#intestinal malrotation
Text
Students with food intolerances deserve a safe, free lunch too. Failing to provide that because you think it’s unnecessary is just ableism. “Eating this food causes them pain because their body can’t digest it, but it’s not life threatening so we don’t need to accommodate it” is such a bad take. Yes, let’s just make them sick every day instead of giving them the option of safe, free foods to eat. So poor kids will have to choose every day if they’re going to starve themselves or if they’re going to be in excruciating pain the rest of the day when they’re trying to learn. Makes no sense.
Furthermore, I don’t think people realize what food intolerances entail. It’s not just, “oh, eating this food gives me a stomach ache.” It is often caused by the body’s inability to break down the sugars in the food because the pancreas and/or the small intestine doesn’t make enough digestive enzymes. People with food intolerances can have a number of disabling conditions, especially because of malnutrition and malabsorption. I am dependent on digestive enzyme supplements, as well as vitamins because I can’t eat and/or get the nutrition I need to thrive without them. This is disabling. Yes, even if it’s not going to immediately kill me if I eat the wrong thing.
Don’t put people in places where they’re required to work, promising that food will be provided for free, and then only provide foods that will make them sick.
#food intolerance#lactose intolerance#ibs d#ibs c#intestinal malrotation#gerd#silent reflux#digestive disorders#ableism#text post
533 notes
·
View notes
Text
Here’s a list of things I keep in my Chronic IllnessTM go-bag.
I have GERD, Intestinal Malrotation, IBS-D, B12 Deficiency, No Gallbladder, and Abdominal Adhesions so my bag is more focused on my messed up digestive/nervous system. I bring my bag with me most places because I struggle to make it through a single week without a flare up of some kind. It cost a lot up front for me to put together, but I really can’t imagine functioning without this now and it’s easy to replace the stuff I use.
Totally recommend it if you’re chronically ill, and I recommend these particular things if you have any of the same conditions as me.
Food Items/Supplements:
BelliWelli Bars - They were developed by someone with IBS. They have probiotics. I usually can’t tolerate probiotic products, but these are also low FODMAP so I can digest them pretty easy. Not available in stores yet. I bought this online from their store. I recommend the Cookies and Crème, Strawberry Shortcake, and Lemon White Chocolate.
Liquid IV - I get extremely dehydrated because of IBS-D which then causes dizziness and tachycardia. This is a hydration multiplier / electrolyte mix you add to water. You can get this at the supermarket.
Powerade - I drink these regularly. Again, I need electrolytes because of IBS-D. I also need B-12 and Powerade contains B-12. You can get this at the supermarket.
Gin-Gins - These are chewy ginger candies. I get nauseous easily. Ginger helps, and these taste pretty good. They have different flavors. The peanut ginger chews are really good. You can get this at the supermarket.
Olly Goodbye Stress gummies - I have anxiety which makes my IBS-D worse and vice versa. My coworker gave me one of these and they did help, so I got a small 10 count bag of them. You can get this at the supermarket, and some retail stores like Old Navy.
B12 Awake Patches - These go on the inside of your wrist or the top of your foot. It definitely works on keeping me awake. The only problem is I get contact dermatitis from putting it on my wrist. It’s okay, but less effective on my foot. You can get this at Target or Ulta.
Clothing Items:
Blisslets - These are fashionable acupressure bracelets. Seabands also work and they’re less expensive, but they’re very obviously nausea bracelets. These are discrete. They really help me avoid nausea without medication.
I keep a change of clothes. T-Shirt and underwear from Aerie. Linen pants from Old Navy. Loose fitting comfortable clothes are important to have if you have digestive health problems. Aerie has comfortable clothing and they’ve been working on inclusive clothes. Aerie also sells period underwear that is less expensive than major brands. I have those in my bag as well.
Bathroom and Hygiene Items:
Public bathrooms can suck, but they’re necessary.
Soap Strips - I got a container of these from the travel section of 5 Below. These are strips of paper-like soap that you can use when there’s no hand soap available.
Poo Pourri Toilet Spray - We all know going to the bathroom stinks literally and figuratively. If you’re concerned about making a stink, I recommend this. I’m very sensitive to smells so it’s a must for me. You can get this in the travel section of most supermarkets.
Potty Packs - What really sucks about public bathrooms is that you can run out of toilet paper and it can be really unclean in there. My local supermarket sells these in the travel sections. They come with toilet paper, seat cover, wet wipes and hand sanitizer. They fit in a small bag or purse.
Flushable wipes - A lot of public bathrooms can’t handle wipes. So I pretty much just have these to clean my body if needed. You can get them at pretty much any supermarket.
Crest Scope Minibrushes - You can find these in the travel section of most supermarkets. Helps keep your mouth clean, especially if you get nauseous like I do or you need to get a bad taste out of your mouth to prevent being nauseous. They have a toothpick on them too.
Grin Floss - This is eco-conscious dental floss. You can get them in different flavors like mint, and I found these at my local supermarket.
I also keep a Wet Brush and extra hair ties to keep my hair out of my face. I separate bathroom items from other hygiene items into two oblong makeup style bags I got from Target. That way I can also take one small bag or another and transfer it to my main bag if I don’t want or need my whole go-bag with me.
I keep two pill containers that are divided into large and small sections I can label with an erasable marker. I got them off Etsy. I won’t list all my supplements / medications because what I need to take isn’t going to be the same as everyone else and I’m no one’s doctor.
Finally, I keep fidget things in my bag to reduce my anxiety!
#gerd#acid reflux#silent reflux#ibs#ibs d#intestinal malrotation#nausea#bppv#b12 deficiency#chronic illness
42 notes
·
View notes
Text
Got a referral for a super invasive procedure for my deformed insides. Honestly I worry about it because I desperately want a gender affirming salpingo-oophorectomy and Im worried my chronic illness will prevent me from getting it.
0 notes
Text
ETB 40: Finding Quality Care for Your Special Needs Child with Gerrie Bourque
ETB 40: Finding Quality Care for Your Special Needs Child with Gerrie Bourque
ETB 40 – In this episode I talk with Gerrie Bourque, mother of 3 whose 26 year old son Tyler has a dual diagnosis of Down syndrome and autism, is medically complex and has rare disorders. Gerrie shares the various caregiving options they have explored over the years.
Tyler has a Texas Medicaid Waiver which provides services for him including a support staff to care for him as needed. Initially,…
View On WordPress
#Attendant Care#autism#Care.com#caregivers#Down syndrome#dual diagnosis#host family home#Next Step Transition Center#support staff#Tyler&039;s story; Recovering from intestinal malrotation#Verne Cox Center
0 notes
Text
"I have something really funny for you actually that I wanted to promote on here. I almost died two years ago and it was from a rare birth defect called Intestinal Malrotation and its where, what can happen is your intestines twist in whats called a volvulus and I survived this four times and I was misdiagnosed every time and the only reason I survived is because basically we pushed and kept asking and then I had surgery which saved my life and since then i've been trying to start a charity because there aren't really any that exist and just recently I partnered with the children's hospital in LA and they're going to start a fundraiser where if we get 125k, they'll create a fellow for this"
- Jack on his charity for Intestinal Malrotation with the LA children's hospital.
36 notes
·
View notes
Link
0 notes
Text
Unraveling the Mystery of Intestinal Nonrotation and Cecal Volvulus: A Rare and Fascinating Medical Marvel

Unraveling the Mystery of Intestinal Nonrotation and Cecal Volvulus: A Rare and Fascinating Medical Marvel
# Unraveling the Mystery of Intestinal Nonrotation and Cecal Volvulus: A Rare and Fascinating Medical Marvel #
Introduction
Have you ever heard of intestinal nonrotation and cecal volvulus? Chances are, you haven't. These are two rare medical conditions that affect the gastrointestinal tract, leading to a host of symptoms that can be difficult to diagnose and treat. In this article, we will delve into the intricacies of these conditions, exploring what causes them, how they present, and some potential treatment options.
Unraveling the Mystery of Intestinal Nonrotation and Cecal Volvulus: What are They?
Intestinal nonrotation is a condition where the intestines fail to rotate properly during fetal development. Normally, the intestines rotate and organize themselves into a specific configuration, but in cases of nonrotation, this does not happen. This can lead to a host of issues, including malrotation of the intestines, twisting or blockage of the bowel, and even volvulus.
Volvulus, in turn, is a condition where a portion of the bowel becomes twisted or blocked, compromising blood flow and leading to severe pain, nausea, and other symptoms. One specific type of volvulus, cecal volvulus, affects the cecum, a pouch-like structure in the large intestine. This can lead to severe abdominal pain, distension, and even bowel ischemia, which can be life-threatening if not treated promptly.
Causes of Intestinal Nonrotation and Cecal Volvulus
There is no clear consensus on what causes intestinal nonrotation and cecal volvulus, but several risk factors may increase the likelihood of developing these conditions. For example, fetal development issues, infections, and genetic factors may all contribute to the development of intestinal malrotation or volvulus.
Other factors, such as previous abdominal surgery, adhesions, or gastrointestinal disorders, may also play a role in the development of these conditions. In some cases, trauma or injury to the abdomen can lead to twisting or blockage of the bowel, which can ultimately result in volvulus.
Symptoms of Intestinal Nonrotation and Cecal Volvulus
The symptoms of intestinal nonrotation and cecal volvulus can be highly variable, but some common signs that may indicate the presence of one of these conditions include:
- Severe abdominal pain, particularly in the right lower quadrant
- Nausea and vomiting
- Bloated feeling or abdominal distension
- Constipation or difficulty passing gas
- Bloody stools or other gastrointestinal bleeding
In some cases, individuals with intestinal nonrotation or volvulus may present with fever or other signs of infection. However, the symptoms of these conditions can be highly variable, and some people may not experience any symptoms at all.
Diagnosis and Treatment of Intestinal Nonrotation and Cecal Volvulus
Diagnosis of intestinal nonrotation or cecal volvulus typically involves a combination of physical examination, imaging studies, and lab tests. Your doctor may perform a detailed abdominal examination to assess for tenderness, distension, or other signs of bowel obstruction.
Imaging studies, such as X-rays, CT scans, or ultrasound, may also be used to visualize the gastrointestinal tract and assess for any abnormalities. Blood tests can help detect signs of infection or inflammation, which may indicate the presence of volvulus or nonrotation.
Treatment for intestinal nonrotation or cecal volvulus may involve surgical intervention to correct the underlying abnormality. Your surgeon may perform a surgical procedure called an Ladd's procedure, which involves repositioning the intestines to prevent twisting and blockage of the bowel.
In some cases, surgery may not be necessary, and conservative measures such as bowel rest, fluid replacement, and pain management may be sufficient. However, in cases of severe volvulus or nonrotation, surgery may be essential to prevent life-threatening complications.
FAQs
Q. Can intestinal nonrotation or cecal volvulus be prevented?
There is no clear way to prevent intestinal nonrotation or cecal volvulus, as the underlying causes of these conditions are not well understood.
Q. What is the typical prognosis for individuals with intestinal nonrotation or cecal volvulus?
With prompt diagnosis and treatment, individuals with these conditions may have a good prognosis. However, delays in diagnosis or treatment can lead to severe complications, such as bowel ischemia, and may even be life-threatening.
Q. Are there any long-term complications associated with these conditions?
In some cases, individuals with intestinal nonrotation or cecal volvulus may develop chronic gastrointestinal issues, such as bowel obstruction, chronic pain, or other complications. However, the long-term prognosis for these conditions is highly variable and depends on a range of individual factors.
Q. Is surgery the only treatment for nonrotation or cecal volvulus?
In some cases, conservative management may be sufficient to manage symptoms and prevent complications. However, surgical intervention is typically required to correct the underlying abnormality and prevent recurrence of the condition.
Q. Are there any lifestyle modifications that can help manage symptoms of nonrotation or cecal volvulus?
While there are no specific lifestyle modifications that can treat these conditions, maintaining a healthy diet, staying hydrated, and managing stress may help to prevent exacerbation of symptoms.
Q. How often do nonrotation or cecal volvulus occur?
These conditions are relatively rare, occurring in only a small percentage of the population. However, they can be highly debilitating and require prompt diagnosis and treatment to prevent complications.
Conclusion
Intestinal nonrotation and cecal volvulus are two rare and fascinating medical conditions that affect the gastrointestinal tract. While their underlying causes are not well understood, a variety of risk factors may contribute to their development. With prompt diagnosis and treatment, individuals with these conditions can often make a full recovery, but delays in diagnosis or treatment can lead to severe complications. If you suspect that you or a loved one may be experiencing symptoms of intestinal nonrotation or cecal volvulus, speak to your doctor as soon as possible to explore potential treatment options. #HEALTH
Read the full article
0 notes
Text
Best pediatrician near me
Visiting Dr.Aggarwal's wellness multi-specialty hospital where you'll get the best pediatrics doctor in Yamuna Vihar which is The core of the medical specialty known as pediatrics is the surgical care of infants, kids, and teenagers. Pediatric surgeons are the medical professionals carrying out these procedures after creating a pre-operative strategy based on the patient's outcomes. The following common pediatric illnesses may necessitate pediatric surgery: Intestinal atresia, necrotizing enterocolitis, meconium plugs, lymphangiomas, cleft lips and palates, esophageal atresia, and tracheoesophageal fistulas, hypertrophic pyloric stenosis, Hirschsprung's disease, Imperforate anus, undescended testes, and intestinal malrotation are examples of congenital malformations. Children's obstetrical tumors, gastroschisis, and hernias include neuroblastoma, Wilms' tumor, ATRT, and liver tumors, among others. Take advice from the best pediatrician in Yamuna Vihar, Delhi.
0 notes
Text
Diet culture hurts chronically ill and disabled people with dietary restrictions because it prioritizes weight loss over health needs.
The majority of "diet apps" I have tried ask me for my weight and weight loss goals, when I need to track my diet for complex medical reasons.
The majority of books in the dietary health section focus on weight loss. There are maybe a couple books out of 100 focused on my condition(s).
Even some of the informational materials and the products that do cater to my condition(s) emphasize weight loss over health needs.
When I ask for dietary accommodations, people ask invasive questions as to why I need it to suss out if I really need it or if I'm just "on a diet."
Even in medicine, weight gain or loss is emphasized over actual nutrition. If you're not at risk of heart disease or "obesity," it's like they do not care.
I could barely eat anything when I was hospitalized because the hospital menu did not account for my specific dietary needs. A damn hospital.
I've been offered the most non-nutritious diet plans and given little to no guidance on my condition(s) by actual doctors who study my condition(s).
So, tell me why there are thousands of diet plans for weight loss but few resources for people like me who end up sicker with vitamin deficiencies.
Tell me why I have to join groups specific to people with my condition(s) just to figure out how to thrive because no one helps us but our own people.
Diet culture is ableist, and diet culture disables people. Diet culture should be about helping people like me thrive, but it's doing the opposite.
This is about accessibility. Diet is ultimately an accessibility issue, and society disables us by not caring if we eat safely or eat at all.
#diet culture#disability#chronic illness#intestinal malrotation#cholecystectomy#cholecystitis#silent reflux#GERD#ibs#b12 deficiency#i still need to get tested for SIBO#but i am fairly certain it's caused my IBS
470 notes
·
View notes
Text
A case report of Midgut Volvulus with Perforation in a Pre-Term Baby
Abstract: Midgut Volvulus (MV) is a life-threatening surgical emergency. The most common causes include malrotation and intestinal atresia. Volvulus can present at any age, but typically presents within the first few days of life. Unrecognized MV leads to bowel ischemia and varying degrees of bowel necrosis with perforation. We herein report the case of a preterm baby of 33 weeks and 5 days at 36 hours of life, with Midgut Volvulus and intestinal perforation.
Case: A preterm male neonate was delivered by emergency LSCS at 33 weeks and 5 days of gestation with birth weight of 1.54 kg. It was a Twin pregnancy with mother having a history of premature onset of labour and bleeding per vagina. Mother received incomplete course of antenatal corticosteroids. Baby had a weak cry on birth and soon developed respiratory distress so was put on CPAP. His APGAR scores were 7 and 8 at 1 minute and 5 minutes respectively.
Baby was started on IV fluid and IV antibiotics (Inj Cefotaxim and Inj Amikacin) after sending sepsis screen and blood culture/sensitivity. Baby was kept Nil per orally as the abdomen was slightly distended and had not passed stool since birth. At 36 hours of life, there was sudden gross abdominal distension with bluish discoloration of overlying skin (Fig 1 & 2) and baby went in shock.
Baby was intubated and kept on SIMV ventilation. IV inotropes (Dopamine and Dobutamine) started through Central line (PICC line). Immediate X-ray abdomen done which revealed dilated bowel loops and no air in the rectum (Fig 3)
Opinion of Pediatric Surgeon was sought subsequent to which emergency Exploratory Laparotomy was done in suspicion of intestinal obstruction secondary to intestinal atresia. The findings during surgery were Midgut volvulus with gangrene of approx 80 cm of small intestine with perforation.
The surgical procedure was derotation of the gut with resection of gangrenous small bowel (80 cm) with double barrel stoma formation. The baby remained hemodynamically stable throughout surgery. Post operation baby was kept on SIMV ventilation with inotropes & IV antibiotics and Total Parenteral Nutrition started. Baby weaned from mechanical ventilation to HFNC in next 72 hours. IV inotropes was gradually stopped by Post-Op Day 4. Trophic feeds started on Post-Op Day 5 which was well tolerated. Baby was finally off ventilatory support on Post-Op Day 11. Full enteral feeds was achieved by Day 28. The baby developed Short Bowel Syndrome as a result of resection of major portion of small intestine. This was managed by starting special formula feed (Amino Acid based Hypoallergenic infant formula), giving Vitamin/Mineral supplments, using Antaacids and introducing small & frequent feeds. The baby started gaining weight. Stoma care was done throughout the stay.
Baby was discharged at corrected gestational age of 37 weeks & 5 days with weight 1.780 kg. Mother was counselled about stoma care, briefed about feeding frequency and amount and regular follow up was advised.
Second surgery was done which was stoma closure at the age of 5 months. The baby was on regular followup. Management of Short Bowel Syndrome was quite challenging but with conservative management, the baby was able to achieve normal growth
Discussion:
Midgut Volvulus is a surgical emergency condition in which the intestine has become twisted as a result of malrotation of the intestine during fetal development. Malrotation of the intestine occurs when the normal embryologic sequence of bowel development and fixation is interrupted.
The possibility of Midgut Volvulus should be included in the differential diagnosis of preterm babies presenting with sign and symptoms of Necrotizing Enterocolitis or feeding intolerance even in the absence of bilious emesis.
Since the entire midgut is potentially at risk for vascular compromise with volvulus, it is best to make the diagnosis at the onset of symptoms and signs of obstruction before symptoms and signs of intestinal ischemia develops. In our case, the baby had Midgut Volvulus with gangrene and perforation which required resection of major portion of small intestine resulting in Short Bowel Syndrome.
Upon confirmation of the diagnosis, the operation of choice is a Ladd procedure that consists of untwisting the volvulized bowel, dividing abnormal bands, broadening of the mesentery and arranging the bowel. An algorithm indicating the approach for differential diagnosis of acute abdomen in neonates is given under Fig 8.
Algorithm
Midgut Volvulus with perforation is a rare and often misdiagnosed entity in preterm infants. Although prevalence is unknown, morbidity and mortality have remained high in the cases that have been reported. Prompt recognition and surgical intervention in preterm infants may reduce the mortality and morbidity seen in the NICU. Volvulus should be considered a possible diagnosis in otherwise healthy preterm infants with signs of an acute abdomen and respiratory distress.
Conclusion: Midgut Volvulus with perforation is a rare and often misdiagnosed entity in preterm infants. Although prevalence is unknown, morbidity and mortality have remained high in the cases that have been reported. Prompt recognition and surgical intervention in preterm infants may reduce the mortality and morbidity seen in the NICU. Volvulus should be considered a possible diagnosis in otherwise healthy preterm infants with signs of an acute abdomen and respiratory distress.
References:
1. Horsch S, Albayrak B, Tröbs R-B, Roll C. Volvulus in term and preterm infants - clinical presentation and outcome. Acta Paediatr Oslo Nor. 2016;105:623–7.
2. Langer JC. Intestinal rotation abnormalities and midgut volvulus. Surg Clin North Am 2017; 97: 147–59.
3. Kanellos-Becker I, Bergholz R, Reinshagen K, Boettcher M. Early prediction of complex midgut volvulus in neonates and infants. Pediatr Surg Int. 2014;30:579–86.
4. Gilbertson-Dahdal DL, Dutta S, Varich LJ, Barth RA. Neonatal malrotation with midgut volvulus mimicking duodenal atresia. Am J Roentgenol. 2009;192(5):1269–1271
5. Stephen D.AdamsMichael P.Stanton. Malrotation and intestinal atresias Early Human Development Volume 90, Issue 12, December 2014, Pages 921-925
6. Vinocur DN, Lee EY, Eisenberg RL. Neonatal intestinal obstruction. AJR Am J Roentgenol. 2012;198(1):W1–W10.
7. James Goodwin Glasser, MD, MA, FACS Pediatric Surgeon Intestinal Obstruction in the Newborn Differential Diagnoses Pediatrics: Cardiac Disease and Critical Care Medicine (Medscape updated Feb 20, 2021)
8. Georgeson K.E , Breaux Jr., C.W. et al.Outcome and intestinal adaptation in neonatal short-bowel syndrome. J Pediatr Surg. 1992; 27: 344-350
#Midgut Volvulus#Intestinal Perforation#Intestinal Ischemia (Gangrene)#Malrotation#Short Bowel Syndrome
1 note
·
View note
Text
A normal morning routine:
Wake up
Go to bathroom
Brush teeth
Get changed
Eat breakfast
Drive to work
Proceed to work day routine
My morning routine:
Wake up
Feel dizzy/nauseous/abdominal pain
Lay back down
Sit up/Drink water
Stand up
Go to bathroom
Brush teeth
Feel dizzy/nauseous/abdominal pain
Lay back down
Go to bathroom
Get changed
Feel abdominal pain
Go to bathroom
(Can't eat)
Drive to work
Feel abdominal pain
Stop to go to the bathroom
Continue driving to work
Get to work
Go to bathroom x3
Proceed to work day routine
7 notes
·
View notes
Text

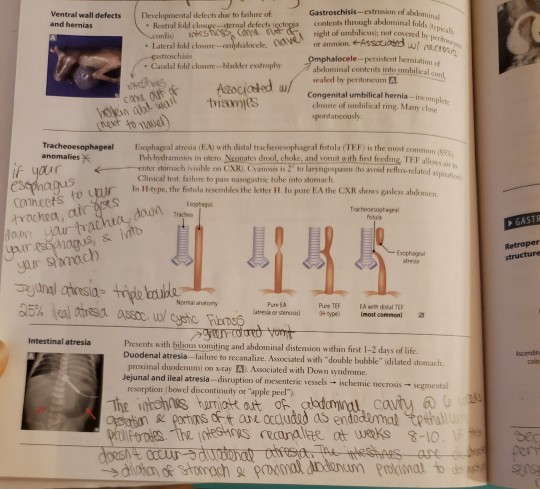
So the first thing I learned regarding double bubble sign is duodenal atresia. But double bubble sign can be different things depending on what you see in addition to double bubble sign.
I think I recall a scholar saying that bilious emesis in a newborn is malrotation until proven otherwise.
So basically, if a newborn is vomiting bile, do this workup.
So I'm looking at First Aid for USMLE Step 1 and it says double bubble is the dilated stomach and proximal jejunum seen in intestinal atresia, specifically in duodenal atresia. So in the OnlineMedEd video, he groups things differently from how First Aid does it. I think the First Aid book is more accurate:
Intestinal atresia is either duodenal atresia or jejunal and ileal atresia. In duodenal atresia, the duodenum doesn't recanalize, so you get double bubble sign on X-ray. In jejunal and ileal atresia, those parts of the small intestine are infarcted, showing bowel discontinuity or "apple peel" because these parts of bowel aren't being perfused, so the become necrotic.
#double bubble#duodenal atresia#intestinal atresia#malrotation#bilious vomit#green vomit#bilious emesis#biliary atresia
1 note
·
View note
Note
If you dont mind me asking what do you mean your organs were at the wrong place
It’s called intestinal malrotation, when I was born my intestines were twisted up wrong, so as I kept growing they would have kept getting more messed up. If it hadn’t been found by chance while I was a baby, it would have caused major problems when I was around 12 and probably would have killed me because that’s not something they would have thought to check for
They only found it because I would randomly stop breathing as a baby lol
#unrelated i’m p sure#that’s also when i got my appendix taken out#i think my appendix was on the wrong side or something?#ask#anonymous#sepulchritudinous
21 notes
·
View notes
Text
Jacks Intestinal Malrotation fundraiser!!
15 notes
·
View notes
Note
You were in and out of a hospital as a kid too? Do you mind if this anon asks why and if you’re all better now?💟💟💟💟💟
i have crohn’s disease! before the diagnosis i had a malrotation of the intestine which basically means my guts were knotted like spaghetti and i couldn’t poop to save my life kjasldkfj. lots of stays trying to figure out meds, sorting things out when meds made things worse, flare ups and regular surgeries to help out with restrictive scar tissue. it’s a chronic illness so it’ll never quite go away but i’ve been in remission for the most part since around 2017! i take a monthly immunosuppressive drug that helps my body not try to kill itself along with dilations and so far the mix has been doing well and i feel good most days!
we’re both hospital kids?! if you’re comfy sharing could i ask why you were in and how you’ve been doing since?
#toffee talks#💟 anon#hospital kids are built different#we know our bodies more than the doctors do kajsldfjads#twice a year i get anally probed by a metal rod and i think that;s pretty kinky#need to make a tag for oversharing irl stuff lkjdflkjs one day
2 notes
·
View notes
Last Seen Blogs

livvylubug
No Sleep, Just Art

pervbatorbro
PervBatorBro

fennkine
Sup, I exist I guess

digitalmarketingstrategies101
Digital Marketing Strategies 101

angelaterry
Random