray. It is approved for ages 2-49 years. It may be preferable in some situations such as vaccinating many persons in a community. It should be avoided if the patient or someone nearby has a suppressed immune system. Hence, it is not suitable for inpatients.
Recombinant vaccine and cell culture vaccine do not contain egg products. They are especially suitable for persons who need to avoid eggs because of allergy or dietary preferences.
Available Vaccines
Universal vaccines that provide durable response against all influenza strains are in human trials (10.1038/s41591-020-1118-7). These vaccines generate antibodies against the viral hemagglutinin protein stem (stalk) domain (HA2). Current vaccines generate antibodies against the immunodominant globular head domain (HA1), which is variable and mutates much more frequently. Vaccines utilizing mRNA are also in human trials. They are likely to have greater efficacy but more side effects than current vaccines. A major advantage of the mRNA vaccines is that they can be readily modified to match mutations in the virus.
Benefits of Vaccination for Adults
Influenza vaccine reduces the risk of respiratory and cardiovascular adverse outcomes and mortality among adults, especially in the presence of pre-existing conditions and advanced age. This was confirmed in a meta-analysis of studies on all adults (10.1016/j.arr.2020.101124). Another meta-analysis found that vaccine reduced the risk of adverse cardiac outcomes, especially in sicker patients (10.1001/jama.2013.279206). Preoperative vaccination is beneficial. A large study of elderly patients who had major surgery found preoperative vaccination reduced by about one-half the risk of pneumonia, intensive care admission, and death (10.1093/infdis/jix616). Patients also had shorter hospital stays and reduced resource utilization.
Influenza Therapeutics
These include neuraminidase inhibitors oseltamivir, zanamivir, peramivir, and laninamivir; cap-dependent endonuclease inhibitor baloxavir; and matrix protein M2 ion channel blockers (10.1001/jamanetworkopen.2021.19151). They attenuate viral replication. They provide postexposure prophylaxis. When started within 2 days of symptom onset, they reduce duration and severity of the disease, and complications. They also reduce transmission of influenza virus. However, their efficacy is limited, especially in patients with serious illness. They are expensive and not widely utilized. Although influenza and COVID-19 have similar initial symptoms, their therapeutics are different. Thus, dexamethasone reduces mortality for hospitalized COVID-19 patients on respiratory support but may increase mortality for hospitalized influenza patients (10.1001/jama.2020.15260).
Influenza Pandemics
They are usually caused by zoonotic influenza A virus strains migrating to humans. The 1918 “Spanish flu” pandemic caused by influenza A H1N1 virus led to more than 40 million deaths worldwide. H1 denotes haemagglutinin subtype 1 and N1 denotes neuraminidase subtype 1. The pandemics of 1957, 1968 and 2009 were caused by influenza A H2N2, H3N2, and H1N1 viruses, respectively. The 2009 “swine flu” influenza A H1N1 virus that originated from pigs was antigenically different from previously dominant influenza A H1N1 viruses. It caused 150,000-600,000 deaths worldwide. Avian influenza “bird flu” caused by H5N1 and H7N9 is not prevalent. Overlapping occurrence of influenza pandemic and COVID-19 will be devastating. Vigilance and prompt action are essential to prevent zoonotic influenza A virus strains from migrating to humans.
Conclusion
Influenza is a prevalent respiratory disease that will continue to affect anesthesia practice in the foreseeable future. With appropriate management, the risk of adverse outcomes is low. Vaccination is highly recommended, especially preoperatively.
For more details : https://jcmimagescasereports.org/author-guidelines/
#US#COVID-19#humans#therapy#appropriately#influenza#prophylaxis#ILI#SARS#anesthesia#laryngospasm#arrhythmias#Uday Jain#jcmicr
1 note
·
View note
Text
What is Prophylaxis?
Dental prophylaxis involves a dentist cleaning the teeth and inspecting the mouth for signs of any dental issues. Prophylaxis means preventive medical treatment. It is a crucial part of looking after the teeth to prevent dental disease and oral health issues.
According to the Centers for Disease Control and Prevention (CDC)Trusted Source, more than 80% of people in the United States will have a cavity by the age of 34 years. Oral health has links to many chronic health conditions, such as heart disease and diabetes, so it is important to practice dental hygiene for teeth and overall health. Read more at https://www.medicalnewstoday.com/articles/what-is-dental-prophylaxis
Check with our dentist in Smile Spa for your expert guidance and help
+91-9895382881
http://smilespa.co.in/
0 notes
Text
I have been thinking about public healthcare, the PrEP (yes, I know it’s a “sensitive subject”) and antimicrobial resistance. And I felt the urge to put some of it into writing - knowing in advance that it may not be the most “PC” thing to do.
I know a person who is not a sex worker but, instead, a very successful self-employed person in the tech field, with the sort of wit I can only dream of. He has more male sex partners than he can actually count, mostly because, given his taste for chemsex parties, he can’t always be sure how many partners he’s had - or whether or not they were protected.
This is a lifestyle choice made by a highly intelligent and successful person, his chosen way to have fun, and he’s free to choose to enjoy life that way.
The welfare state of the country I live in pays for his PrEP. So I, and every other tax payer in this country pay for it.
About a year ago, next to me in a public hospital’s A&E in the country’s capital city, there was an elderly lady with oesophageal cancer who required an urinary catheterisation. It is a painful procedure normally done with lidocaine gel which both lubricates and helps numbing some of the pain. There was no such gel in that A&E. According to the staff, the department had run out of it months before, and there was no budget to buy more. Yet, budget hasn’t run out for my wealthy (and healthy) acquaintance’s PrEP.
Yes, I have read the studies and understood the numbers in the PrEP’s “profitability” projections. There will be (according to the experts) savings in the long run. That is, if we include HIV prevention vs the costs of treating HIV in the equation, and basically nothing else.
That equation, however, seems to forget “human factors”, which we know can be instrumental in producing both miracles and disasters.
Generations have grown up dreading HIV-AIDS. Other STIs are treatable, but not this one. HIV is *THE* STI. To protect ourselves from it, we use condoms, and we don’t stop to think about how many other STIs they help protecting us from. No one truly fears those other STIs - nowhere near as much as we fear HIV, at least.
Here comes the miracle of the PrEP. We are safe from HIV - and HIV is, again, *THE* STI. Remove HIV from our list of worries and sexual freedom increases exponentially. Other STIs are easily treatable - what is a meagre course of antibiotics, after all?
Well, in the great scheme of things, it is a lot, and increasingly so. Everyone has heard terms and expressions like “antimicrobial resistance” or “antibiotic stewardship” but, thankfully (lucky them), not many have come face to face with those terms’ reason for being.
We have used and, sadly, abused antibiotics for decades (we’ve been literally feeding what we once called “magic bullets” to the pigs, for goodness sake!) and, whilst the bugs have been getting used to and, therefore, immune to our “magic bullets”, no new classes thereof have been introduced into the healthcare context recently.
What we see now, are pathogens that once responded well to certain antimicrobial agents no longer doing so - some of them being those behind STIs. Superbugs like MRSA, which were once limited to healthcare facilities, are now popping out of apparently nowhere in the midst of the community. And that’s just one such superbug, many others are out there - and new ones keep showing up - they adapt according to what’s thrown at them, and what we throw at them are antimicrobial agents, such as antibiotics.
Back to the PrEP - the moment we are protected from HIV and start feeling that barrier protections are more “nice to have’s” than anything else, what happens in terms of the myriad of other STIs, some of which many of us have never even hear of? They are overwhelmingly treatable, so that’s precisely what we’ll do: treat them - with antimicrobials - thus exacerbating the major global problem of antimicrobial resistance.
We may say that a few courses of doxycycline is cheaper than a lifetime of integrase, protease, etc inhibitors, and that’s quite true. But once that doxycycline no longer works and we start going for the “heavy machinery” to handle “trivial bugs turned monsters”, can we really say how much that will cost?
And when exposing all sort of pathogens (not only STI-related ones, but everything out there) to that “heavy machinery” starts turning some amongst that virtual infinity of “benign” bugs into superbugs, how much will that cost, both in terms of the financial burden to our NHS’s and in terms of lives?
Everything is connected but, from everything I’ve read over the last year or so, not enough connections seem to have been explored as to allow us to say with any degree of certainly that “the PrEP is cost-effective in the long run”.
Add to that everything that is lacking in our healthcare systems, which our governments, whichever they are, can’t squeeze out of the tax payer to pay for and, from proton beam therapy to the widespread use of viral vectors in cancer immunotherapy (mentioning oncology alone, and there’s a lot beyond it), given that my acquaintance has chosen his lifestyle, but my A&E “neighbour” didn’t choose her cancer, can we really say that the PrEP should be our budget priority?
Up to each individual to come up with their own answer to this question - which is not being asked anywhere near often enough.
#prophylaxis#hiv/aids#hiv prep#antibiotic resistance#antibiotics#public health#healthcare#priorities#hard questions#perspective
0 notes
Text
The Role of Prophylactic Antibiotics in Laparoscopic Cholecystectomy
Abstract
The inappropriate or excess use of antibiotics is one of the biggest current threats to global health and there is therefore a drive to minimse antibiotic use including for prophylaxis. Perioperative antimicrobial prophylaxis is administered prior to surgical procedures to prevent surgical site infections.
Read More About This Article : https://irispublishers.com/ajgh/fulltext/the-role-of-prophylactic-antibiotics-in-laparoscopic-cholecystectomy.ID.000519.php
Read More Iris Publishers Google Scholar Article: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=Wws4PocAAAAJ&cstart=20&pagesize=80&citation_for_view=Wws4PocAAAAJ:MXK_kJrjxJIC
0 notes
Photo

Visite de routine pour garder votre bouche en santé. #dentalphotography #dentalroutinecheckup #dentalroutine #prophylaxis #fypge #dentalcare (at Delmas, Ouest) https://www.instagram.com/p/CgZ84_zpcyv/?igshid=NGJjMDIxMWI=
0 notes
Link
“If this can inform and help, this is why I share. This is xxxxx’s recent sharing to a group of us as we bantered on BA.5 and masks and steps to reduce risk from this more infectious sub-variant given the COVID vaccine has failed, it is junk. Any protection wanes near immediate and you are now on a booster treadmill and will never get off.
Start here:
‘There is such a high % of people that don't understand that this is much different, and also that surgical masks are useless, but so far there is not much risk to healthy under age 60.
Of course the MSM and Democrats and Govt. want us to continue to be afraid.
I don't know the best treatment protocol, but if at risk, you can't go wrong with daily diluted Iodine mouthwash (povidone-iodine), along with nasal application (either via fine sprayer or Q-tips).
3 tablespoons of 10% povidone-iodine in one liter of clear mouthwash, is an 18 fold dilution, resulting in a 0.45% P-I solution (consistent with effective studies.).
Of course upon first symptoms, or suspected exposure, increase above multiple times daily.
Due to the rapid replication, it makes even more sense than ever to begin taking 200 mg hydroxychloroquine daily (or dose of ivermectin), beginning with the first suspected symptoms (fatigue, headache, fever) even before the coughing/phlegm begin. Of course always have Mucinex DM around, to reduce the inconvenience of excessive coughing and phlegm.
If there is more evidence that replication goes to lungs, should have 250 mgs Azithromycin (antibiotic) around.’”
1 note
·
View note
Text
“Syndrome of Contractures and Deformities” According to Prof. Hans Mau as the Primary Cause of Hip, Neck, Shank and Spine Deformities in Babies, Youth and Adults | Chapter 15 | New Horizons in Medicine and Medical Research Vol. 8
The Syndrome of Contractures and Deformities (SofCD) is thought to be the result of abnormalities in the locomotor system in children, as well as inadequacy and pain in adults. Prof. Hans Mau claims that there is a list of symptoms that can be seen in neonates and babies. He refers to this condition as the "Seven Contracture Syndrome" (or "Siebenersyndrom" in German). The authors describe the eighth abnormality, namely the varus deformity of shanks, in this publication from 2006. The Syndrome of Contractures and Deformities, as the primary cause of wry neck (torticollis) and one of the four causes of Blount disease, is thoroughly discussed in this article, as well as its impact on the development of hip dysplasia. In addition, the biomechanical origin of so-called idiopathic scoliosis is explained.
Author(S) Details
Karski Tomasz
Vincent Pol University in Lublin, Poland.
Karski Jacek
Medical University in Lublin, Poland.
Pyrc Jaroslaw
Department of Trauma and Orthopedic Surgery, Hospital Radebeul Elblandklinikum Radebeul, Saxony, Germany.
View Book:- https://stm.bookpi.org/NHMMR-V8/article/view/6653
#Contracture#incorrect position of the body#influence on the neck#spine#hips and shank#therapy#prophylaxis
1 note
·
View note
Text
Prophylaxis Masterlist

Status: Completed
Pairing: Wanda Maximoff x Female Reader
Summary: The most powerful Avenger is afraid of one thing: dental appointments, or the one where you're a dentist and Wanda is a baby about seeing one
Tags: Fluff, Humor
Total word count so far: 12.2k+
Parts: prophylaxis | the follow up | it's just dinner | loving an avenger
Main Masterlist
200 notes
·
View notes
Text
On the other hand I've had maybe one migraine a month since we raised my T dose and I've been having daily to weekly-at-absolute-minimum migraines since I was five or six years old. It's fucking insane that hormones can do that
#Keep joking that I transed my gender like 50% as chronic migraine prophylaxis#I have trialed almost every migraine treatment on the market and aside from 500 mg Topamax nothing has helped like#Fucking. Exogenous testosterone
24 notes
·
View notes
Photo

i gotta revive my dead tumblr wit art lol
idk how tags work and i never will B)))))
Art for ~ Prophylaxis on quotev ~
#corpse party#oc#ocart#art#anime#digital art#pixelated#myart#oc stuff#lunaria#lunariamv#prophylaxis stuff
8 notes
·
View notes
Text
MAMAMOO IN SG
- Yong is obsessed with STEADY BOMBIBI
- Byul keeps yelling out SHIOK SHIOK and sang “Singapura… Oh Singapura…”, the song they learnt while they did their fanmeet in 2019
- Wheein and Hyejin kept laughing at Moonsun’s attempt to talk singaporean slang lmao
- Hyejin said she didnt expect the seats to be filled and said our energy was really great
- Third floor aka my area was the loudest according to mamamoo and gave us a group heart (which we couldnt take photos bcs security)
this was my attempt to be sneaky and take a blurry ass photo
- Yong did something (i forgot what) and Byul yelled “YOURE CRAZYYY” and then messed up her part during Taller Than You. Bij blamed it on Yong and yelled “YOURE CRAZYYYY” again. She tried to go to Wheein and play with her but Wheein acted like she didnt know Byul. #shedeservesit
- Moomooshin-nim made a comeback but she was shy uwu
- Hyejin was being a sweetheart and sat down at the edge of the stage and looked at all the moos at Cat 1 🥹🥹
- Everyone was so hyped during LIEC with their moobongs, even moos were hyped and screamed with them
- Byul was shielding her eyes from the spotlight and looked up while waving, idk where she was looking but i tried waving and she waved back. i waved faster and she waved faster too. im just gonna assume she was looking at me 🥹 me, you, we both cant see each other clearly 🥹🥹
- we had a fanevent where everyone was holding up a banner. mamamoo loved it and wanted to take a photo. they squat down and was ready to pose when solar asked “wait whos gonna take our photo” 🤣🤣
- byul went to kiss a towel, went to each member and asked them to kiss, swung it and threw it pretty far. i think that lucky fan got out of their seat and caught it. (if i got the towel, my mum would probably wash it and i would most definitely cry)
- Byul closed by saying “SHIOK SHIOK I LOVE YOU DEEP DEEP DEDEDEDEEEPPP”
all that i can remember from todays concert. ily mamamoo i wanna see you up close. my old ageing eyes didnt do me justice, i wanted to see you guys in hd 4k resolution 😭
#anyways the concert was a solid 3hours#managed to catch the last train but i got to walk home afterwards 🫠#took painkillers for migraine prophylaxis but ended up with a gastric even tho i ate and took some gastric pills too#BUT FOR MAMAMOO EVERYTHING IS WORTH IT#got macdonalds after concert huehue#mamamoo#solar#moonbyul#wheein#hwasa#myconinsg
8 notes
·
View notes
Last Seen Blogs

archaalen
Untitled On Purpose

staraxi
Hello!
iconic-times
✨Iconic Times✨

wunder-kin
I swing both ways. Violently. With an axe.

sapphiredragonprincess
A Dragon's Palace