#neuro icu
Text
Subarachnoid hemorrhage
Greetings all! I haven't done an informative post for awhile and since I'm in a neuro/surgical ICU, I figured I discuss subarachnoid hemorrhage (SAH), particularly in a critical care context.

A SAH is a type of hemorrhage stroke. Bleeding occurs spontaneously or from a traumatic source within the subarachnoid space. As a quick reminder, the brain has tissue layers creating separate intracranial spaces where blood or CSF can collect. We name these bleeds often based on WHERE they occur.
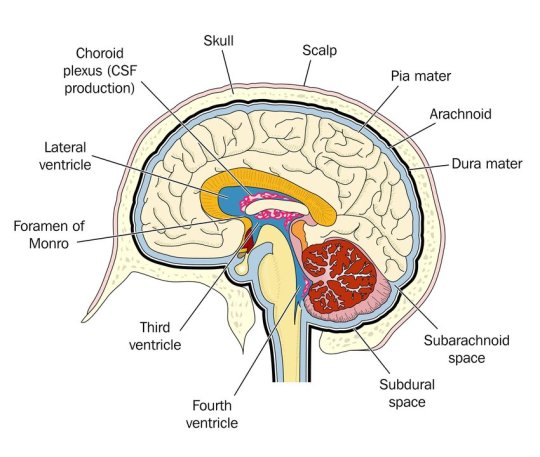
Therefore, a SUBarachnoid hemorrhage occurs beneath the arachnoid mater but above the pia mater.
Background
Most SAH are spontaneous from a ruptured aneurysm, though around 20% of SAH do not have a defined cause. Less commonly people experience traumatic SAH (tSAH) from a fall or MVC. The management of a spontaneous SAH and tSAH are different.
Most common in patients >40 y/o, with dominance in woman. Most common cause is rupture of an aneurysm, 80% of which are berry aneurysms. Risk factors for aneurysm rupture are hypertension, smoking, hyperlipidemia, atherosclerosis, advanced age, and extreme emotional stress.
Diagnosis and ED Care
Symptoms: classically the "thunderclap" headache or "worst headache of my life" which progresses rapidly over several minutes. This is usually a constant headache that pain meds really can't touch. Patients can also have nausea or vomiting - beware if you see this as it is a sign of increasing intracranial pressures. Can also have photophobia, delirium. They do NOT have a focal neuro deficit.
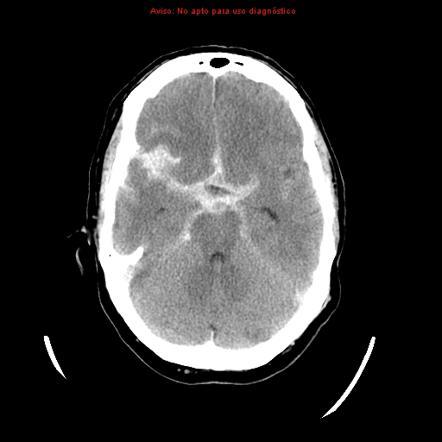
Have a LOW threshold to scan this patient's head. Diagnosis is obtained from head imaging. Get a non-contrast head CT to identify the presence of intracranial blood. Of note, xanthochromia on LP is also diagnostic; however, this isn't helpful for surgical planning. On a non-contrast CT, blood will appear white.
Surgical & Critical Care Management
Emergency Surgery: At minimum people receive a ventriculostomy to drain the head of blood. Some people with significant swelling require a hemicraniectomy. Below is a general illustration of ventric placement (also called EVD - external ventricular drain).

After immediate drainage (or sometimes before), patients receive a CTA of the head to locate the aneurysm and if surgically repairable, the aneurysm will be coiled the next day in the neuro IR suite. These patients will also receive CT perfusion (at least once, sometimes twice) to check for vasospasm.
SAH precautions: apply to all patients at all times
HOB >30
Strict bedrest
Arterial line for precise BP measurement (you'll find disagreement among critical care providers about this since arterial lines have not been shown to improve patient mortality. However, that study was NOT in a neuro critical care population)
Continued ICP monitoring (via the ventric)
Antibiotics while the drain is in place (usually ancef)
Daily stool softeners to avoid straining with bowel movements
Low lights, quiet environment (no phone, little tv, etc)
Stat head CT for any acute neuro decline
Maintenance of euvolemia (SUPER important as hypovolemia can trigger vasospasm)
Seizure prophylaxis x 7 days (usually keppra 500 mg BID)
Vasospasm prophylaxis x 21 days (nimodipine 60 mg q4h)
No antiplatelets or blood thinners.
No dvt prophylaxis until bleeding has significantly decreased (usually after coiling- surgeon dependent)
Avoid hypercapnia, hyperglycemia, hyperthermia
Aggressive blood pressure control (usually SBP <140)
Sodium goals (patient dependent, higher goal if significant swelling present)
Worth noting that tSAH patients have SOME of these precautions but not all. Nimodipine is not indicated for vasospasm prevention in these patients. I've seen it used in special situations but most commonly not. Depending on size of tSAH, they may not need a ventric or seizure prophylaxis.
Prognosis
Prognosis has improved over the past 2 decades. Outcomes are multifactorial on age, size of bleed, overall health, and presence of rebleed or complication (vasospasm, ischemic stroke) etc. Roughly 1/3 of patients have a good outcome, meaning return to baseline functionality. 1/3 of patients will have a focal neuro deficit, usually due to vasospasm which caused an ischemic infarct. The remaining 1/3 of patients die from SAH.
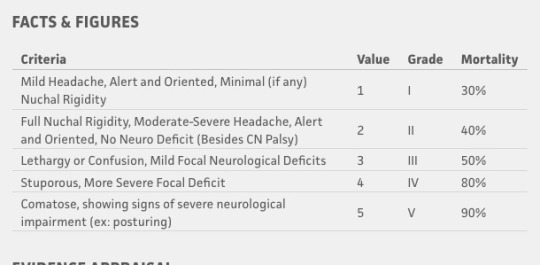
At presentation you can use the Hunt and Hess Scale to help guide education for families about prognosis. Generally, the poorer the neuro exam at presentation, the worse the prognosis. There has been some criticism that it is observer dependent and distinguishing between Grade I and Grade II is moot. The important thing about this scale is that is does NOT include the CT imaging. I personally have seen HUGE bleeds that one would think would kill the patient but with prompt intervention they have a normal exam and good outcomes.
The most common complication is rebleeding of the aneurysm even if it has been repaired. This is usually due to poor blood pressure control, vasospasm, or head trauma after SAH recovery. Rebleeding is usually bad for most patients.
These patients stay in the ICU for at least 7 days for ICP and neuro monitoring. Some stay more if vasospasm is present. I do not get to interact with patients on neuro step down and don't have the privilege to see them in outpatient clinic. But if comorbidities that contributed to the stroke are well managed and the patient receives the necessary PT/OT and other support services, outcomes are good. It's still a horrible diagnosis to get but it's not as devastating as it used to be.
If you work in neurology/neurosurgery and see these patients in clinic, please reblog and comment. I think a lot of ICU providers (myself included) get jaded with the horrible stuff we see and don't have a good grasp of longer term recovery.
#neuro critical care#neuro icu#critical care#icu#pablr#pa-c#medblr#pa-s#pre-pa#physician assistant#pa school#SAH#subarachnoid hemorrhage#neurology#neurosurgery#medicine#nurblr#pharmblr
42 notes
·
View notes
Text
How to choose the best neuro hospital in Bangalore?
Whether it's addressing epilepsy, Parkinson's disease, or strokes, the quest for suitable treatment and hospital care is crucial for those seeking relief and restoration of health.
Are you in search of the best treatment for neurology in Bangalore? Neuro hospitals stand as beacons of hope for individuals battling conditions spanning from migraines to brain tumors. These institutions boast state-of-the-art facilities and a team of highly skilled professionals specializing in nervous system disorders. From neurologists and neurosurgeons to neuroradiologists and neurorehabilitation specialists, these hospitals offer a comprehensive, multidisciplinary approach to patient care, ensuring tailored treatment plans to meet individual needs.
A significant leap forward in neurology lies in the realm of minimally invasive procedures for neurological surgeries. Traditional brain surgeries often entailed extensive incisions and prolonged recovery periods. However, advancements such as endovascular surgery and stereotactic radiosurgery enable neurosurgeons to perform intricate procedures with smaller incisions, reduced risks, and faster recovery times, revolutionizing patient care with a less invasive alternative.

Moreover, the best neuro hospital in Bangalore spearheads research into groundbreaking treatments like deep brain stimulation (DBS) and gene therapy. DBS involves implanting electrodes into specific brain areas to regulate abnormal neural activity, effectively treating conditions like Parkinson's disease and essential tremor. Similarly, gene therapy holds promise for genetic neurological disorders by targeting and rectifying faulty genes responsible for these conditions. These innovative approaches signify the future of neurological treatment, offering hope to patients with previously untreatable disorders.
Furthermore, neuro hospitals prioritize holistic care, addressing not just the physical aspects but also the emotional and psychological impacts of neurological conditions. Through specialized programs such as neurorehabilitation and cognitive behavioral therapy, patients receive comprehensive support aimed at improving their quality of life and fostering long-term well-being.
Neuro hospitals play a pivotal role in advancing neurology and providing cutting-edge treatments for neurological disorders. With a commitment to innovation, interdisciplinary care, and patient-centered approaches, these institutions continually push the boundaries of neurological medicine. As research and technology progress, we anticipate even greater strides in understanding and treating the complexities of the human brain, offering hope to countless individuals and families affected by neurological conditions.
#best neuro hospital in Bangalore#best treatment for neurology in Bangalore#Best ICU Care in Bangalore#Best Hospital in Bangalore
0 notes
Text
Services – Eesha Multispeciality Hospital in Bengaluru
Eesha Multispecialty Hospital (EMH) is dedicated in providing the highest quality compassionate and effective clinical care to those who cannot attain modern specialized health care services. At EMH, our dedicated team of doctors and specialists dissolve the gap between world class healing and home proximity.

Specialities & Services
The biggest hurdle that patients face while being diagnosed at a traditional/specialty hospital is when they are told to transfer to a different hospital due to a lack of staff and equipment. But at Eesha Multispeciality Hospital, this does not happen because of the presence of other doctors, physicians, surgeons, neurologists, etc, who can keep track of patients’ records from different departments. Our Specialities & Services It creates a uniform structure for the patients and doctors along with other hospital staff, since all the amenities are under the same roof it is easy to get treatments for various ailments without having to travel to different places and hospitals. It saves a lot of time, money, and other resources.
GENERAL MEDICINE :
The department of General Medicine, which is an integral part of the Eesha Multispeciality Hospital, provides comprehensive medical care to patients above 14 years of age. This is one of the finest facilities of its kind in the region, it offers outpatient, inpatient and 24*7 emergency care services with emphasize on excellent doctor patient communication. The department is led by some of the best physicians in this area. The department is supported by the latest diagnostic facilities.
GENERAL LAPAROSCOPIC SURGERY :
Laparoscopy is an operation performed in the abdomen or pelvis through small incisions (usually 0.5–1.5 cm) with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen. There are a number of advantages to the patient with laparoscopic surgery versus an open procedure. These include reduced pain due to smaller incisions and hemorrhaging, and shorter recovery time. There are a number of advantages to the patient with laparoscopic surgery versus the more common, open procedure. Pain and hemorrhaging are reduced due to smaller incisions and recovery times are shorter.
OBSTETRICS & GYNECOLOGY :
At EMH we deal with Obstetrics and Gynecology which are medical Specialities that focus on two different aspects of the female reproductive system. Obstetrics deals with the care of the pregnant woman, the unborn baby, labor and delivery, and the immediate period following childbirth. The obstetrician ensures that mother and child get the best prenatal care to ensure labor and delivery are accomplished without complications and that should intervention be needed, it is done quickly and safely. Gynecology deals with any ailment concerning the reproductive organs; uterus, fallopian tubes, cervix, ovaries, and vagina.
ORTHOPEDICS :
The Department of Orthopedics at EMH offers a wide range of services, including Knee Replacement Surgeries, Total Hip and Shoulder Replacement Surgeries and Spine Surgeries, as well as various kinds of innovative care for a broad range of musculoskeletal conditions. EMH has a team of highly skilled orthopedic surgeons who with the help of ultra-modern techniques and technology can assure correct diagnosis, holistic healing and speedy recovery. At EMH we offer a wide range of services from diagnosis to treatment and physiotherapy. Bone Density Screening with management of Osteoporosis is also offered by EMH.
UROLOGY :
EMH’s Department of Urology provides the latest & most advanced technology for problems related to the urinary system, like –
Treatments Available
● Renal Stones
● Enlarged Prostate Gland
● Prostate / Bladder / Kidney Cancer
● Pediatric Urology
● Neurogenic Bladder
● Urogynae Problems
ENT :
The ENT Department at NHS Hospital has experienced doctors and surgeons to deal with conditions of the Ear, Nose and Throat (ENT) and related structures of the head and neck.
Treatments Available
● Head & Neck Oncology Surgery
● Hearing Loss
● Throat Infection
● Sinus
● Sleep Apnea
GASTROENTEROLOGY :
EMH’s Gastroenterology department aims at holistic approach to various GI, pancreatic and liver diseases including Obesity and early detection and management of GI cancers.
Treatments Available
● All liver diseases and All Pancreatic diseases
● Acute G.I. bleed
● Gastrointestinal
● Track Cancers
● CBD and Gall Bladder stones
COSMETOLOGY & DERMATOLOGY :
The Cosmetology department at EMH offers a variety of therapies ranging from Laser hair removal, Anti-ageing solution, Skin rejuvenation, Scar revision, Mole excision and a variety of other therapies.
The Department of Dermatology offers procedures and services, both investigative and curative, pertaining to general dermatology, cosmetic dermatology and venereology. Comprehensive consultation and treatment is provided for both outpatients and in-patients covering all dermatological conditions including: General Dermatology, Sexually transmissible diseases, Vitiligo, Leprosy & Psoriasis.
PHYSIOTHERAPY :
Physiotherapy deals with human movement and function. It aims to maximize patient potential and return to normal function following ill health, trauma or disability for other reasons. At EMH Physiotherapists work in a wide range of clinical settings from intensive care units caring for acutely ill patients, to outpatient departments helping with people that need treatment for conditions such as a painful shoulder or twisted ankle. The service offers a positive approach to treatment planning and goal setting, encouraging patient involvement in their own care, to help them achieve personal goals. Through inter-professional working we aim to ensure an efficient and safe journey with the best possible patient outcome.
NEUROLOGY & NEURO SURGERY :
Neurology Medicine deals with Stroke, Epilepsy, Headache, Dementia, Movement Disorders, Various Muscle, Nerve, Spinal Cord Disorders. EMH is a complete all under one roof for all neurology problems
EMH provides best-in-class advanced neurosurgical services. This Institute brings together expert doctors and surgeons, state-of-the-art technology, cutting-edge treatment options and superior patient-focused care to deliver the best healthcare experience.
OPERATION THEATRES :
Eesha Multispeciality Hospital is equipped with state of the art operation theatres capable of performing all kinds of surgeries. All theatres have a dedicated air handling units to match the air exchanges and special OT flooring, both as per the international infection control norms. All operation theatres are equipped with LED OT lights, good quality OT tables, diathermy machines, anesthesia workstations, multipara monitors, defibrillators, warmer machines, central suction and all medical gases and well trained nursing and paramedic staff.
ICU WITH VENTILATOR :
Our highly trained critical care intensivists treat the most severely ill and injured persons in this department. Eesha Multispeciality Hospital has specialist to take comprehensive care of patients going through major trauma or surgery. The doctors of EMH Hospital look after the people who require advanced care and monitoring. In fact, the full spectrum of this department is provided by specialists and other medical experts specially trained in critical healthcare and are there at the Hospital 24×7 to serve patients.
OUR EXPERTISE :
Minimal Access Surgery
High Risk Obstetrics
Gynaecological Surgery
IVF Treatment
Trauma Care
Joint Replacement
Arthroscopy
Spine Surgery
Hematology
Histopathology
Cytology
Address:
11 & 30, Ramaiah Complex, Bhuvaneshwari Nagar Main Road,
Ward No. 6, H. A. Farm Post, Dasarahalli,
Bengaluru 560 024, Karnataka, India
Call Us: +91 9901616060
Email Us: [email protected]
Link : https://eeshahospital.com
#Eesha Multispecialty Hospital#Multispecialty Hospital#Multispecialty Hospital in Bengaluru#Eesha#Eesha Hospital#General Medicine#General Laparoscopic Surgery#Obstetrics & Gynecology#Orthopedics#Urology#ENT#Gastroenterology#Cosmetology & Dermatology#Physiotherapy#Neurology & Neuro Surgery#Operation Theatres#ICU With Ventilator
0 notes
Text
The Implication of Neurologists for neurosurgery

A Neurologist is a medical doctor who diagnoses, treats, and manages problems in the brain and nervous system. A neurologist from a neurology hospital in Noida is aware of the anatomy, feature, and situations that affect your nerves. It controls everything you think, sense, and do — from shifting your arm to the beating of your coronary heart.
What's a Neurosurgeon?
A Neurosurgeon at the best Neuro hospital is a scientific medical doctor who performs surgical treatment on the brain. Neurologists treat humans with medicinal drugs, bodily therapy, or different strategies. You can find the Neuro hospital in Noida for neurosurgery.
What forms of tests does a neurologist advise?
• Angiography: Angiography can show if blood vessels to your mind, head, or neck are blocked, damaged, or extraordinary. It could come across such things as aneurysms and blood clots.
• Biopsy: A biopsy is the removal of a chunk of tissue from your body. Biopsies can be taken of muscle, nerve, or brain tissue.
• Cerebrospinal fluid analysis: This check entails the elimination of a sample of the fluid that surrounds your mind and spinal twine. The take a look can come across evidence of mind bleeding, infection, multiple sclerosis, and metabolic diseases.
• Electroencephalography (EEG): This test measures your brain's electrical interest and is used to help diagnose seizures and infections (which include encephalitis) mind damage and tumors.
• Electronystagmography (ENG): This organization of exams is used to diagnose involuntary eye motion, dizziness, and stability issues.
• Myelography: This test enables diagnosing spinal and spinal cord tumors and herniated disks and fractures.
• Polysomnogram: This look measures mind and frame activity at some point of sleep and enables the diagnosis of sleep issues.
• Positron emission tomography (pet): This imaging check can show tumors or be used to assess epilepsy, brain tumors, dementia, and Alzheimer's sickness.
• Thermography: This test measures temperature adjustments within your body or precise organs and is used to assess pain syndromes, peripheral nerve issues, and nerve root compression. You can check online for the best trauma hospital in Noida.
#ICU facilities doctor hospital near me#ICU facilities hospital near me#best ICU hospital in noida#best ICU hospital in Delhi NCR#best trauma hospital in Noida#best trauma hospital in delhi ncr#trauma hospital in noida#rauma hospital in delhi#best neuro hospital in Noida#neuro hospital in noida#neuro surgery hospital#neuro surgery hospital in Noida#neurology hospital in noida#neurology hospital near me#neuro hospital near me#neuro surgery hospital in sector 70#neurology hospital in sector 70#neurosurgeon in noida#best neurosurgeon in noida#best neurosurgeon in in delhi ncr#neurosurgeon near me#neurologist near me
0 notes
Text
There is one thing I will miss about nursing and that's cute accessories — aesthetic cheat badge cards, colourful torch lights, brain-shaped badge reels, rainbow lanyards, mini whiteboard markers, pronoun pins, handover notebooks with beagles and cats, crocs with medical jibbitz... Maybe I'll post my little collection before I give it away when I leave work...
It probably tells a lot that this is the only thing I'll miss
(And maybe the times when you give some extra time and attention to a patient during personal care and they tell you they already feel more like themselves a bit and get that new spark in their behaviour or trying to talk more when their family comes to visit... despite how unprioritized personal care is on neuro icu, or any critical care in general, I always found it to be very soothing and rewarding)
EMT/paramedic uniforms are nicer than scrubs (and more gender euphoric for me) though and I'd be glad to leave for a slightly less toxic field with slightly better pay and career options
#i saw some stuff in nursing and I don't mean the horrible trauma pts or psych pts or even the standard of care from docs#some of my colleagues have zero empathy and id not trust them with me or my relative#most are competent enough on the medical side (most...) but the way some nurses treat their patients as a nuisance is just heartbreaking#i think i'd go crazy if i had to do nursing for another year and watch it not being able to do anything about it#the lack of choice in pts' own care on wards is also horrifying#me posts
10 notes
·
View notes
Text
So 7 full months after my surgery, my insurance sent me a letter that says they covered my surgery but not the 1 (one) night stay in the neuro ICU I needed right after because they deemed it "not medically necessary."
I started bleeding from the access site in my femoral artery at 3am and only survived because I was in the neuro ICU and had nurses checking on me every hour for exactly that reason. I fucking hate what we've done to healthcare in the US.
Also please don't give me advice about how to handle this, I know what I need to do, I'm just venting.
#personal#medical stuff#insurance companies are straight up evil#i can't even appeal yet because they just sent the denial letter not the claim info letter so I'm just sitting here steeped in dread
9 notes
·
View notes
Text
So, I'm sleepless at 1am and I'm tired and I'm upset so I'm going to get out the shit that has been going on for me the past month and a half, because it keeps leaking out in tags and I guess maybe I should not do that. This is going to be long and it's a huge bummer. I just don't feel like I can come out and talk about it directly to anyone because it is indeed a huge bummer and I just. can't deal with like. the feeling of unloading this on someone and then what.
but throwing it into the tumblr void and hiding it behind cuts feels less like I'm throwing a bunch of gross stuff at someone's feet so like, yeah.
Content warnings for uh, facing the mortality of aging parents, the American healthcare system being a fucking nightmare, mentions of strokes, infections, and other huge medical problems, and basically stuff being awful.
I have lived with my mom as her caregiver for the past three years, since losing my job during covid. She is six years in remission from breast cancer, diabetic, and in end stage renal failure, meaning her kidneys don't work and she needs hemodialysis 3 days a week. I came in mostly to do things like shopping, the majority of cooking and cleaning, be present in case of falls, things like that. It's worked out, mostly. It sucks that she had to move to AZ to live near her brother simply due to the fact that her cozy little house in MT that she got remodeled to her needs has no dialysis centers within an hour's drive and the closest ones had no open seats anyway, not even for a summer stay, because of the nationwide nursing and technician shortage in healthcare. So she lives in AZ and goes to dialysis 10 minutes away. It works out, sorta.
But.
Since August 1st:
she had a stroke, which affected the language centers of her brain and made speech, writing, and complex communication difficult
she spent a week in neuro ICU for follow up; this was at a hospital 20 miles away in Phoenix. yes I drove there every day to see her.
she was transferred to a rehabilitation center after that week, where she had several good days but then started to experience severe lower back pain.
the back pain got so severe that she was crying and even screaming when being helped into/out of bed, or having the head of the bed elevated so she could eat.
myself and her other present family were very upset about this, because she was in pain! and also it was preventing progress in her PT/OT after the stroke! we wanted them to do something and find out what was going on!
an xray was done. "no significant findings."
we asked for a CT scan or MRI if an xray found nothing.
it didn't happen. maybe insurance said no, maybe assumptions were made that it wasn't necessary.
but mom spent the rest of her 15 days at that rehab facility on tylenol and then oxycodone.
she was then discharged, and yet in no state to come home.
we found a short-term care facility for her that she'd actually stayed at after her initial ER stay that discovered her renal failure. we thought that she'd do okay there.
she didn't. she declined. she was still in severe pain. MWF for her dialysis, she was basically just, done. and they had scheduled her dialysis at 6am. so. the day was just over, no ability for therapy.
they still just gave her oxycodone so even on good days she was sleeping a lot and very out of it.
we asked to speak to the physician and her case worker. we were not able to.
we asked for her to get further testing instead of just this pattern of throwing narcotics at her and watching her decline. it didn't happen.
at the end of her second week there, she was becoming less responsive and more inclined to just sleep.
she wasn't eating. I tried so hard to encourage her to eat, I even fed her. she still would eat a few bites and then be uninterested in more.
one day she only ate a cup of yogurt.
then she was so badly out of it and barely responsive that I demanded that they do something. so they gave her narcan. because maybe she was too lost in the oxycodone sauce. didn't help, they gave her more. didn't help. they called EMTs.
she ended up in the ER, where they did a CT, MRI, and bloodwork.
(this was a week ago)
turns out she has an infection in her spine. which is osteomyelitis, an infection in the bone and bone marrow that just constantly hurts. oh also numerous pressure sores, including a bad one on her heel, and a bad one on her lower back. either could have introduced the infection into her spine.
that infection has spread to her blood. yeah she's got sepsis.
she also has had at least one additional stroke and her speech has degraded even further.
she spent several days in the ICU and it was very touch and go.
it is still very touch-and-go but she's now in progressive care (pcu) which is a downgrade from ICU in terms of how serious.
but yeah. sepsis is very dangerous for young and relatively healthy people. she is 74. her diabetes means her healing is very slow. her renal failure means that her system can't handle a heavy load of antibiotics so they have to be given more spaced out and in lower doses.
it. sucks.
I still go to see her every day and talk to her even if she's not responding. I sing songs she knows. I put on videos of the church services in her hometown for her to listen to. - it. sucks. so. much.
oh yeah also her place here in AZ is in a retirement park and I can only be here because she resides here. so if something happens even in terms of her moving her permanent residence elsewhere I can't stay here.
I have no income I basically just lived here with her and she covered my expenses as my pay for being her caregiver. so like. looks at the potential need to get independent housing, looks at bank account with $30 in it, laughs darkly and decides I can't think about that.
besides I need to think about how this could be the last time I have left with my mom.
it. sucks.
14 notes
·
View notes
Text
17/5/23 // 21.50
It’s been a while! Here’s some more neuro notes, and quite conveniently for me, I have the pick of the patients to do as a case study because I’m essentially working in a neuro icu atm. GBS, encephalitis, some weird neuro things that might be meningitis, and a stroke patient. What a time to be studying neuro!
#mine#studyblr#studyspo#notes#studying#pharmblr#pharmacy#medblr#Maria does diploma#heystasia#heyharri#lattesforlaura#myhoneststudyblr#Maria does icu#that’s a tag now okay#imagine me. ya gal. an icu pharmacist.#every time I answer my bleep as I’m the icu pharmacist I highkey freak out#I’ve officially made it#anyway these patients are super interesting sorry to the boring post op monitoring and the paracetamol overdose but you do not excite me#patients with weird and wonderful conditions excite me#even if that’s a 4pm warfarin problem
21 notes
·
View notes
Text
8. Persistent Fever
Part 1 | Part 2
With the drain in, Finn’s obs came up to a more acceptable level, the sedation they’d given him helping to keep him settled whilst they did it. With that sorted, they’d let Fao clean and even close the cuts to his head, talking softly to his brother as he did it all. He knew they’d bent the rules for him to let him do that, but he appreciated it. It certainly helped Finn out, and the nurse commented that he’d not been that settled or content.
They’d got him a place on ICU, and soon enough he was taken up there. Fao followed wearily, feeling exhausted and overwhelmed. Finn was still very sick, that much was obvious. He knew ICU was the best place for him, but it was still worrying. Nobody wanted their brother in intensive care. Fao was worried about his seizures, too, but they said Steve would see him whilst he was admitted to try and control them.
His fever was the most worrying, seeming to not get any better even with all of their treatments. It would take time, but for the moment, it was less than ideal.
Steve appeared after a while, Finn’s case perplexing him. The discussion he'd had with the ED hadn't shed any more light on it, but the scans hadn't shown anything he was too concerned with. Of course there was the matter of his infection, the antibiotics he'd already been on apparently having done nothing. The chest drain was a necessary evil, but Steve couldn't help the worry about it and his seizures. Finn wouldn't be conscious, of course, but it wouldn't be pleasant for him to pull it out.
Fao had settled at Finn’s bedside, exhausted from a long night and not a lot of sleep. He’d ended up resting his head on the bedrails, just to close his eyes for five minutes. At least he’d still be close to Finn, able to settle him if needed, or speak to the staff if they needed anything.
Steve sighed as he saw the brothers, reminded of their first meeting so many years ago. He cleared his throat gently. "Knock knock."
Fao lifted his head, hair falling in his eyes. “Oh, Steve. Sorry, wasn’t asleep, I swear.”
"You don't need to apologise." He said with a smile. "You deserve the rest. How are you getting on?"
“Ah, y’know. Glad he’s got a bed now.”
"Yeah, of course."
“He’s settled now, at least.”
"He's had some sedation, hasn't he?'
Fao nodded. “And he’s finally stopped fighting it.”
"Bless him. I'd got a bed organised for him for the morning, your mum had said he was starting to struggle with absences and the paracetamol wasn't helping with his fever."
“When she called me tonight I assumed it was the big seizure we’ve all seen coming, but of course he had to be different.”
"Of course, it is finn, after all."
“Never a dull moment.” Fao said drily.
"That's very true."
“I suppose he couldn’t let me have all the fun.”
"You and Harrison caused enough stress, I don’t need him joining in, and I bet She and Fred don't either." Steve managed to joke.
“How is Harrison?” He asked. “Haven’t spoken to him in a little while.”
Steve's smile grew forced. "He's getting there. He's struggling a little with everything, but you know what that’s like."
“All too well. I’ll text him.” Fao said. “I’m guessing you’ve come to see Finn, I’ll stop distracting you.”
"Came to see both of you." He said softly. "There's not much neuro-wise I can do at the moment."
“Both of us? I hope I don’t need a neurosurgeon.” Fao joked weakly.
"I'm not on the market for more patients." Steve joked back.
“Good.” He murmured. “I’m good with my head intact, thanks.”
"Though I'm sure Sheila would be surprised to find you did have a brain." He teased, moving to Finn’s side. "Finn? Just Steve, you're okay."
Finn gave a groan, taking a moment to manage to open his eyes. He finally focused on Steve, gave a grunt in acknowledgement, and then rested his head back down.
Fao reached across to squeeze Finn’s hand. “Steve’s checking up on you, eh?”
"It's a stupid question, I know, but how are you feeling?"
Finn made a noise, his voice muffled by the mask. "Tired."
Fao huffed a laugh. “You and me both, kid.”
"I don't blame either of you."Steve said. "Aside from tired? Any pain?"
"No." Finn shook his head. "Fuzzy."
"Like before seizure fuzzy, or after fuzzy?"
That was too much effort. "Both."
Fao couldn’t help but smile. “Always helpful, Finn.”
"How many have you had now?" Steve murmured, looking through the notes. "Right, I'll ask them to keep an eye on it, I'll change the lorazepam to immediately if he does. What's the valproate doing? Hmm, I'll add that too, his other levels are good, that's fine."
Steve trailed off, making a few notes before returning his attention back to the brothers. "Right, a bit of a plan for you two. They're gonna keep the sedation going anyway, make that a bit more comfortable for you, Finn. I'll increase your normal meds, the new one we're trying, and that should help keep them away. If you do have a seizure, we've got that management plan in place and ready. I've written you up for more pain relief too, so just ask. You don't have to wait until if you have a seizure."
It was too much for Finn to pay attention, but he nodded all the same. "'Kay."
“Thank you, Steve.” Fao said, taking it all in.
"Is there anything else you need from me? Or want me to do?" He asked gently.
“No, no.” Fao murmured. “Other than tell the staff I’m a doctor that works here, none of them recognise me.” He couldn’t help the little laugh. “And obviously just keep looking after Finn.”
"I saw you'd managed to sort his lacs out, you did a good job." Steve said. "I'll make sure to let them know."
“They were great in ED.”
"I'm glad." He gave him a genuine smile. "I'll pop back later, see how the two of you are getting on."
“Thanks, means a lot.”
He hesitated before he left. "Hars wouldn't mind a text, and you're always welcome at ours."
“I’ll text him. Gotta keep myself entertained whilst sleeping beauty gets his rest.”
"Of course." He laughed. "Take care."
“And you.” Fao murmured, turning his attention back to Finn.
Finn gave a grunt in acknowledgement that Steve had left, already mainly asleep. He struggled to get comfortable, tossing his head in frustration.
“Here, let me help.” Fao said, standing up to fuss with Finn’s pillows.
He caught Fao's eye as he helped, frustrated and tired and feeling rubbish. Fao fixed the problem though, and that earned a sigh in content, one thing less to complain about.
With the pillows fixed, Fao moved to stroke through Finn’s hair, leaning over the bed to press a kiss to his forehead. He was still absolutely burning up, despite everything they’d done, and his hair was damp with sweat. He wasn’t quite as aggressive and delirious as he had been, but he certainly wasn’t well, and it seemed like everything they were doing wasn’t doing enough.
Biting his lip, he sat back down, worry churning in his stomach. He kept his hand in Finn’s once he was settled, lifting it to press a kiss to his knuckles.
“Love you, Finn. Don’t do anything stupid, please. Let’s get rid of this fever, it’s not doing you any good at all.”
#sicktember 2023#sicktember day 8#persistent fever#whump writing#whump prompt#oc#fic#finn daniels#faolan blackwood#brothers in more than arms#steve cunningham#seizures#ICU#intensive care#worried carer#mention of medication#finn's having a bad day#so is fao lbr#pneumonia
13 notes
·
View notes
Text
a girl i went to high school with finished early bc she got pregnant and then did an accelerated nursing school program and has been a neuro trauma icu nurse since she graduated and i think that's so crazy. like impressive but crazy because those people need so much care
7 notes
·
View notes
Text
Why choose the best treatment for neurology in Bangalore?
In the face of adversity, the strength of one's spirit becomes evident. Whether grappling with the physical aftermath of an accident or the enduring emotional scars of trauma, our committed healthcare team endeavors to provide tailored and holistic support for recovery and rehabilitation.
Trauma, whether physical or psychological, can cast a lengthy shadow over an individual's life. Particularly, head trauma presents myriad challenges necessitating attentive care. Recognizing the profound interplay between bodily injury and emotional turmoil, our approach is rooted in empathy and practicality—a collaborative, compassionate effort aimed at restoring lives.
As a premier accident and trauma center in Bangalore, we have broadened our scope to encompass diverse rehabilitation services, each meticulously crafted to address specific trauma-related concerns, with a particular emphasis on head trauma. We hold firm to the belief that every path to recovery is unique, and our comprehensive methodology ensures the holistic well-being of each individual.
Renowned for their proficiency in diagnosing and treating various neurological disorders, Bangalore's leading neurological care centers boast a team of expert neurologists, neurosurgeons, and specialists, ensuring patients receive cutting-edge treatment modalities.
Equipped with state-of-the-art diagnostic tools and technology, these centers facilitate precise diagnosis and personalized treatment plans through comprehensive evaluations, ranging from advanced imaging techniques to neurophysiological assessments.

Employing a multidisciplinary approach, the best treatment for neurology in Bangalore unite professionals from diverse fields—neuroscientists, neurosurgeons, neuropsychologists, and rehabilitation specialists—to deliver holistic patient care, addressing the complex needs of each individual.
Furthermore, fertility centers in Bangalore offer unparalleled treatment options and interventions, whether through advanced surgical procedures or innovative neurostimulation techniques, prioritizing patient-centric care to enhance efficiency and elevate quality of life.
#Accident and trauma center in Bangalore#Best treatment for neurology in Bangalore#Best ICU Care in Bangalore#Best Hospital in Bangalore#Best Neuro Hospital in Bangalore
0 notes
Text
[Encore] The Neuro Nursing Chronicles: A Masterclass from the Archives
In this episode, we are re-sharing our most popular neuro episodes from the archive in one massive episode. Kati Kleber, Elizabeth Mills, and Melissa Stafford (all experienced neuro ICU nurses) discuss:
When to worry about your neuro patient
The most common disease processes for acutely ill neuro patients
Common neuro meds
Frequent diagnostics
How neuro patients are monitored
Common neuro surgeries
These episodes were originally recorded in 2018, but the information is still incredibly relevant today for neuro nurses. This content is for informational purposes only; best practices may have changed.
For ALL of our neuro nursing content: https://www.freshrn.com/neuro-nursing/
For our free mini-course on conscious neuro assessments, click here: https://courses.freshrn.com/p/neuro-assessments-mini-course
To learn more about our comprehensive neuro prep course, Neuro Wise: A Crash Course For New Neuro Nurses, click here: https://courses.freshrn.com/p/neuro-wise
Learn more about the FreshRN All-Access Pass here - https://courses.freshrn.com/p/membership
To see our latest course catalog (med-surg, ICU, precepting, charge nurse, ortho, cardiac, neuro courses, and more), click here: https://courses.freshrn.com/
Get weekly tips, encouragement, stories from the bedside, and more - just for nursing students and new nurses at: https://www.freshrn.com/email-sign-up/
Connect With Me Online!
Facebook: https://www.facebook.com/FreshRN
Twitter: https://twitter.com/Kati_Kleber
Pinterest: https://www.pinterest.com/Fresh_RN/
Instagram: https://www.instagram.com/kati_kleber/
TikTok: https://www.tiktok.com/@freshrn
Music credit: Keep My Cool by Benj Heard
Check out this episode!
4 notes
·
View notes
Text
MAG 122 Relisten
Activity on my first listen: baking something with apples
Ah yes, another episode with a meta-title. The statement is about "zombies", and Jon just returned from the dead.
BASIRA: "Could he have come back? Moved it?"
GEORGIE: "I guess?"
So there's some time between Georgie running into Oliver and this. She obviously called Melanie/Basira about the tape recorder and Basira came to the hospital. And in this time, Georgie reckons, Oliver could have had the opportunity to come back, so Georgie wasn't with Jon at least this whole time between MAG 121 and now.
BASIRA: "What, capital ‘D’ Death?"
GEORGIE: "Yeah. Y’know, one of your… dark gods –"
BASIRA: (frustrated) "They’re not –"
[SHE CUTS HERSELF OFF.]
This tells me that broadly speaking Georgie still has no idea what is going on with the Fears. It's okay if you don't understand something and don't want to understand something. But then you also have no right to tell people what to do about it.
BASIRA: "Right. So how exactly is it that you’re able to identify an avatar of the End on sight?"
GEORGIE: "Honestly Basira, it’s not your business. (pause) Sorry."
(Warning, bit of Georgie slander xD) Yeah, I know, Georgie doesn't know Basira and therefore there is less trust to feel comfortable enough to tell why she's could identify Oliver. But the low-key hypocrisy. In the end, emotionally nobody ows anyone. Basira probably wanted to evaluate the situation and that also means evaluating, if Oliver was actually an avatar. Georgie probably saw it as an attack. (Like S1Jon asking every statement-giver if there was the possibily that they all just dreamed it!). Understanding what messages can say without directly addressing it is a key to understand communication. If anyone's interested, look up the four-sides-model of a message.
BASIRA: "I don’t know. The whole tape thing is… I don’t know."
GEORGIE: "Right, well… I showed you like you asked, so –"
BASIRA: "Shh."
Okay, ignoring that Basira spotted the tape recorder, between Basira's "I don't know" and Georgie's "Right, well..." I already hear breathing sounds.
Ah yes, later the breathing more clearly audible and also addressed in the transcript.
GEORGIE: "So – what does it mean?"
JON: (hoarse, tired, drained) "That’s a very good question."
Okay, I mean the coma in itself is a trope often used in like family dramas. But the suddenly waking up and speaking is also such a trope! And I knew this day would come and the last 3 days I've been pestering my family (incl. former neuro ICU nurse) to tell me if there are any plot holes! (Luckily, they also listened to TMA...) Now, in consideration that this is a "magical" coma and the recovery of the patient is also fully supported by "magic", you can throw a lot about waking up overboard (for example that it's usually a slow process). I always thought someone in an ICU who needs ventilation is definitely intubated (what could have made the waking up and immediately speaking kinda impossible), but the nurse in my family said, it's not always required. You can go without intubation with the head-tilt and chin-lift manoeuvre to avoid air going down the esophagus and into the stomach. Sounds like hell of a strain on the neck, but said nurse family member seemed very on board with the portrayal here. I've heard them nitpicking about sci-fi before, so there are instances where they're bothered by things like this.
Btw. I'm also guessing the Institute paid for a fancy room with only a single bed.
I was a bit surprised how Jon insists that he is alright but then, I mean, he doesn't know he's been in a coma for 6 months. He probably thought it was like the next day or next few days after the Unknowing. Which, was btw. on August 7th, Elias was arrested on the 9th of August and now it's the 15th of February.
JON: "Six… Uh, the others. T-Tim. Is he…?"
Tim is actually the first thing that comes to his mind when realizing the Unknowing went not so smooth, that his position in the wax museum put him in a 6 months long coma.. Jon was semi-aware at the end there, and this realization immediately bringing him to Tim could be seen as a sign, that he may remember a bit more of what was going on including Tim's last words to him... Even if he wouldn’t admit it...
JON: "Honestly, I – I, I think I’m alright. I mean that’s – good, right?"
GEORGIE: "After a six month coma? No – it’s not. This isn’t how it’s supposed to go, Jon."
JON: "I – what? Y-y-you’d prefer I was – brain-damaged? Dead?"
So yeah, usually waking up from a coma is a process. Jon waking up and being super alright tells Georgie that Jon has officially turned into one of these "monsters" he talked about. Because there is no way a "normal" human could recover that fast. This is also a good example four-sides-model of a message.
GEORGIE: "Jon. If this really is a second chance, please try to take it. But I don’t think that it is."
JON: (breath) "Georgie, I don’t underst–"
GEORGIE: "Take care of yourself."
Georgie can't feel fear, but she does know what Death feels like. I once read the headcanon, that Georgie could also feel that on Jon, since he freshly got his End mark. Either way, I can kind of understand that she's upset and runs away, even if it is really bad timing for Jon's mental health. I do not blame her for cutting ties, that is very much her right to do.
Basira bringing a statement. Bit of an Eye moment there? Or just in case, since there was a tape recorder. Also, bringing a statement means she thought it would help Jon? So I can't really feel her being disappointed?
JON: "Recording by Jonathan Sims. The Archivist."
That self-awareness... acceptance? resignation? of what he is now...
"So maybe it isn’t quite as surprising as all that. I like animals, too. They don’t pretend to be important."
Yeah, can relate. Not that I don't understand emotions on the faces of others, mostly I even feel them too much I think. But animals don't assume. They might judge you on occasions, but if you're good to them, they won't hold it against you. You can try to be good to certain people all you want and they will just hate your guts and will let you know it.
Hearing about the statement-giver experimentally cutting this Liam to see if they're real is one horror I find in this statement. The statement-giver, who won't see you as a human being...
"The next day he was there again, this time in the hallway outside my office, standing in the center, so that I had to hug the wall to avoid touching his… motionless form."
Yeah, that's more like it. People ignoring you... How it makes you feel...
On the subject of zombie, I don't really follow the concept of P-Zombies. But I really could feel the zombification as Dr. Steven Scholzman describes it. It's more about other people not seeing you as an individual. You're just a number, an NPC just like any other. A zombie won't care if they eat your brain or the brain of the one next to you, or the one behind you and therefore taking your individualism. Look it up, Dr. Scholzmann has TED talks about this, one about zombies and one about horror, really interesting.
JON: "They can be hard, though, other, other people. Feelings."
Like the whole opening scene just proved.
JON: "I’m trying to focus, trying to make sure I’m the same me as before, but… how can anyone really remember that? How do you know you’re the same person that went to sleep?"
Oh yeah, hit me with that existential shit, I love sitting in those thoughts! Generally though, there are certain situations out there, when you can absolutely tell, that this is not you. Depersonalization under Burn-Out for example. Would also fit theme of lack of empathy against others of this statement.
JON: "Honestly, I’m surprised Martin isn’t –"
[BASIRA TAKES A DEEP BREATH.]
JON: "What? (realizing) Oh god – the, the plan, it’s – Martin i-is – is he okay, w-what –" (he takes a breath to compose himself) "What did Elias do?"
Yep, a Martin of 6 months ago would totally be the first one in the hospital. That poison in the last sentence though, realizing that something must have happened because Martin would totally be here otherwise.
JON: "What did he do to Martin?"
BASIRA: "I… don’t know. We don’t see him around the Archives much these days. Best I can figure? He’s working on something with Lukas."
JON: "No, that – No, that – that – There must be something else."
Martin willingly, though for a greater purpose of helping others, joining an avatar and Jon can't quite believe that he would actually do that... Hmmmmm MAG 194...
BASIRA: "I’ll get you some new ones. Better ones."
Lol. First, Basira says Jon's clothing style wasn't really good. And I'd like to know what kind of clothes she buys for him XD
JON: "Oh, or, uh, a cup of t–"
Awww! I'm sure somewhere he began to really like Martin bringing him tea.
@a-mag-a-day
22 notes
·
View notes
Note
this feels almost a little stalkery to write, but i just realized you haven't posted anything in a while - i always enjoyed your posts in my feed. Hope you're doing well off-tumblr and wish you an awesome New Year! 🌟
Hi there and late Happy New Year to you (and anyone who reads this) 🎉✨
This is not stalkery at all - it's actually really nice...🥹
In short, the past two months ve been awful irl for me, winter pressure in nursing is horrendous and as someone who works in ED/neuro ICU I'm just too tired for much most days. My health's been shite since cluster headaches are back and my adhd/depression are all-time high, and there's been some other shite going on in my partner's family, I just don't have much energy for the online stuff
I pop here from time to time when I have a slower time (like rn) but don't do much, it's all just piling up in my inbox/drafts/etc and I'm incredibly sad (and feeling a bit guilty) b/c tumblr is my fav place online and fandom people are so dear to my lil heart 💔
Probably gonna make a longer ramble-y post about it all soon-ish, sort out some posts, etc since I'm finally starting to get back on my feet, I'm in the process of switching to EMT (got the job finally!) and also doing my ambo driver training which just makes the hours at work add up
I'll be back with my crappy posts, promise, and I'll get most of my shit in order, I just need a minute...
#Thank you for popping in my inbox anyway#it really warms my heart alright#sorry to anyone who's been expecting stuff from me 😔
7 notes
·
View notes
Text

The NET brand HF810C ICU Bed Motorised with Battery Backup boasts major features such as backrest, knee rest, height adjustment, Trendelenburg/Reverse Trendelenburg, cardiac chair position, neuro position, and zero-level position, all maneuverable by four separate linear actuators operated through integrated panels on side rails.
https://www.narang.com/hospital-medical-furniture/hospital-beds-icu/HF810C.php
3 notes
·
View notes
Text
Aftermath
Age Rating: 12+
Chapters: Two of Three
Fandom: Grey’s Anatomy
AN: Here’s the second chapter enjoy and I always appreciate a reblog and like.
Summary: Amber helps Jo and Jenny with Paul that ends in an unexpected note.
Words: 1931
After my breakdown in the locker room I opted to spend the rest of the day making sure Paul is alive and not pressing charges against us. It will help keep my mind busy from the fact that I’m about to get fired. And as mad as I am at Alex for inadvertently getting me in this mess, I wouldn’t want to see him go to prison for something he didn’t do. I know it’s irrational of me to be angry at him especially since he didn’t know about Paul until recently but as my dossier points out I’ve got anger problems.
I spot Alex and Jo by the medical cart in the ICU right outside of Paul’s room. I shake my head at their stupidity and approach them calmly. I stand in front of them ready to tear them down.
“You know why don’t you guys just hang up picket signs that say, ‘I Did It!’ you standing outside while he’s dying isn’t suspicious enough.”
“It wasn’t us.” Jo states defensively.
“Yeah believe me I know.” I admit, “But that doesn’t mean the police will and I know you and I are good but Alex is not gonna survive prison.”
Alex looks at me offended, “Did you just come here to insult us? Because we’re freaking out enough as it is.”
“Oh I know.” I whip my hair back over my shoulder, “People who freak out make extremely poor decisions that can make them look like murder suspects.”
“Shepherd came back with her neuro results.” Jo tells me and I listen, “It’s a severe concussion and broken ribs.”
A part of me is glad he’s okay but after my meeting another part of me was hoping he would get a colonoscopy bag for the rest of his life. Then I wouldn’t be the only one with a mess to clean up. I pinch the bridge of my nose in conflict that Alex catches as he looks at me concerned.
“Are you okay?”
“Do you know how stupid of a question that is right now?” I ask Alex in a bitchy tone, “So if none of us ran him over then who the hell did?”
“We have one theory.” Jo says uneasily, “We think it was Jenny who did it. I mean you saw her when she left with him, she was terrified and I told her it would only get worse she did this because of me.”
“I think she would’ve gotten behind that wheel with or without your help.” I inform her, “Trust me hell hath no fury like a scorned woman, it’s the only book that caught my attention when I had to fill my humanities requirement. Besides I think I’m more likely to go to jail than you after the police see the damage I did to Paul’s nose.”
“You can say it was from the hit and run.” Alex offers and I nod in agreement with that plan, “Hey heads up.”
I turn around and I see Jenny Walker approaching us with a coffee in her hand. She looks pretty normal for a woman whose fiancé was almost killed which supports Jo’s theory more. I stand by them so they aren’t facing her alone and don’t say anything stupid in front of her. If history serves with these two it’s a frequent problem.
“Jo. Amber.” Jenny stands in front of us.
Alex comes in to our defense, “They really shouldn’t be talking to you.” Twice in two days I get an overprotective brother, it’s a new record over the past decade.
“I know.” Jenny persists, “I just need one minute please.”
Alex looks at her suspiciously but I decide to let her talk to us. She might say something incriminating and get us off the hook. I turn to Alex and say assuredly, “We’ll be fine.”
Jo agrees with me too, “It’s okay.” Alex reluctantly walks outside the ICU as we both face Jenny who leans in and whispers.
“I just want you to know you don’t have to worry. I didn’t tell the police anything.” Okay we’re getting somewhere now we just need a confession.
“What do you mean?” Jo asks.
“I didn’t tell them it was either of you.” Her words catch me off guard and I look at her in mild shock as she looks at us gratefully, “But thank you, thank you so much.” My mouth gapes open as I look at Jo who also has her mouth open from finding out it wasn’t Jenny who hit Paul.
------------------------------------------------------------------------------
Jo and I lead Jenny to an empty ICU room and close the door behind us so we can have some privacy. This kind of discussion over who ran over Paul is not the kind of gossip the nurses need to say through the grapevine. God knows they’re still on the topic of me.
“Wait.” Jenny faces us confused, “I-I was at the hotel. He got mad and went for a walk and told me to stay p-it wasn’t you two?”
“No!” Jo and I exclaim in shock and I continue, “I went to my brother’s place and she was in bed when I got there. We didn’t find out until my friend came barging in, we thought it was you.”
Jenny looks perplexed at the sheer coincidence, “Who do you think did it?”
“An avenging angel?” Jo throws in and I shake my head at her suggestion.
“I’m sorry.” Jenny tells us in shame.
Jo doesn’t have it though, “No you don’t have to-”
“I do.” Jenny continues, “I really thought I was better than you. I believed everything he told me about you.” She turns to me with pleading eyes, “I should’ve said something when he barged in like that and told your friends all that stuff about your mom and your brother, oh my god I am so incredibly sorry.” Jo looks at me in sympathy over this new information.
“I don’t think that bastard would have let you get a word in edgewise.” I retort bitterly, “It must have been satisfying to see me punch him though.”
Jenny’s eyes glisten, “Not as much as I wanted it to no. God! I'm smart. I'm a scientist. I'm a feminist. I never thought that I would end up in something like this.” My anger towards Jenny shifts to pity as she explains her side, “It happened so slow. I stopped talking to co-workers, friends he didn't like. Then my family didn't understand. They got worried. So I just brushed them off and then stopped talking to them, too, and then my circle got smaller and smaller and smaller until all I had left was him. And then I stopped believing myself, things I had seen and heard, things I knew, because he told me I was crazy and I just believed him. He knows me so well. He can zero in on an insecurity and make a whole argument turn on a dime, and now it's my fault. It's my fault again. I'm always the one that's wrong. When he started hitting me, it was just barely a surprise. And he told me it was my fault, and I actually believed him. Until you talked to me yesterday, I really believed him. How did I believe him?”
“Because he was good to you in the beginning.” Jo starts, “And on the good days. Jenny, we're not stupid. We didn't fall for someone who beat us. We fell for someone who made us laugh and feel wanted and loved and seen. Paul is brilliant and charming and persuasive, and the good outweighed the bad until it didn't.” I look at Jo in awe over how she explains it wasn’t their fault and that there comes a time you have to save yourself even from someone you love. And now it’s Jenny’s turn.
------------------------------------------------------------------------------
I offered to be there with Jo and Jenny when they confronted Paul and let me accompany them. We stand outside the room as Dr. Shepherd exits the room.
“Are you the fiancée?” Shepherd asks Jenny, “Maybe you can talk some sense into him.”
Dr. Grey tries to stop us, “This is not a good idea.” We ignore her and walk around her to face Paul who looks at us annoyed. It’s taking everything in me not to press on that headlac of his.
“Why are you with Brooke?”
“'Cause she doesn't want to be alone with you.” Jo says bravely causing Paul to chuckle lightly, “Oh, why am I not surprised that you tried to poison her while I wasn't even able to defend myself?”
“The only toxic substance in this room is you.” I tell him not caring if I get heard from people outside.
Paul inhales angrily, “Jenny, get my stuff. I'm not staying here.”
Jenny doesn’t back down, “No.”
Paul pauses at her refusal and I can tell he’s getting angry but he’s too smart to let it show, “Babe. I'm really trying here, but you got to meet me halfway. I know I'm not perfect. You are way closer to that than I am. But, please, can we just leave this place and not look back? We have a wedding to plan.”
Jenny exhales sharply before responding, “You should probably call your office and let them know you're gonna be gone for a few days.”
Paul grins, “That's my girl.”
“Or, like, to years.” I grin slightly at Jenny’s cold statement and revel in Paul’s shocked face.
“What?”
Jenny explains, “I'm gonna talk to the police, Paul. I'm gonna tell them every time you ever hurt me. Every kick, every slap. You put your hands around my throat last night, so that's not just domestic violence. That's attempted murder. And I’ll tell them you used my email this morning to send Amber’s file to her bosses after you hired someone to hack her.” She turns to us, “Will you two testify?”
“Yes.” Jo replies.
I nod, “Absolutely.”
“You sound crazy.” We all deny Paul’s accusation, “Jenny, I'm a well-known physician, and you're…nobody. All you're gonna do is throw your career in the garbage. No one's gonna hire someone they don't trust.
Jenny doesn’t get scared, “No, I'm not gonna let you scare me into backing down again.”
“Scare you?” Paul asks appalled, “I'm the one who should be scared. You're threatening me in a hospital bed. I-I'm defenseless.” I shake my head at him playing the victim to get Jenny to be his punching bag, “Please. Can we just talk?”
Jenny looks broken for a moment before regaining her stance, “Some very broken part of me still loves you, Paul, but let me be very clear. I am never speaking to you again unless it's from a witness stand.”
Paul’s face scrunches in anger, “You stupid bitch.” I look at him blankly not affected by his insult, “You're not going to the police!” He moves to get off the bed and I move fast as does Meredith. We pull Jo and Jenny back as they shriek in fear at Paul moving to attack, “You're not walking out on me!”
Suddenly Paul trips and hits his head on the foot end so fast it takes me a moment to process his unconscious body on the floor. Despite my shock I keep Jo and Jenny back as Grey carefully checks Paul’s pulse and looks up.
“His pulse is thready and he’s not breathing. We should get a crash cart in here.” I gasp at the prognosis and keep still even as Jo moves to get a crash cart.
#greys anatomy#amber karev#alex karev#jo wilson#elizabeth gillies#andrew deluca#liz gillies#headcanon#giacomo gianniotti
3 notes
·
View notes
Last Seen Blogs

flowercrownexo
i think i like it

jebitz
Jebitz

soft-behind
Non-nude Curve Appreciation

driedbaby
Want to start a fight?

ursa-mediocre
ヽ(o`皿′o)ノ