#not following CDC guidance
Note
Just curious. How bad has Biden been at controlling COVID-19 in your view?
First: I already responded to a similar question you left on this post.
Second: Biden has been atrocious for COVID-19 safety and management. COVID-19 is still killing people, and our president has done a horribly insufficient job in mitigating that. "Better than the Republicans" is not the same thing as "good" or "effective." Biden's abysmal reaction to COVID-19 is part of why I'm so thrilled that the Uncommitted campaign for the Democratic primary has achieved some success. That particular campaign is focused on ceasefire in Palestine, but the People's CDC explained in a statement how Palestine is also very much a public health issue. We need to scare the bastard and actually do some of that "pushing him left" that people claimed they'd do after getting him elected. Though it seems to me like a lot of people just settled for, "okay, we got rid of Trump, we don't have to worry anymore."
Third: While I'm at it, people have to do more than vote. You have got to get involved. You have got to do more than participate in the presidential election once every four years. Join a union (may I recommend the IWW?), follow the guidance of The People's CDC, volunteer for your local Food Not Bombs, get involved in a tenants union like the Autonomous Tenants Union Network, read Riot Medicine, get trained in first aid and get involved in a street medic group, read up on your local politics and get involved on the small-scale, do something in addition to voting in the presidential election. Even if you're limited in how much you can personally participate, find the people who are talking about these issues and signal boost them, and share the information with others who may be more able to participate more. If you can tell people to go vote in the presidential election, you can also tell them to go do other things, too.
Now, with all of that out of the way, here are some links related to Biden's abysmal COVID-19 response:
During his 2020 campaign, Biden promised immediate $2K stimulus checks. Instead, he delivered $1,400. Sources: [x] [x] [x] [x] [x]
Velena Jones for NBC Bay Area: "‘Too expensive': Bay Area residents shocked over new COVID vaccine prices"
Reuters: "COVID vaccine manufacturers set list price between $120-$130 per dose"
Joseph Choi for The Hill: "Free COVID-19 test program to be suspended for now"
Disability activist Alice Wong writing for TeenVogue: "Covid Isn't Going Anywhere. Masking Up Could Save My Life," and the follow-up article, "COVID and the 2024 Election: What Biden and Democrats Owe High-Risk People."
Laura Weiss writing for The New Republic: "Democrats Can't Keep Ignoring Covid in 2024."
David Cohen and Adam Cancryn for Politico: "Biden on '60 Minutes': 'The Pandemic is Over.'"
Alex Skopic for Current Affairs: "COVID-19 is Still a Threat. So is Biden’s CDC."
Adam Cancryn for Politico: "Biden Appears to be Over Covid Protocols."
Paul Thornton for the Los Angeles Times: "Covid Still Rages, and the Biden Administration Isn't Helping."
Eric J. Topol for the Los Angeles Times: "The U.S. is facing the biggest COVID wave since Omicron. Why are we still playing make-believe?"
We should have free, universal testing. We should have free, universal vaccination. We should have free, universal treatment. We should have financial assistance for those of us who can't work outside the home. We should have mandated work-from-home for any job that can be done remotely. We should be emptying prisons and paying attention to the way disease and abuse proliferate inside their walls. We should have COVID-19 safety PSAs and government support for universal masking. We should have free distribution of N95s. We should have mandated masking in medical settings and public spaces. We should have a higher minimum wage. We should have healthcare reforms. We should have strong worker protections. We should have improved infrastructure. We should have a president who gives a single flying fuck about how many of us are dying.
And we have none of it.
But we sure seem to have money to keep dropping bombs, arming cops, terrorizing the vulnerable, and imprisoning innocent people to use for slave labor.
145 notes
·
View notes
Text
If there is one reason COVID is spreading far and wide it is because people are not testing and not taking cold symptoms seriously, and they are not isolating and following isolation rules. After 5 days of isolation you need to wear a mask for at least another 5 days if you go in public wear an N95 or other respirator.
40 notes
·
View notes
Text
"It’s interesting how often people cite “CDC guidance” as their reason for unmasking. Although the CDC has absolutely participated in and cosigned the mainstream minimizing of the illness, even the CDC still acknowledges that vulnerable people are at risk from COVID infection. They simply encourage the public to let those people die.
During an interview with the BBC in the fall, Dr. Fauci famously said aloud “You’ll find the vulnerable will fall by the wayside. They’ll get infected, they’ll get hospitalized, and some will die.” Should he have characterized any other vulnerable group this way (“You’ll find Native people will fall by the wayside,” “You’ll find trans people will fall by the wayside,” “You’ll find Black people will fall by the wayside,” “You’ll find women will fall by the wayside”) there would surely have been an almighty backlash. But to say medically vulnerable people must die so the rest of us may have brunch indoors does not beget such a reaction- never mind that all the above-named groups- Native people, trans people, Black people and women- are at a higher risk for Long COVID, and other poor outcomes from COVID."
...
"The move to frame the requirement of a public safety measure- no different from requiring seatbelts, helmets, pants and shoes in public- as a violation of bodily autonomy came directly from groups like the Atlas Network, which, as you might gather from its Ayn-Rand-worshipping name, opposes all public regulation. Meanwhile, we continue to violate the bodily autonomy of disabled people by making participation in public life contingent on accepting forcible, continual reinfections.
Since Biden’s COVID normalization campaign, MAGA-style rhetoric about how disabled people should “stay home forever” and how they are “useless” and “weak” has absolutely infiltrated left spaces. Many disabled people, in fact, are effectively “staying home forever.” They are shielding themselves from a disease that may kill them, and certainly would likely lower their baseline health, and have been for years. Meanwhile, the pleas of these incredibly isolated people for the bare minimum of solidarity- please at least mask up indoors when not eating or drinking- are ignored because that is apparently too difficult for the mental health of abled people."
...
"A last point I will address, I did see questions about how we are supposed to “force” people to mask. Disabled people, vulnerable people, and left groups generally do not have the power of the state. We are not going to be engaging in “policing,” because nobody is going to end up in jail, physically hurt, on probation, or with limited job prospects because of our community care. Simply write “masks required” on your event invites, distribute masks wherever possible (contact your local Mask Bloc!), and do your best to spread information while modeling good praxis by masking yourself. For the most part, people are following the crowd. They will do what the majority is doing, and many will be happy to mask if it is normalized instead of stigmatized.
A left that purges its spaces of everyone who values community care, everyone who is willing to experience a minor inconvenience for the well-being of another, everyone who thinks it’s all of us or none of us, is a drastically weakened left. A left that does not incorporate disability praxis is drastically limiting its own scope and ability to be effectual. A left that mocks vulnerable groups and seeks to justify harm to them is not grounded in real justice and has only a superficial understanding of its own aims. Join us in masking, keep your comrades safe, and relish the beauty of avoiding illness while knowing you did your part to protect others. It’s a good feeling at the end of the day, I promise you that."
#covid#eugenics#ableism#genocide#genocide joe#blue maga#anticapitalism#antifascism#antizionism#wear a mask#anarchism#every single unmasked adult in public deserves to be treated as the fascist eugenicist they are#if you think you're radical but you're not masking then your radicalism includes eugenics and that just makes you a goddamn nazi#you will never halt one genocide by carrying out another genocide
26 notes
·
View notes
Text
The stance by the Centers for Disease Control and Prevention (CDC) on face masks has taken many twists and turns throughout the COVID pandemic.
After initially claiming face coverings weren’t necessary, the CDC changed course in April 2020, calling on all Americans — even children as young as 2 years old — to mask up.
That September, then-CDC Director Dr. Robert Redfield said during a Senate hearing that “face masks are the most important powerful health tool we have,” even suggesting that they might offer more protection than vaccines.
Those recommendations likely played a large part in 39 U.S. states eventually enacting mask mandates.
Now, a new scientific review — led by 12 researchers from esteemed universities around the world — suggests that widespread masking may have done little to nothing to curb the transmission of COVID-19.
Published by Cochrane Library, the review dug into the findings of 78 randomized controlled trials to determine whether “physical interventions” — including face masks and hand-washing — lessened the spread of respiratory viruses.
When comparing the use of medical/surgical masks to wearing no masks, the review found that “wearing a mask may make little to no difference in how many people caught a flu-like illness/COVID-like illness (nine studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (six studies; 13,919 people).”
Next, the review compared medical/surgical masks to N95 respirators (or P2 respirators, which are used in Europe).
It found that “wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (five studies; 8407 people); and may make little to no difference in how many people catch a flu-like illness (five studies; 8407 people), or respiratory illness (three studies; 7799 people).”
The 78 studies looked at participants from countries of all income levels.
Data was gathered during the H1N1 flu pandemic in 2009, non-epidemic flu seasons, epidemic flu seasons up to 2016 and the COVID-19 pandemic, the study authors wrote.
Doctor says review had some key limitations
The new findings seem to call into question the CDC’s enthusiastic embrace of widespread masking.
However, Dr. Marc Siegel, professor of medicine at NYU Langone Medical Center and a Fox News medical contributor, pointed out a key limitation: “The researchers focus primarily on randomized trials, but most of the studies that have been done on masks are population studies,” he said.
“There are very few randomized trials on masks.”
In a randomized trial, researchers place participants in different groups and observe the results in a controlled environment.
By contrast, population-based studies measure outcomes in a “real-world” setting.
The study authors did admit to some limitations and a risk of bias, including the low number of people who followed mask guidance and the wide variation of outcomes.
“The results might change when further evidence becomes available,” they wrote.
‘Be sure of consistency’
Dr. Siegel said he has never supported mask mandates.
He believes that while masks might be effective on an individual level, they don’t work as well on a population level.
“If you’re going to mandate something, you’d have to be sure of consistency across the population, and that’s never happened,” he said.
However, the physician pointed out that the CDC never actually mandated masks — with the exception of a public transportation mandate in January 2021.
“It was the state and local authorities that took the CDC’s recommendations and implemented the mandates,” Dr. Siegel said.
“The recommendations may have been wrong, but the CDC doesn’t deserve the blame for everything. I think they were aware that masks may have value on a personal basis, but they got carried away with the politics.”
What do you think? Post a comment.
As of right now, no U.S. states have mask mandates in place.
On Sunday, New York dropped its state-wide mask requirement in hospitals — leaving the decision up to individual facilities. Many healthcare facilities are currently still requiring them.
258 notes
·
View notes
Text
For the sake of guidance, I hope people will follow the highest precautions possible. The worst of SARS-CoV-2 is not limited to 2020, despite what is stated by politicians, media outlets and other public figures and professionals to whom it applies.
I want to inform readers the CDC has officially ended the 5 day isolation period for SARS-CoV-2 and this does not suddenly mean it is not contagious or that our protocols should be lapsed or relaxed. Spread is more rampant than ever. So please do not let this announcement and decision give a false sense of security.
Piece by the incredible Lucky Tran.
Note, please do not use the Washington Post as a source for quality coverage of the ongoing pandemic.
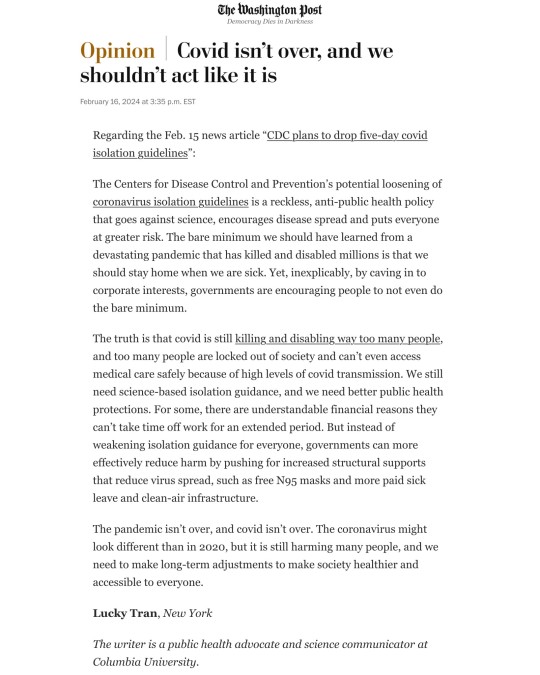
As others have said, if SARS-CoV-2 cannot be eradicated (I still hold out hope and think it imperative in fact), it means adjusting and adapting, not ignoring it, treating this virus and disease as harmless or of little harm and create hostile untenable conditions and daily situations for any efforts of prevention and control of it.
Of what I've read over the course of 4 years, SARS-CoV-2 continues to mutate, kill and disable. This cannot last and will end in an ever escalating disaster if we continue to allow it. - Admin and mod
Additional: Immunity rates are a concern as are vaccination rates. The boast of vaccines administered does not often enough include a breakdown based on how many in the series per person (e.g. 1 dose, primary series, x number of boosters and how recently).
Vaccine rates vary by country, but in regard to the U.S. rates have been on a decline, thus compromising effectiveness on a population level.
#Updates#News#Admin#Moderator#Public health#SARS-CoV-2#Covid-19#Covid 19#SARS CoV 2#SARS 2#Pandemic#Ongoing pandemic#Lucky Tran
5 notes
·
View notes
Text
the CDC just deleted their Covid isolation policy because “no one is following the guidelines anyways” and their goal is to conflate Covid with flu and RSV, but then they literally admit that they expect people to hear this and think Covid is completely over.
i swear these fuckers are living in lala-land if they think people follow their guidance at all. half the country was actively against their guidance from the start, and now NO ONE gives a flying fuck anymore and it shows that people NEED to be told what to do in terms of public health, even things to save themselves and others. people most often are too distracted and misinformed to think critically on their own.
CDC saying shit like “we urge everyone to stay home if they feel sick” and “we urge companies to let their employees stay home if they’re sick” — HOW ASININE
the CDC is essentially saying “thoughts and prayers everyone!!” while admitting using their own downplayed metrics (that omit comorbidities!) that over 1,000 people die and 19,000 are hospitalized every week from Covid in the US
6 notes
·
View notes
Text
From the report by Beth Mole, posted 29 Feb 2024:
In a lengthy background document, the agency laid out its rationale for consolidating COVID-19 guidance into general guidance for respiratory viruses—including influenza, RSV, adenoviruses, rhinoviruses, enteroviruses, and others, though specifically not measles. The agency also noted the guidance does not apply to health care settings and outbreak scenarios.
"COVID-19 remains an important public health threat, but it is no longer the emergency that it once was, and its health impacts increasingly resemble those of other respiratory viral illnesses, including influenza and RSV," the agency wrote.
The most notable change in the new guidance is the previously reported decision to no longer recommend a minimum five-day isolation period for those infected with the pandemic coronavirus, SARS-CoV-2. Instead, the new isolation guidance is based on symptoms, which matches long-standing isolation guidance for other respiratory viruses, including influenza.
"The updated Respiratory Virus Guidance recommends people with respiratory virus symptoms that are not better explained by another cause stay home and away from others until at least 24 hours after both resolution of fever AND overall symptom are getting better," the document states. "This recommendation addresses the period of greatest infectiousness and highest viral load for most people, which is typically in the first few days of illness and when symptoms, including fever, are worst."
The CDC acknowledged that the eased isolation guidance will create "residual risk of SARS-CoV-2 transmission," and that most people are no longer infectious only after 8 to 10 days. As such, the agency urged people to follow additional interventions—including masking, testing, distancing, hygiene, and improving air quality—for five additional days after their isolation period.
"Today’s announcement reflects the progress we have made in protecting against severe illness from COVID-19," CDC Director Dr. Mandy Cohen said in a statement. "However, we still must use the commonsense solutions we know work to protect ourselves and others from serious illness from respiratory viruses—this includes vaccination, treatment, and staying home when we get sick."
Overall, the agency argued that a shorter isolation period would be inconsequential. Other countries and states that have similarly abandoned fixed isolation times did not see jumps in COVID-19 emergency department visits or hospitalizations, the CDC pointed out. And most people who have COVID-19 don't know they have it anyway, making COVID-19-specific guidance moot, the agency argued.
In a recent CDC survey, less than half of people said they would test for SARS-CoV-2 if they had a cough or cold symptoms, and less than 10 percent said they would go to a pharmacy or health care provider to get tested. Meanwhile, "The overall sensitivity of COVID-19 antigen tests is relatively low and even lower in individuals with only mild symptoms," the agency said.
The CDC also raised practical concerns for isolation, including a lack of paid sick leave for many, social isolation, and "societal costs."
The points are likely to land poorly with critics.
“The CDC is again prioritizing short-term business interests over our health by caving to employer pressure on COVID guidelines. This is a pattern we’ve seen throughout the pandemic,” Lara Jirmanus, Clinical Instructor of Medicine at Harvard Medical School, said in a press release last month after the news first broke of the CDC's planned isolation update. Jirmanus is a member of the People's CDC, a group that advocates for more aggressive COVID-19 policies, which put out the press release.
Another member of the group, Sam Friedman, a professor of population health at NYU Grossman School of Medicine, also blasted the CDC's stance last month. The guidance will "make workplaces and public spaces even more unsafe for everyone, particularly for people who are high-risk for COVID complications," he said.
But, the CDC argues that the threat of COVID-19 is fading. Hospitalizations, deaths, prevalence of long COVID, and COVID-19 complications in children (MIS-C) are all down.
COVID-19 vaccines are safe and effective at preventing severe disease, death, and to some extent, long COVID—we just need more people to get them.
Over 95% of adults hospitalized with COVID-19 in the 2023–2024 respiratory season had no record of receiving the seasonal booster dose, the agency noted.
Only 22% of adults got the latest shot, including only 42% of people ages 65 and older. In contrast, 48% of adults got the latest flu shot, including 73% of people ages 65 and older. But even with the crummy vaccination rates for COVID-19, a mix of past infection and shots have led to a substantial protection in the overall population.
The CDC even went as far as arguing that COVID-19 deaths have fallen to a level that is similar to what's seen with flu. "Reported deaths involving COVID-19 are several-fold greater than those reported to involve influenza and RSV. However, influenza and likely RSV are often underreported as causes of death," the CDC said.
In the 2022–2023 respiratory virus season, there were nearly 90,000 reported COVID-19 deaths.
For flu, there were 9,559 reported deaths, but the CDC estimates the true number to be between 18,000 and 97,000.
In the current season, there have been 32,949 reported COVID-19 deaths to date and 5,854 reported flu deaths, but the agency estimates the real flu deaths are between 17,000 and 50,000.
"Total COVID-19 deaths, accounting for underreporting, are likely to be higher than, but of the same order of magnitude as, total influenza deaths," the agency concluded.
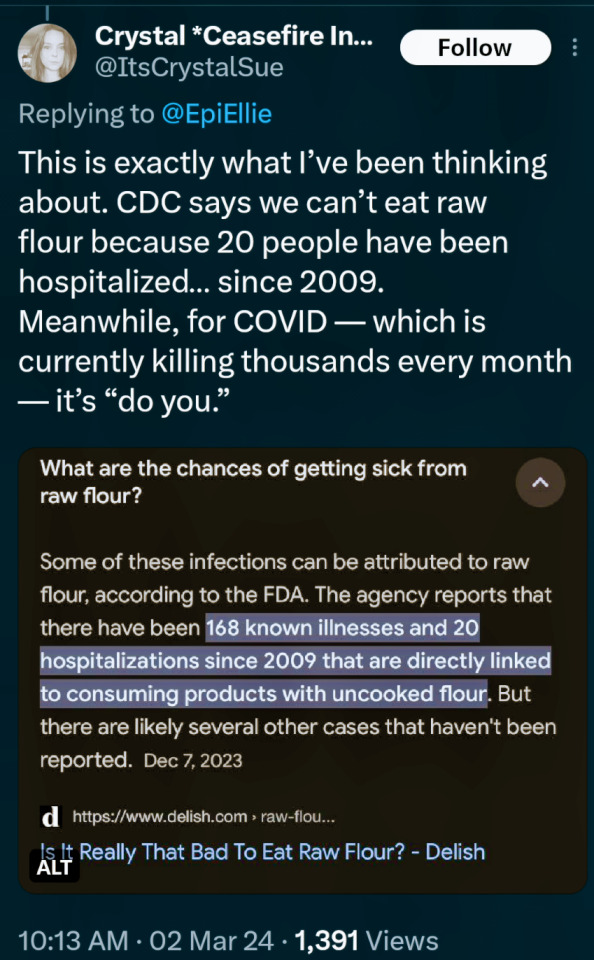
(say no to raw dough: CDC)
#please stay safe#the vaccines are safe#yes the covid shot is safe#covid is not a hoax#covid causes permanent long term damage to your body even if you're healthy#news#scicomm#science#ars technica#covid--19#coronavirus#beth mole#pandemic#the cdc#centers for disease control#5 day covid isolation#yes you should stay home for at least 5 days if you test positive for covid#Open windows to ventilate indoor space with outdoor air to prevent virus transmission#Wear a mask that doesn't touch your lips#keep distance from others
5 notes
·
View notes
Text
"...The planned HICPAC revisions would water down infection control protections, particularly for aerosol transmission and multidrug-resistant organisms.
Most immediately worrisome is its conclusion that plain surgical masks (aka “baggy blues”) are equivalent to N95s and provide adequate protection to healthcare workers and patients. There is abundant evidence to the contrary. This from the CDC:
[Graphic showing that N95s lower odds of getting covid]
It is clear that N95s offer far better protection against aerosols, such as from Covid-19 and other inhaled pathogens.
More than 900 experts in infectious disease, public health, industrial hygiene, aerosol science and ventilation engineering signed a letter to Mandy Cohen, M.D., the new CDC director, explaining how the new draft guidelines weaken protections for healthcare workers. They state, “Surgical masks cannot be recommended to protect health care personnel against inhalation of infectious aerosols.”
The experts’ letter was coauthored by Lisa Brosseau, Jane Thomason and Peg Seminario, among others. Seminario was the director of occupational safety and health for the AFL-CIO from 1990 to 2019.
The CDC responded to Seminario and the experts’ letter only now, a month later, and just before the scheduled Aug 22 meeting. The agency offered no substantive or specific rebuttal, but spoke of its dedication to “improving healthcare quality” and commitment to “to transparency, communication, and stakeholder engagement.” It also claimed that the CDC is meeting the guidelines for transparency required by the Federal Advisory Committees Act. The letter is not yet publicly available.
HICPAC’s proposals also fail to include ventilation, UV disinfection and HEPA filtration, all essential tools against an airborne pathogen.
There are many concerns regarding HICPAC’s process, as well.
Meetings did not include experts in aerosol transmission, ventilation, occupational health and worker protections, Occupational Safety and Health Administration (part of the Department of Labor), National Institute of Occupational Safety and Health (part of CDC which researches worker health and safety) or representatives of healthcare workers.
Lisa Brosseau, an expert on respiratory protection from infections at the Center for Infectious Disease Research and Policy and a retired professor, expressed outrage at HICPAC’s process: “Why are they not consulting with all the people and all the stakeholders? They are not, and that's a sort of basic expectation of a federal advisory committee.”
Brosseau was equally critical of the committee’s literature review, saying that it was “cherrypicked” and “the most ridiculous literature review I've ever seen.” She concluded, “I think they were hoping nobody would notice” how the review was manipulated.
While HICPAC suddenly (Aug 15–a week before its scheduled meeting) invited public participation, it has not provided meeting notes, minutes, transcripts or a draft policy beyond its bullet point slides.
Thomason said HICPAC is “weakening existing guidance for infection control and not following the science that has been built over the last several decades about aerosol transmission.” She added that, in their goal of providing more flexibility, “They said to employers, ‘Here are the minimal standards, and you guys figure out what you need and want to do.’” They are proposing minimal crisis standards of care.
Brosseau added, “Being in health and safety, I know where that goes. It means you get nothing, workers get nothing, no protections. You don’t leave it to the employer to make decisions about workplace hazards.”"
More in the article:
8 notes
·
View notes
Text
I’m very grateful for the online chronic illness community and feel it can and does make a positive contribution
---
I was recently asked to submit some comments about my experiences of using the Internet as somebody with an energy-limiting chronic illness. As I was one of many people who were contacted for this article, “Spoonies: who we are and how to be an ally” https://chronicfeminist.uk/2022/09/17/spoonies-who-we-are-and-how-to-be-an-ally/ not all my comments were used so I thought I would share them in this mini blog. This of course is not a comprehensive exposition of the topic.
---
I have been severely affected (housebound with dozens of debilitating symptoms) with Myalgic Encephalomyelitis (sometimes known as Chronic Fatigue Syndrome, or ME/CFS) since all the way back to 1994. In 1995, I joined my first online forum in 1995 (CFS-L/alt.med.cfs) and ever since I’ve been a regular contributor to online ME/CFS and chronic illness forums and more recently social media.
My energy-limiting chronic illness/spoonie condition means I’ve never actually attended an in-person support group in all those years so it’s been great to have access to all the online discussions.
One of the things I’m most proud of is highlighting how graded activity/exercise programmes may not just help but can sometimes cause harm in ME/CFS. I wish someone had warned me of this as it might have prevented much of my disability. I initially became ill in 1989 as a sports-mad 16-year-old after contracting a viral infection; I wasn’t diagnosed until age 22: I blame the late diagnosis and the advice to exercise as causing my illness to deteriorate drastically as for the first few years I was only mildly affected and in full-time education.
Unlike pharmaceuticals, non-pharmacological interventions like exercise programs are not highly regulated. The harm many of us had suffered from exercise programs was not being picked up. I and others were able to use online media to warn others including in recent years those with similar symptoms following Covid (i.e. a subgroup of those with Long Covid). I would like to think this has prevented some people’s health deteriorating.
I was so frustrated by the medical profession ignoring the fact that graded activity programs for ME/CFS very often didn’t work and sometimes caused harm that I eventually devoted a lot of my free time and energy writing to peer-reviewed journals (see: https://www.researchgate.net/profile/Tom-Kindlon/research ). I teamed up with others I met online on many occasions. In recent years, national guidance in the field from bodies like NICE and the CDC has changed with graded exercise programs no longer being recommended and I believe what I and others I worked with online helped bring about these changes.
Both the internet and myself have changed over the years. Initially I was in some groups for young people who were ill but passing 50 last month, I can no longer be seen as young by any definition. Saying that, I’m still dependent on my parents who do all the chores for me in the family home, freeing me to use my limited energy in ways I find most meaningful. Apart from family life and some limited contact with old friends, most of my contact with the outside world is online. The internet has been a godsend in enabling me to connect with others with similar experiences and challenges in a way that doesn’t drain my energy stores too much. Also, now photos and videos can be shared enhancing the experience in comparison to the 1990s when everything was in text form. Throughout history, some have claimed the latest technologies would cause major harm in weird and wonderful ways we would now consider ridiculous and I think that’s how people should consider claims that it is somehow harmful for people with energy-limiting chronic illnesses to use the internet to discuss their challenges and reach out to others in similar circumstances.
29 notes
·
View notes
Text
I'd love to share with you all my undergrad honors thesis! Warning, it's a long read but well worth it, especially if you're into harm reduction
Why do Chronic Pain Patients Use Opioids Outside of the Realm of Prescription?
December 21, 2022
Nadiya
With the guidance of mentors David Frank, PhD and Noa Krawczyk, PhD
Macaulay Honors College Public Health Honors Project
AbstractThis exploratory review aims to summarize the reasons why chronic pain patients have been using opioids not as prescribed. Review and analysis of Reddit posts revealed people’s reasons for not using drugs as prescribed, and yielded meaningful anecdotes about their stories. Results showed four overall themes, with one theme being patients not getting enough supply, either through underprescription, no prescription, or getting cut off prescriptions; one theme being issues with withdrawal, often linked to lack of information or various reasons for patients to DIY the process; one theme being blocked communication between doctors and patients, specifically focusing on stigma in the medical community against drug users; and the last theme focusing on the negative effect of national, state, and practice-based prescription guidelines. These can be summarized by one overarching theme of disconnect between patients and doctors. Recommendations can be made to improve guidelines and to train doctors better.
Background/Introduction/LiteratureThe use of opium as an analgesic can be traced back to the times of ancient Sumer, with references to it written on a clay tablet of medical preparations (Norn et al., 2005). Since then, opium and increasingly stronger opioids, including synthetic opioids, have been used in a widespread manner, primarily for pain management and for recreational use, as opioid euphoric properties hold similar levels of power as analgesic properties (Norn et al., 2005). Although there had been previous opioid “epidemics” such as the high level of Opioid Use Disorder following the Civil War, the most currently thought of opioid “epidemic” is the one that occurred in the late 1990s and early 2000s, whose dangerous aftereffects we are seeing today with the advent of fentanyl (Jones et al., 2018). A perfect storm of the medical institution starting to briefly acknowledge the importance of pain and the invention and widespread marketing of preparations like OxyContin, as well as the willingness of many physicians to prescribe of opioids, caused an increase in the rates of opioid use, unfortunately leading to dependence and overdose in some cases (Jones et al., 2018). These negative consequences caused a shift in the pendulum in the complete other direction, with more crackdown on prescribing doctors, crackdown on users, and low rates of prescription of opioids (Marchetti et al., 2020). By now, the CDC has put out federal guidelines about opioid prescription for doctors (2016 guidelines dealt with how much opioids can be prescribed and what risk factors can be considered in prescription) (Bohnert et al., 2018). Furthermore, states have set up their own guidelines to try to curb causing dependence (Soelberg et al., 2017). Also, private healthcare companies often have blanket rules or limits that either they won’t prescribe opioids or no more than a limited dose of opioids (Webster & Grabois, 2015). In theory this was to cut down on pill mills, where anyone could claim any injury for a prescription they could get multiple refills of (Kennedy-Hendricks et al., 2016).When reading this paper, it is important to note the different kinds of opioids mentioned.OxyContin, Norco, Lortab, and tramadol are all available by prescription but also on the street; in the US, heroin is only available on the street. Methadone and suboxone are forms of medication-assisted treatment (MAT); suboxone, which was mentioned more often in this research, is a partial opioid agonist which also often includes naloxone, an antagonist, in its preparation to block users from getting high on other opioids (Velander, 2018). Although mostly obtained via prescription, suboxone can be acquired on the street (Hswen et al., 2020). Kratom is a plant with opioid characteristics that while still often used for pain or euphoria, is most frequently associated with assisting with withdrawal symptoms or tapering off stronger opioids (Eastlack et al., 2020). It is not legal in all states or countries, but where it is legal, it is typically sold in headshops or online; it is never prescribed (Prozialeck et al., 2020).Another important concept that received several mentions in patient posts was withdrawal, which requires explanation. After some level of dependence, an opioid user will start developing withdrawal symptoms when they stop using (Kosten & Baxter, 2019). These will worsen over the duration of use (Kosten & Baxter, 2019). Symptoms include an agitated/anxious mental state, insomnia, sweats, chills, flu-like symptoms, cramps, diarrhea, nausea, and vomiting (Kosten & Baxter, 2019).
MethodologyIn this exploratory review and analysis, Reddit posts were analyzed to answer the question of why current chronic pain patients use opioids in an illicit and/or non-prescribed way to manage pain. The social media forum Reddit, through its subreddit r/opiates, was used to sort through posts that might be of relevance. The search term used was “chronic pain.” Inclusion criteria used when considering posts for analysis incorporated posts consisting of at least 5 words in the body, and if there was repeat posting, only first posting in order of the algorithm was counted. Non-prescribed use had to be present or heavily implied in the content of the post. The project defined non-prescribed use as use beyond the scope of a prescription, encompassing everything from using drugs bought on the black market to doubling the dose of a prescription or using non-prescribed supplements. At this point, 50 posts that matched criteria were collected.The posts were coded on Google Sheets using the following list of categories, which were picked after thematic analysis of the topic.Can’t obtain a prescriptionAlready dependent from previous prescriptions or non-prescribed useWant more after prescription but can't getPrescription too lowRan out of prescription earlyRaised toleranceOff label use of prescriptionAre using for recreational reasonsDon’t want to go to a doctorCan't afford a doctor/doctor doesn't take insuranceReceived shared pills from othersWere already using pre-pain,Want the high from a stronger drugAvoidance of dopesickness/withdrawal symptomsUse vs suicideNo illicit use mentioned (still not using as prescribed)On medication-assisted treatmentUse of kratom,Different route of administrationRelief from dopesickness/withdrawal symptomsFear/avoidance of painUsing from non-prescribed supply on top of prescriptionUse of non-opiate drugs mentioned,Doctor lowered/took off scriptNew or worsening chronic pain after withdrawal/abstinence (post-acute withdrawal syndrome)Use of heroin.Each category was given a code and these codes were marked next to posts that pertained to them. Then important quotes were gathered and several themes were identified, some stemming from criteria, and some from analysis.Limitations include the fact that posters could use other terms than “chronic pain” to describe their pain, and the fact that posts were shown in the order of Reddit’s proprietary algorithm. Another limitation is the lack of inclusion of “should I” posts, or posters who haven't yet made the jump but are asking about using their prescriptions in a different way or trying new substances. Another limitation involves the fact that this study does not take into account the people who would not be using Reddit to talk about their experiences, including, notably, many elderly individuals who may be a part of the target demographic.
Results
Quantitative AnalysisOut of 50 data points, here’s how many were counted positive for each category:Category Count
Can’t obtain a prescription 13
Prescription too low 11
Use of heroin 10
Are using for recreational reasons 9
No illicit use mentioned (still not using as prescribed) 9
Using from non-prescribed supply on top of prescription 8
Different route of administration 7
Want more after prescription but can't get 7
Off label use of prescription 6
Use of kratom 6
Use of non-opiate drugs mentioned 5
Raised tolerance 5
On medication-assisted treatment 5
Relief from dopesickness/withdrawal symptoms 5
Ran out of prescription early 4
Fear/avoidance of pain 4
New or worsening chronic pain after withdrawal/abstinence (post-acute withdrawal syndrome) 4
Use vs suicide 3
Doctor lowered/took off script 3
Don’t want to go to a doctor 2
Received shared pills from others 2
Were already using pre-pain 2
Avoidance of dopesickness/withdrawal symptoms 2
Can't afford a doctor/doctor doesn't take insurance 1
Want the high from a stronger drug 1
Already dependent from previous prescriptions or nonprescribed use 0
Qualitative AnalysisAnalysis of the Reddit posts revealed four umbrella themes:1. Patients aren’t getting enough medication to manage pain.2. Patients are dealing with issues related to opioid withdrawal/dependence/tolerance.3. Patients are not consulting with their doctors about their opioid use.4. Guidelines for prescription of opioids are not serving patients well.
Umbrella Theme 1: Patients aren’t getting enough medication to manage pain.Multiple Reddit users found that although they were getting prescriptions, the prescriptions were insufficient to their levels of pain. Some patients feel their doctors aren’t understanding their pain, and are acting out of a fear of overprescription.One poster described their frustration at not being prescribed opioids.“and what got me so pissed off, was when I talked to one of the docs he was saying “we really don’t want to use any narcotics as they’re dangerous and we want to keep you safe, if you have excruciating pain, you can have a small dose of norco once a day.” ”Self-management of pain medication is a strategy many use to allow for their low prescriptions. Here, one patient described using dietary changes to make their dose have a higher effect, in this case using grapefruit juice to potentiate the effects of opioids. (Nieminen et al, 2020)“It's gotten so bad that I've begun to starve myself most of the day and drinking mostly grapefruit juice to have my limited dose hit as hard as possible.” Others, like the next two posters, stretch their limited prescription, finding themselves in a conflict to take multiple doses to alleviate pain versus risking having nothing left to deal with a potential flare-up.“Try to keep it in the 15 - 30mg range per day so I don't max out my script in one week.”“I hate that so far today, I've taken 75mgs of oxy [Oxycontin], yet my back is still screaming at me. I hate that I only have one 15mg pill left, and I'm trying so hard not to take it just yet.”Many users found themselves unable to take prescriptions at all: “cant get doctors to help me for shit have to self medicate.”In some of these cases it is clear that the patients have already sought extensive care but still can’t get a prescription.“There's so much scaremongering about doctors overperscribing (sic) opiates, but I'm out here with a super fucked up back (dont want to get into specifics but its gnarly) and the xrays and MRIS to prove it and i still can't find a doctor to prescribe me anything stronger than naproxen.”“I've had a torn miniscus (sic) tendon for the past 7-8 years and none of the doctors I've been to will do anything about it. Doctors refuse to send me to pain management, their excuse is that I don't need it. I've taken it upon myself to medicate with the only pills that seem to work for it. (Oxy, Lortab)” For at least one patient, only mild or highly improbable solutions have been given.“every single doctor I've been to just gives me shitty NSAIDs and tells me to exercise”In some cases, doctors are cutting patients off their medications. One patient has been told that there is no cure and is therefore scared of being cut off their meds.“I’ve been told this “is it” for me, as after 6 years of treatment/surgeries there’s nothing left to do but treat symptoms, and I’m terrified I’ll be cut off my meds this year, it’s terrifying…..”This patient’s story shows a direct link between being cut off and buying on the black market.“I was prescribed quite a bit of opioids but I was cut off because it was just a general doctor and I had to go to the streets which eventually led me to suboxone [an opioid partial agonist used for withdrawal]”
Umbrella Theme 2: Patients have issues with withdrawal/dependence/tolerance and the way interactions with doctors about these topics have gone.One patient was worried that trying to taper off legally with suboxone would affect other prescriptions, and was crowdsourcing information instead of telling the doctor their fears.“I’ve bought subutex [same as suboxone] before and managed to get myself off it but I can’t get it this time. Would a doctor allow you to be prescribed subs while your already on other opioids prescribed?”Another patient is trying to crowdsource answers to their problem; they started off using legal kratom, but it wasn’t enough for the pain.“Now i tried to just come off morphine and jump on to kratom but my habit is too big and the kratom wasn't holding me plus it wasn't really putting a dent in my pain. I'm so fkn lost, i really don't know what to do at this point this seems insurmountable and i've just been crying all day.”One person feels they made a mistake telling their doctor. There are steep costs associated with suboxone for them, and they consider heroin to be more pleasant and cheaper.“Doctors refuse to help me. Even with my medical history , I made a horrible mistake of going for help in my most desperate moments of withdrawal, tried to get on subs [suboxone, an opioid partial agonist used for withdrawal], But said fuck it when I realized they wanted $16 every single day to dispense me a sub [suboxone] strip 6 days a week with only 1 take home for sundays. My dope [heroin] habit I could maintain on for only a little more money and it felt way better so why the fck would I get on maintenance?”Two patients likely weren’t given enough information about withdrawal. Withdrawal is seen as a “junkie” thing, so doctors don’t want to give their patients the impression they’ll get it (or don’t know much about it themselves), and patients don’t think it will happen to them so they don’t research it. (Rieder, 2017)“Only today it dawned on me what an odd coincidence it is I feel sick when I don't take it but I'm fine when I do. I've been using it continuously for the past couple days and today I woke up feeling like complete shit.”“Now my tolerance is so high I haven’t been taking as directed and taking the max dose. I ran out almost 3 days ago now. I am so tired, my legs and my arms hurt if I don’t move them, have the shits [diarrhea], headache, and all over feeling terrible [typical opioid withdrawal symptoms]. I’m assuming this is withdrawal but I feel so fucking awful.”
Umbrella Theme 3: Patients are not consulting with doctors about pain and opioid use.Patients were often found to be deliberately withholding information from their doctors for various reasons:“Like I said I hid it from my doctors, so I never really got to find out exactly what that pain was”At least one patient was scared that doctors would think they were lying for a prescription.“I tried to hide it from everyone. I was scared that doctors would think I was phishing [committing fraud/lying] for pain pills, and/or that my family would doubt my sobriety because of my behavior.”Rehab facilities often don’t let patients take any psychoactive drugs, and this person was rightfully worried that if she entered rehab, her meds could be taken from her.“She says she can't go to treatment because they'll take her meds for her illness (she collects SSI for her disability) and they could fuck with that as well.”There are often lengthy processes associated with trying to get specialists that put people off.“I've been thinking of trying to get a referral by my regular doctor to the nearest chronic pain center, to see a specialist and psychiatrist for specific pain-related treatment. In this country the doc has to write up my medical history, explain the current condition in a referral letter, mail it to the pain specialist, and if he deems it legit he'll mail me a form to fill to evaluate my pain levels. Which I have to mail back to expect a call back about a first appointment. You can understand that this is so convoluted it doesn't even make me wanna do it.” Doctors are often wary if a patient asks for a specific opiate, thinking they are trying to commit fraud.“As of now I have been to two docs who pushed me aside giving me 800mg Tylenol, it didn't do shit but I remember I had gotten a script of trammadol (sic) for a root canal and it made everything painless and easy but as soon as I said that to the doctor he immediately wrote another 800mg Tylenol script without hesitation and sent me on my way.”Many patients were scared of being marked as addicts due to withdrawal symptoms, other prescriptions, or being honest about recreational drug use. “Doctors see the addict mark on my history and treat me like a piece of garbage.”One patient regrets honesty with their doctor, who won’t prescribe to a heavy drinker. Although alcohol and opioids are synergistic, this patient is still in a lot of pain. (Cushman, 1987)“I went to the doc my sister goes too (sic) and told him about my drinking habits and the pain, he told me he won't prescribe any opiates for "fear of additional addictions" occurring.”Here, the patient knows they are labeled dependent, so they are scared that the “addict mark” will not let them request extra of their prescription.“And when I go in for my next appointment, if I mention that the 10mg dose is preferable do you think I'll run into any trouble for suggesting that now that I have been labelled as dependent?”The patient feels they can’t be honest about illicit use without fear of being cut off from their meds.“If I go to my doctor and come clean that I’m using oxy’s {Oxycontin] and heroin will the (sic) blacklist me from the prescription I’m on?”This poster is worried that coming clean about their opioid usage will cause their psychiatrist to stop giving them benzodiazepines.“I have no intentions of telling my psychiatrist because knowing her, she'd most likely just take away my benzo [benzodiazepine] prescription away and think the problem is solved. I'm almost 100% if I tried telling anyone else I wouldn't get taken seriously either, just like with all my other both physical and mental health issues, and it's not that dangerous of a drug anyway. I don't want to make the situation even worse for myself, like it's always happened before when I mistakenly trusted people, despite it being their job to help me”This poster is worried that if suboxone is on their record, they will be blacklisted from future pain medication prescription and is wanting to try to self-medicate withdrawal with kratom instead.“I’m thinking about using kratom as a substitute for suboxone. I don’t want to take subs [suboxone] because 1. i don’t want my family to know 2. i don’t want that on my health record as i struggle with chronic pain and it would hinder some medical treatment for sure”In this case, a doctor’s beliefs about marijuana use are getting in the way of evidence-based care; the patient has essentially been cut off after admitting to marijuana use and exhibiting vague symptoms.“Now when it comes to my doctor. I feel like the stigma behind my marijuana use has greatly affected my care. He thinks I’m addicted to marijuana which is absolutely ridiculous. I’ve had panic attacks before in the hospital (I’ve dealt with anxiety far longer than I’ve been using marijuana) and he attributes them to “marijuana withdrawals” like wtf. And more recently he’s completely cut out any opiate use in my care. I’ve had multiple times where I have bad chest pain episodes and I need to go to the ER but the only thing they will give is toradol and Tylenol which does jack shit. This has forced me to start going to my local hospital ER whenever I have bad pain cause I know it can be treated there properly then I could be transferred to my normal hospital.”
Umbrella Theme 4: Guidelines for prescribing opioids aren’t serving patients.In this case, the patient is unsure but thinks state or healthcare company regulations are applying a rule that results in insufficient care.“Idk if doctors in California specifically at kaiser [Kaiser Permanente, a healthcare company] can even still prescribe monthly pain meds I don’t care about being high anymore I want this pain to end.”Here, a GP is prescribing an insufficient dose because of fear of crossing guidelines, which could impact their licensure.“My doctor (not pain management doc, normal GP) won't go over 50 MME [morphine milligram equivalents] a day because they're scared of the 2016 CDC Opioid guidelines bullshit.”Many practices have pain contracts, which require opioid-receiving patients to give their word to do certain things to keep getting their prescription (Payne et al., 2010). Here, a patient is scared that because they will have six less than needed if they didn’t use extra, at their next count they or their doctor will get penalized.“My doctor does pill counts now, the amount I’m supposed to be coming in with is 12 and if I’ll only be left with 6, am I gonna be fucked [low counts might look like abuse or dealing]? I’m not abusing them in any way, and I’m scared that I’ll look like I am and fuck up my prescription or get my doctors narcotic license taken away or something. I’ve only failed one drug screening when I wasn’t taking my medication because (TMI sorry) I hadn’t shit in a week.”
Discussion In analysis of these posts, the most common overarching theme was patients feeling disconnected from doctors, from not being able to convey their level of pain and having it met, to being prescribed medications they don’t understand, to not sharing issues with their doctors for fear of judgment or non-prescription.. All four themes — insufficient prescription, withdrawal issues, patients not consulting with doctors, and prescription guidelines — often come down to issues with the medical institution or individual doctors. However, this is such a widespread problem among individual doctors that change must be made on the systemic level, for instance, during education.Insufficient prescription stories in the data can be narrowed down to three categories: patients with prescriptions who experience more pain than their prescription can help, patients who cannot obtain a prescription for opioids, and patients who are cut off from their prescriptions. In all of these sub-categories, there is a common theme of frustration with doctors not meeting patient needs. There is also a theme in the already-prescribed sub-category of using other strategies to make a prescription have more power, some of which are risky. Using other substances to potentiate the drugs, especially benzodiazepines and alcohol, can lead to overdose, and doubling up on doses to then run out can lead to a cycle of withdrawal (Knopf, 2020). In the never-prescribed subcategory, it is becoming clear that many patients who are seeking extensive medical attention are not getting the medications they need. In the cut-off category, getting cut off or tapered down without permission can precipitate withdrawal. In all, this umbrella category shows a pattern of denial of a patient’s agency in their own pain management process, and doctors should find better ways to monitor people’s pain and not assume the least effective methods will do the trick.Multiple issues come up with withdrawal precipitated by running out of opioids and self-precipitated withdrawal due to the desire to taper off. For instance, it is hard to obtain suboxone and when people do, it can be quite expensive (Hswen, 2020). Kratom can also run quite expensive, and oftentimes does not treat withdrawal symptoms effectively (Eastlack et al., 2020). In a lot of cases, patients aren’t able to utilize detox programs because they would have to be free from opiates, but either doctors aren’t providing helpful ways to get patients off opioids, or patients don’t feel comfortable approaching the subject with their doctors (Timko et al., 2016). Additionally, many patients are not adequately educated on withdrawal; it can take a while for them to catch on to the fact that they don’t have a nasty flu, they are instead in withdrawal from the prescribed opiates they take (Kearney et al., 2018). This would imply that in long-term opiate prescriptions, doctors need to do a better job of describing the near-inevitability of withdrawal, the signs and symptoms, and when to seek help.Patients are also often scared to seek help from their doctors, often preferring to seek answers from nonprofessionals on sites such as Reddit instead. There is fear that doctors would think they are lying. This is especially true when patients want to ask for a specific opiate, as this often makes doctors wary (Lagisetty et al., 2019). Instead, self-research about medications should be encouraged and not seen by doctors as grounds for a scam. Additionally, strict rehab policies and lengthy processes to get specialists are turning patients off (Mehrotra et al., 2011). The specialist issue is not unique to pain management, but should still be improved (Mehrotra et al., 2011). Rehabs or other drug treatment centers should also have less all-or-nothing, more harm-reduction centered approaches, especially ones that match the reasons why a person might be taking a specific drug.There is also a heavy stigma against drug users of all kinds in the medical profession (Ahern et al., 2007). Although it can be understood that a provider would be wary to prescribe an opioid to a self-disclosed drinker or benzodiazepine user, as these can cause dangerous combinations, there has to be some way to balance this. Otherwise, we have a system where patients lie to their doctors about their drug and alcohol use and therefore are not properly counseled and can succumb to these consequences. Doctors should take extra care if there is a Substance Use Disorder (SUD), but still prescribe, maybe with mandatory counseling, as more than anyone, people with SUDs can find these drugs on their own. In this system, posters are reporting lying so they won’t be cut off any prescriptions and even withdrawing by themselves so they are not marked as an addict by records.In the wake of the 2000s “opiate epidemic,” doctors were given more stringent prescription guidelines. In many cases, patients aren’t aware whether they are being affected, unless their doctors told them directly, but patients are aware that some great changes have been made, either from their past medical experiences or that of the people they know. Private practices have also instituted blanket rules against prescription, mandatory pain contracts, drug urinalysis, and pill counts, which can lead for one “slip-up” or double dose in a patient’s pain regimen to get them in trouble (Tobin et al., 2016). These policies should be reexamined as they are mostly working just to deter and punish chronic pain patients (Tobin et al., 2016). State and federal guidelines also need to be loosened, as doctors should have more freedom over their prescription choices, making patients’ lives better.
Hope you like this and feel free to share!
#science#social science#research#public health#drugs#harm reduction#opioids#chronic pain#disability#cripple punk#sociology
18 notes
·
View notes
Text

The perfect photo doesn't exi- wait I think we found it.
This summer, we will be featuring previous Get Into Your Sanctuary Photo Contest winners. Enter your best images of people responsibly enjoying national marine sanctuaries, whether they’re surfing, boating, kayaking, diving, swimming, conducting research, or just hanging out on the beach. Photos should be taken following CDC and local guidance. Submit these pics into the “Sanctuary Recreation” category.
Credit: Anna Baker Mikkelsen (2021 1st Place Winner - Sanctuary Recreation)
#ILoveMySanctuary#EarthIsBlue#SaveSpectacular#PhotoContest#Winners#Photography#RecreateResponsibly#Recreation#Tourism#NaturePhotography#LandscapePhotography#Surfing
38 notes
·
View notes
Text
Please be aware, data not being collected does not mean there is no data. Reach out to your local representatives to push HARD for continued funding of waste water monitoring. It is the most reliable, and an incredibly vital resource. Without information about viral trends, it becomes quite uncertain how to proceed for the average person and for communities.

I posted an article awhile back about waste water monitoring finding quite potentially being in a precarious position. Furthermore this would lead to outbreaks and the general public being unawares and run afoul of horrible outcomes.
The work of aggregating and collating of data is being left to individuals, which is not only horrifying, unethical and well out of step with science based methods and guidance, but highly unusual given data is kept and provided for other illnesses, especially ones as severe and concerning as covid-19 (SARs CoV 2).
For the time being, I personally will be assuming transmission is moderate to high in addition to my sources. In the absence or great reduction of data and reports, greater estimations and assessment of made, and when only observations, assumed. Be as safe as you can everyone 💝 - Admin
Please be aware of what may no longer be offered, operating or an out of pocket cost. Masks, tests (all types), vaccines, remote options, COVID-19 tracking apps. Also be mindful of any local or nationwide level policies, proposals, news or trends that cite mask and other NPI removals, bans, stigma or efforts towards criminalization.
For the time being, the following resources remains invaluable:

https://biobot.io
It has come to my attention the person whose account is Laughter In Light has falsely claimed a prominent disability advocate encouraged or engaged in doxxing and slander with no demonstrable proof which has led to great harm. Laughter in light has provided some very helpful information throughout the pandemic. It is also important to be aware, critical and hold people into account for their actions, ideologies, commentary/statements and or stances. There are many other wonderful sources to inform oneself and stay up to date. - Admin
Provides regular updates on infectious diseases news

Sadly they don't have a website or any links I know of. Their Twitter is public however and can be viewed even without an account.
Give incredible analysis and updates on SARS CoV-2! Excellent medical and scientific communicator!
Stella has been amazing since the beginning and continues to be. Definitely worth following! Check out their link tree! They're also on Tiktok!
If anyone has any international resources for updates and tracking, please add it via reblog and I'll definitely share! - Admin
#covid-19#covid 19#sars cov 2#covid#Data tracking#Reports#Waste Water Monitoring#Cases#Deaths#Excess Deaths#Long covid#long haul covid#the pandemic#pandemic#public health#Lucky#Lucky Tran#Peoples CDC#Biobot Analytics#Laughter in Light#Tiffany Najberg#Walgreens Covid-19 Index#Waste Water Scan Dashboard#Our World In Data
20 notes
·
View notes
Last Seen Blogs

kawisnm
Untitled

siklabartwalk-blog
Siklab: Artwalk

adidassuperstar11mo-blog
adidas superstar 11 - adidas originals superstar

sweetsakuma
link gallagher

fayvpor
fay! 🔱⚡️ ⸆⸉