#dysthymic disorder
Text
turns out i've been diagnosed with Dysthymic Disorder since 2017 and i didnt even know it
0 notes
Text
Ah lads it’s the sorrows again
#Sad Bitch Sometimes Syndrome strikes again#technically it's called persistent dysthymic disorder#but I like my name for it better
18 notes
·
View notes
Text

So tired of it being treated like it is
#art#artwork#digital art#drawing#digital artwork#digital media#furry art#drawings#vent art#furry#bpd#borderline personality disorder#borderline#dysthymic#dysthymia#adhd#attention deficit hyperactivity disorder#cptsd#ptsd#complex post traumatic stress disorder#post traumatic stress disorder
7 notes
·
View notes
Text
looking at my medical charts from the past 10 years and finding a strange diagnosis and it turns out they just wanted a new word for depression
1 note
·
View note
Text
Levi, Emotional Expression, and Social Interaction
I've seen different posts on Levi lately across different platforms that claim he is a cruel or mean person, which are fundamental misunderstandings of his character. I sort of see the problem as people mistaking Levi's emotional expressions (or lack thereof) as indicative of malicious intent or rude behavior. As such, I wanted to discuss how Levi's history and trauma have shaped how he expresses himself and relates to others. Once one has an understanding of that, it becomes evident that Levi's expressions should not be used to judge his intentions or feelings.
I wrote another post on how Levi fully meets the criteria for post-traumatic stress disorder (PTSD) on my main blog, and that diagnosis is important for understanding Levi as a character, as he's someone who's been largely affected by his trauma. To further expand on that post, we're going to discuss both Levi's affect and his ways of socially interacting with others, using concepts such as social modeling and self-monitoring.
What is Emotional Affect?
Affect, in psychology, refers to a patient's expression of emotion. Expression of emotion encompasses facial expressions, gestures, body language, tone of voice, etc. Mood, on the other hand, refers to the internal state of a patient's emotions sustained over a period of time. Affect helps us interpret a person's mood; however, there are such situations where affect can be considered inappropriate—that is, the person's affect is not entirely congruent (i.e., consistent) with the person's present mood and/or situation. A classic example of inappropriate affect would be laughing at a funeral, as that is incongruent with the context of the situation. Another example—a patient who is smiling and laughing after being involuntarily committed is considered to have an inappropriately euphoric affect.
Affect can be described across multiple dimensions, but the two most typically used are the quality of affect and the range of affect. Quality of affect is typically categorized as either euthymic (normal), dysthymic (depression, anxiety, guilt), or euphoric (an abnormally elevated sense of well-being, such as in mania). The range of affect can be labeled as labile, broad, restricted, blunted, or flat. Broad is considered the normal range of affect.
For the purposes of conciseness, we're going to focus on blunted and flat affects, as those are the range of affects that are best suited to describing Levi. Flat affect is when there is no variation in the patient's emotional expressions, regardless of their mood and situation. Blunted affect is similar, but it is a bit less severe—it means minimal variation. Practically, what do these mean?
Levi's Affect
When Kenny first finds Levi as a child, Levi is in a severe state of neglect; he is dying of starvation, he is wearing rags, his hair is unkempt, and he is sitting in the same room as his mother's decaying corpse. A typical child in this developmental range would be in extreme distress: crying, expressing fear, pleading for help, etc. However, Levi shows no such displays of emotions; he does not cry, he does not move, and he barely speaks. In fact, there is absolutely zero emotional expression, and there is no indicator he is upset about his situation (even as it is clear he must be). This is flat affect. Even in the short montage we see after Kenny has taken Levi under his "care", Levi never once shows variation in his emotional expression—no anger, no laugher, nothing.
Once Levi is an adult during the present timeline in the series, Levi exceedingly rarely displays his emotions. He often speaks in monotone, minimally varying the tone or volume of his voice—never yelling as well, even when angry. His smiles are so rare that it's a notable moment when he does smile (such as when Historia punched him at end of the "Royal Government" arc), and he never cries even after significant personal losses (except his one tear at the end of the series). His affect as an adult ranges from flat to blunted. This is significant too because we do know that his mood does vary, as it's clear from his verbal and body language the toll that different events take on him, and he does also display a sense of humor across the series. Again, though, his emotional expression does little to reflect how he's feeling.
What Causes Flat Affect?
To give a quick list of the most common causes:
Schizophrenia and other psychotic-spectrum disorders
Brain damage, such as from organic brain pathology or a traumatic brain injury
Neurodevelopmental disorders, such as autism spectrum disorder (ASD)
Severe psychological trauma, typically resulting in post-traumatic stress disorder
Major Depressive Disorder (MDD)
I will say outright that there is no evidence Levi suffers from schizophrenia, and thus, that is unlikely to be the cause of his flat/blunted affect, especially given the onset of Levi's flat affect and the exceeding rarity of childhood-onset schizophrenia. Similar reasoning applies to brain damage, so both of those can be excluded from the differential.
I do believe Levi meets the criteria for MDD in adulthood; however, that would be more so a comorbidity of his existing PTSD. Levi looked to be around 4-6 years of age at the start of Kenny's flashbacks, and MDD in that age group is quite uncommon, even when accounting for childhood-onset and adolescent-onset depression.
This leaves us with both severe psychological trauma and ASD as the two most likely causes of Levi's flat affect as a child and through adulthood. ASD can be a valid interpretation of Levi's significantly reduced affect display during childhood, as well as his consistent social difficulties throughout all of canon. Based on criteria laid out by the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR), Levi can be seen as having ASD (which I'll likely make a future post on). However, the presence of severe psychological trauma confounds this diagnosis. Despite this confounding diagnosis, it is still possible he has both PTSD and ASD.
Regardless, the most likely explanation for Levi's range of affect remains severe psychological trauma. In a child that young, something had to have gone extremely wrong in his early upbringing for his significantly reduced affect display. An entire separate post can be written on this topic, but Levi demonstrates clear signs of an insecure attachment style by the time he's discovered by Kenny; this indicates that Kuchel, despite having loved Levi, was simply unable to properly care for him, and this resulted in deep and ingrained psychological trauma that affected Levi's ability to socially relate and interact with others for the rest of his life. I intend on going into more detail in a separate post, but Levi's attachment style is likely insecure-avoidant or insecure-disorganized.
Observational Learning and Social Modeling
Albert Bandura's social learning theory posits that children learn through a combination of traditional behaviorist processes (classical and operant conditioning), cognitive processes, in addition to observation and modeling. In reference to Levi, observational learning is the most salient aspect of this theory.
In simple terms, observational learning refers to the way children observe the people around them. Individuals observed are referred to as models. Models can include, but are not limited to, parents/caregivers, TV characters, school teachers, and friends within a peer group. Basically, children pay attention to these models and encode their behavior into their memory. At a later time, this behavior is then imitated. This is referred to as "social modeling".
Who were Levi's models? Kuchel, Kuchel's patrons at the brothel she worked at, Kenny, and others who lived in or frequented the Underground City.
Given Kuchel's circumstances and the danger of human trafficking in the Underground, it is likely she taught Levi to avoid interacting with anyone in order to ensure his safety. Kuchel's patrons, in all likelihood, abused her and Levi was most assuredly witness to this abuse or the effects of it in some way. Then, Kenny—Levi's most significant parental figure—was a prominent serial killer who displayed and actively taught Levi violence.
All of this points to Levi never having had the opportunity to learn proper social interaction. In fact, he was actively taught inappropriate and unhealthy ways to socially interact. Not only was Levi's emotional development stunted and severely impacted as shown through his lack of affect, but his ability to socially interact and relate to others was inhibited due to both his insecure attachment and the absence of appropriate social models. How does this manifest in Levi?
Self-Monitoring
Self-monitoring is the degree to which people monitor and adjust their self-presentations when interacting with others and across different social contexts. Whether someone is a high or low self monitor can be affected by their natural personality, their experiences growing up, and/or their neuropsychobiology.
High self monitors tend to be actively aware of the social image they are projecting, and they will be adept at responding to social cues. They will also vary the image they project dependent upon who they are interacting with and what the social circumstances are. They have greater concern over situational appropriateness, and they are often perceived as more friendly and pleasant by others.
In contrast, low self monitors tend to exhibit emotional expressiveness and social responses more congruent with their internal states regardless of social context. That is, they do not adjust their beliefs, attitudes, and dispositions to be more socially acceptable. As such, they are often perceived as rude, socially awkward, and/or unaware of others' social needs.
Levi is a low self monitor. Regardless of who he is interacting with or what the situation is, he consistently maintains the same attitudes and beliefs; he is always honest and says what he's feeling. He never adjusts his social tone, even when it would make him more appeasing to others. Throughout the series, he's often referred to as rude, socially awkward, a lunatic, etc. for his inability to self-monitor. This is a likely a result of the aforementioned psychological trauma, his lack of appropriate social models, his innate introverted nature, and his potential ASD.
Summary
My goal with this post was to explain how Levi's trauma and experiences growing up have formed the way he expresses himself and interacts with others. Levi never sets out to be seen as rude, unkind, or cruel. In fact, I'd say he is by far the kindest and most compassionate character in all of Attack on Titan. However, because of his social disposition, he is consistently misperceived by both characters in the series, as well as readers/viewers. Levi, through a combination of his innate nature and the environment in which he grew up, simply lacks the social skills and affinity for social interaction to properly explain himself and come across as more palatable to others.
Note: I am a doctor of psychology student, so much of this information has been informed by my schooling.
#attack on titan#shingeki no kyojin#levi ackerman#aot#snk#attack on titan meta#shingeki no kyojin meta#Levi Ackerman meta#aot.text#aot.meta#my thoughts#c: levi ackerman#meta.levi#text.levi
118 notes
·
View notes
Text
Aziraphale Does NOT Have Depression
or: Please Have a Look at the ICD
or: This Word Does Not Mean What You Think It Does
I cannot believe I even have to make this post, but here we are. Hi. Hello guys. Maybe I should start a series called "Alex fact-checks meta posts" because I have seen things that should have never been written.
A small excursion before we start: The way things usually work in academic circles is that the person making the claim needs to provide proof for said claim, which is then peer-reviewed by unrelated academic parties. That involves not only making sure that the results they are basing their claim on are replicable—meaning that if someone else were to do the same work, they would receive the same result—but also that their methods were ethical and functional.
If it turns out that their methods or any other part of the process are not replicable, functional, or otherwise waterproof, then the paper is marked as not being correct and that it should be disregarded.
While this is far from academic circles, these rules still apply to any kind of conversation or discussion, especially that last part:
If you make a claim, back it up, or it should be disregarded.
With that, welcome to the peer-review of "Aziraphale has depression" claims. Obligatory note that this is not about fanfiction or headcanons but people claiming that Aziraphale canonically has depression.
You may sit in front of your screen and think Alex, why do you think you can write this post? To which I happily respond that not only am I professionally diagnosed with both Dysthymia and Recurrent Depressive Disorder, I have also a) done my research offline with psychiatrists and psychologists and b) know how to read academic literature because my degree very much requires me to be able to do so.
If you want to go and fact-check what I am about to present—which you are explicitly invited to do in case you want to publicly disagree with me—you can find the entirety of the ICD 11 right here.
No paywall, completely free access.
For those who have never heard of it, ICD stands for "International Classification of Diseases", which is by now on its 11th version and written and maintained by the WHO/World Health Organization. It contains all kinds of relevant information, like diagnostic criteria, about all diseases. As you can see, this includes mental disorders and illnesses:

Let's get into it!
First things first, there is no such thing as "depression", that term is a colloquial reduction of a number of different disorders categorized under Mood Disorders -> Depressive Disorders. Said category also contains any and all diagnoses related to Bipolar Disorders.
"Depression" is nondescript, loose, and can mean a long list of things, and social media has diluted and romanticized its meaning. For the purpose of this post, we will have a look at the criteria for three diagnoses:
Dysthymic disorder (shortened here to dysthymia)
Single episode depressive disorder, mild ( // to single episode)
Recurrent depressive disorder, current episode mild ( // recurrent)
I assume people mean a crude mix of these when they say "depression". Both recurrent and single episode can be diagnosed with dysthymia, but they cannot be diagnosed with each other. Recurrent automatically excludes single episode as a diagnosis, which I think is obvious if you think about it.
Before we look at the symptoms themselves, here is something very important to keep in mind about diagnoses: There are two requirements that pretty much every listed disorder and illness in the ICD has.
The first is that the symptoms are not related to something else—whether that's another mental disorder, a physical illness, or simply a cultural influence. It needs to be clear that they are due to something outside of what is already known and not circumstantial.
The second one is that the present symptoms are causing significant distress and impair a person's functioning in at least two different areas of life.
Or, to put it bluntly, a disorder needs to be disordering or it isn't one.
Additionally, the severity of the displayed symptoms needs to be taken into account. If several of them are not causing any negative impact on someone's life, they are not symptoms and cannot be counted.
Now, I will very much reduce the information the ICD provides us with or we will be here forever, but it is all correct and not partial in its meaning. To keep everything neat and tidy, I created a nice, colour-coded table:
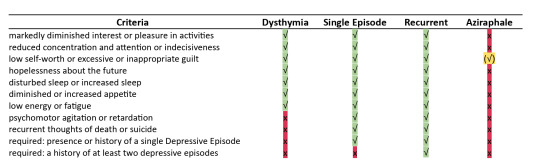
If you disagree with what I marked for Aziraphale, great, please provide me with textual evidence of where exactly he exhibits each criteria, that it is not related to periodical stress or something else, and cannot be attributed to exceptional circumstances (like the end of the world).
The ONLY symptom we ever see Aziraphale consistently show throughout all six thousand thousand years is the one marked in yellow: low self-worth or excessive or inappropriate guilt.
However, if you paid attention to what I explained above, you will notice why this is in no way indicative of a depressive disorder.
Not only is it one symptom out of several required ones, it can also be explained by something else, which is the emotional neglect and abuse heaven subjected and subjects every (former) angel to. The same can be said for any anxious symptoms he exhibits sometimes, emphasis on sometimes.
In conclusion, Aziraphale does not have depression, and I think making a case that he does will be almost entirely built on assumptions and subjective interpretations, not anything that is in any shape or form supported by text or subtext.
Does that mean all of his struggles are somehow invalid? No, of course not. They are simply not due to a disorder but something else, that's literally all this post proves. It makes no moral judgement.
#alex talks good omens#good omens meta#good omens season 2#aziraphale meta#go2#aziraphale#aziracrow#crowley x aziraphale#ineffable husbands#good omens#ineffable wives#ineffable spouses#crowley
77 notes
·
View notes
Note
hi, hope you're doing well! i know you joined the team in s2 when a lot of that groundwork was laid in s1, but what were the discussions around the portrayal of sherlock's depression/addiction like? i love how elementary seemed to portray his depression as more dysthmic especially compared to contemporary shows like You're the Worst/Bojack Horseman, though it seemed to be less of a focus in later seasons. also thanks for helping my fave show of all time come to life!
I'm fine except for the annoying covid.
We talked about Sherlock's addiction all the time, though less so about his depression. I'm not 100% sure he has depression, TBH. Maybe bipolar disorder? Whatever type of depression he may or may not have is complicated by a LOT of other issues. We always believed Sherlock's neuroatypicality was extremely atypical and thus difficult to pin down. We wrote that part of him as, well, Sherlock. Diagnose at your own peril.
That said, I can certainly see why you might see him as dysthymic. Your understanding of Sherlock's issues may vary.
And thanks for the kind words.

#ask me anything#tv writing#ask me stuff#cbs elementary#elementary#sherlock holmes#sherlock#neurodivergent#neuroatypical#depression#addiction
52 notes
·
View notes
Note
i'm sorry i'm just... figuring something out so... would you be able to talk about what internal voices "sound" like? with schizophrenia
In my case which. I am not a model for schizophrenia. I do need to note that. I am diagnosed with schizophrenia but generally have a type psychosis that worsen considerably with stress, which is described as dysthymic schizophrenia in my french diagnosis, but doesn't tend to follow the same constant severity of some of my schizophrenic peers.
So I will moreso talk about psychotic voices bc the only thing I'm certain of is that they are linked to psychosis, they might be able to happen in other disorders considering the blurriness of my own situation (I've for exemple also been diagnosed as a weird type of bipolar for a while).
Anyway, in my case, I could "hear" voices inside my head, who were very recognizably not from outside of it, I couldn't mistake it for someone talking to me. It was moreso like hearing you internal dialogue, but another voice you cannot control. I honestly interpreted it for years as a normal thing that happened to everyone due to that, and I'm not completely wrong in that assumption, as I've very much met other people, particularly commonly writers, who had voices that were semi to fully autonomous talking to them, but never seeked any diagnosis since it didn't impact their quality of life.
However in my case I had both recurring voices (characters with names and preferences, who I'll categorize as having tagged along for at least a few months) and non reccuring voices (very simplistic presences who did not have a name and were very single minded). An exemple of a recurring voice is Sunahbii, my headmate, who's an eldritch beast, is very independent, highly dislike sexual topics, etc. He feels like a person, and this is the type of voice I have that is analogous to an alter, and although they can be aggressive, they are not just so and can be reasoned. An exemple of non recurring voice could be a voice that shows up one evening to argue that someone followed me home. These voices have been practically always aggressive, cannot be reasoned, and pretty much are weird intrusive thoughts screaming at me in my brain.
The recurring type is rather rare, I've had a single one that was present since I was a young teen, Sunahbii, and around 4-5 at most in my life.
Both type of voices happen more when I'm in a psychotic state, but although I used to pretty regularly get new non recurring voices, I very very seldom got new recurring voices. The only time I can remember when I had an explosion of complex voiced was when I had my biggest psychotic break, and that case was correlated to feelings of switching, and generally very system like stuff, however, I'm,,,,, suspicious of that event as the nature of the psychotic break was partially tied to someone telling me they thought I was a system and that I had forgotten my trauma. It was not caused by that person, mind you, but while in a psychotic break I am very easy to influence and I theorize the very system like traits, which stopped after the psychotic break receded, were just how my psychosis reacted.
So tl;Dr :
- the voices are internal and not able to be mistaken for speech. They are like the voice you hear when you think words in your brain intentionally, I just don't control them and they have their own "tone".
- I have alter like voices that stick with me during a long period of time and keep a coherent personality, but also intrusive thought-like voices that stick just for the duration of the discussion and have no real personality.
- alter like voices can be aggressive but can be reasoned, intrusive voices are just. Kinda repeating whatever they're trying to say and it tends to be very unpleasant.
- I do not seem to switch naturally. I also experience derealization (outside world feels weird) but I do not dissociate or feel like I skip time. I do not have significant trauma. These are all specific to me, I do not really know if someone else with whatever I have could possibly switch.
- both type of voices went away upon taking antipsychotics. I have taken quetiapine (Seroquel I think in English?) and Loxapac, both seem to block them.
Hope that's enough to help.
7 notes
·
View notes
Text
DYSEMPATHY
“People understand me so poorly that they don’t even understand my complaint“ about them not understanding me.” —Søren Kierkegaard
Yes, I know that dysempathy is not a word, but antipathy, apathy, acedia, or angst don’t define the feeling; and social anxiety, dysthymic, or antisocial personality disorders don’t label it. What I’m trying to name is the lack of the ability to connect to others…

View On WordPress
#acedia#alcohol#angst#art#career#connections#dysthymia#empathy#fantasy#friendship#introspection#love#nostalgia#pair bonding#romance#social anxiety#success#usefulness
3 notes
·
View notes
Text
An Intro to Atypical Depression in Under 11 Minutes
Major depression, often known as dysthymic disorder, has a subtype known as atypical depression. People who suffer from atypical depression tend to have increased hunger or excessive weight gain, drowsiness or excessive sleeping, exhaustion or weakness, and mood swings that are strongly influenced by environmental conditions.
What is Atypical Depression: Detailed explanation
The symptoms of this depression are unlike those of melancholic depression, which are primarily characterized by sadness regardless of hope or good fortune. By contrast, atypical depression occurs when circumstances change, resulting in an improvement in mood. In other words, if something good occurs, a person's mood can get better. Although this mood improvement lasts for a limited period of time, it is temporary.
A mental illness which is known as major depressive disorder (MDD) can have an impact on a person's thoughts, feelings, and actions. They don’t find their life worth living and start staying in isolation. MDD patients frequently lose interest in the things they normally love doing and struggle to complete routine duties.
When a person suffers from atypical depression, the disorder does not show the same symptoms as "typical" depression. There is one important exception to the symptoms of atypical depression that differs from those of major depressive disorder (MDD) which is called “mood reactivity.”
Depression is often identified when a person is a teenager. Studies have shown that this mental ailment is basically referred to as MDD along with atypical features.
Atypical depression: how serious is it?
People suffering from any sort of mood disorder usually feel stuck and traumatized. Their mental health gets worse with time. one never knows when this can hit him/her. In our daily life, we usually get affected by numerous events occurring that affect us negatively and no matter how hard we try to escape those conditions, eventually we get trapped by them.
Atypical depression, on the other hand, is a bit different type of depression where there are chances of a person feeling better in a few circumstances. When something positive happens to him/her, then, at least for a small period of time, they feel better. There are possibilities of one getting improved mental conditions. The fact is people around them need to understand them and support them. Consequently, which is not in our hands.
An explanation of atypical depression in adolescence
#atypical depression#melancholic depression#Major depressive disorder#MDD#depressive episode#Depression#mood disorders#mental illness
7 notes
·
View notes
Text
Depressive / Melancholic Personality Disorder (De/MePD)
Note: You cannot be diagnosed with this disorder, as it's not in any diagnostic manual; you would be diagnosed with Other Specified Personality Disorder instead.
Criteria from the DSM-IV-TR (2000):
A pervasive pattern of depressive cognitions and behaviors beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following:
usual mood is dominated by dejection, gloominess, cheerlessness, joylessness, unhappiness
self-concept centers around beliefs of inadequacy, worthlessness, and low self-esteem
is critical, blaming, and derogatory toward self
is brooding and given to worry
is negativistic, critical, and judgmental toward others
is pessimistic
is prone to feeling guilty or remorseful
Millon's subtypes:

(Millon, ed.).
About De/MePD
De/MePD is similar to avoidant, schizoid, masochistic / self-defeating, negativistic / passive-aggressive and borderline PDs. It's part of what Millon & Bloom term the "Reserved Personality Patterns", along with AvPD & SzPD.
Differential diagnoses include anxiety disorders, mood disorders, and somatic disorders.
The most common PD comorbidities with De/MePD are AvPD (19.53%), AsPD (14.06%), & Negativistic / Passive-Aggressive PD (13.02%). The least common was HPD (1.82%). Less than 6 percent (5.34%) had only ("pure") De/MePD [much higher than people with pure Ne/PAPD or SaPD] (Millon & Bloom).
Millon defines it on a spectrum from pessimistic -> depressive (melancholic) (Millon Personality Group); or alternatively from dejected [personality type] -> forlorn [style] -> depressive [disorder] (Millon).
"The depressive and masochistic are so similar that some authors view them as a single constellation" (Millon, ed.).
In the DSM-IV-TR it was described as being “characterized by a pervasive pattern of depressive cognitions and behaviors, low self-esteem, brooding, and pessimism." (Coolidge & Segal).
"Always in a dejected and gloomy mood, they see themselves as inadequate and worthless. They submerge themselves in criticism for even minor shortcomings and tend to blame themselves when things go wrong. A pervasive pessimism leads them to anticipate the worst - to expect that life will always go wrong and never improve. Their days are spent brooding and worrying, ignoring the good and dwelling on the bad. Saturated with guilt, they wish that life could be different, but instead of taking the initiative, they berate themselves for missed opportunities and feel powerless to change their destiny. Such individuals may indeed be depressed, but their depression emerges from a way of thinking, feeling, and perceiving - a depressive personality" (Millon, ed.).
De/MePD only ever appeared in the appendix of the DSM-IV & IV-TR, and it was dropped because it was "controversial whether the distinction between depressive personality disorder and Dysthymic [Persistent] Disorder [was] useful" (DSM-IV-TR).
However, "many dysthymics did not meet criteria for depressive personality. [...] In fact, the proportion of those with depressive personality disorder who had never met criteria for dysthymia was high", indicating that De/MePD is likely a separate disorder from persistent & major depressive disorders (Millon, ed.).
References
Coolidge, Frederick L., & Segal, Daniel L., ‘Evolution of Personality Disorder Diagnoses in the Diagnostic and Statistical Manual of Mental Disorders’, Clinical Psychology Review, 1998, vol. 18, no. 5, pp. 585-599.
Millon, Theodore, & Bloom, Caryl, The Millon Inventories, 2008.
Millon, Theodore, Disorders of Personality, 2011.
Millon, Theodore, ed., Personality Disorders in Modern Life, 2004.
'Pessimistic / Melancholic Personality', Millon Personality Group, 2015, https://www.millonpersonality.com/theory/diagnostic-taxonomy/melancholic.htm.
#melancholic personality disorder#depressive personality disorder#other specified personality disorder#ospd#dsm iv#dsm iv tr#dsm-iv#dsm-iv-tr#described#described in alt text#dogpost#long post#personality disorders
2 notes
·
View notes
Text
The pain deep inside
There is a pain
I hold deep inside
Feeling broken
And aching in misery
There is a pain
I hold deep inside
Afraid to share
For who would care?
There is a pain
I hold inside
No matter what I do
I always screw up
There is a pain
I hold inside
No matter how hard I work
It always falls apart
There is a pain
I hold inside
No matter how hard I try
There is no place for me
There is a pain
I hold deep inside
Am I good enough?
Am I cursed?
There is a pain
Deep inside
I don't want to live
I don't want to die
There is a pain
Deep inside
Feeling stuck in limbo
Trying to just survive.
There is a pain
Deep inside
The deeper I reach
The more fear I feel
There is a pain
Deep inside
Afraid to feel
Afraid to be weak
There is a pain
Deep inside
Afraid to cry
Afraid to fly
There is a pain
Deep inside
Afraid to fail
Afraid of myself
Note- I wrote this during a depression episode. I am going to talk to my dr about it because I think I have premenstrual dysthymic disorder. Its where its like severe PMS. Every month I get severe depression and irritability. I had just learned this term awhile ago #womanshealth #mentalhealth
4 notes
·
View notes
Text
Major Depressive Disorder vs. Persistent Depressive Disorder: Understanding the Difference

When we talk about depression, there are generally two different categories that people in the mental health field tend to focus on: major depressive disorder and persistent depressive disorder. Understanding the differences can help the individual identify the type of disorder that they may be suffering from. It can also help when seeking a diagnosis or seeking treatment. Major depressive disorder, also known as unipolar depression or clinical depression, is a mood disorder that is characterized by the same signs as other forms of depression. People with this disorder experience extreme sadness, guilt, reduced concentration, lethargy, and other related symptoms for at least two weeks. These symptoms are typically accompanied by a lack of interest in activities that were once enjoyable, and they may have difficulty sleeping or sleeping significantly more than usual. Persistent depressive disorder, formerly known as dysthymic disorder, is another mental illness. It is characterized by a depressed mood that can last for over two years. Persistent depressive disorder usually involves feelings of hopelessness and worthlessness, changes in appetite, and a lack of motivation and interest in life. Unlike major depressive disorder, these symptoms may not be as severe or frequent, but they typically last for much longer. While it is important to understand the differences between major depressive disorder and persistent depressive disorder, it is also important to recognize that both can be effectively treated with medication, therapy, lifestyle changes, and other forms of treatment. Here are the key differences between the two:
Major Depressive Disorder usually involves more intense and dramatic symptoms, such as an inability to enjoy activities that once brought joy, extreme feelings of guilt, and a lack of desire to engage with other people. Symptoms may also linger for longer than two weeks.
Persistent Depressive Disorder involves more subtle symptoms than major depressive disorder, such as feeling slightly down or having a negative outlook. These symptoms typically remain consistently for over two years.
Both mental illnesses can be treated through medication, therapy, lifestyle changes, and drug rehabilitation programs at addiction treatment centers.
It is important to remember that no one should have to face depression on their own and that seeking treatment is the best way to address the symptoms and underlying issues that may be causing them. Speaking to a mental health professional is a good first step for anyone who feels that they may be living with either major depressive disorder or persistent depressive disorder.
0 notes
Text
Introduction
Hi, my name is Mouse. Nice to meet you :)
[Likes and follows from @pansyp-nk]
I'm a 23 year old autistic person. They/he.
I was diagnosed in my teens, but I'm still figuring out what autism means to me & learning to accept my disabilities. Poster child of the "high masking gifted kid to autistic burnout" pipeline.
Some more about me:
Dutch (voornaamwoorden: die/hen of hij)
Autism, suspected adhd/adhd traits. Dysthymic disorder. SPD. Long history with ED's. To summarise, a nightmare for insurance companies.
In college (somehow?)
Verbal but it takes effort to speak clearly
Always stimming!
Animals are very important to me. Especially cats!
Special interests: minecraft, cat behaviour, archaeology, (special) education & pedagogy
May talk about topics like drug use, relationships and food. Will tag triggers!
0 notes
Text
Dysthymic Disorder/Persistent Depressive Disorder - DSM-5 Criteria Calculator
The DSM-5 Criteria for Major Depressive Disorder diagnoses major depressive disorder (MDD).
0 notes
Photo

Found out I might have dysthymic disorder, a kind of depression #poem #poetry #poet #poetsofinstagram #text #writing #writer #write #author #words #dikt #dikter https://www.instagram.com/p/CmKTYloK5rN/?igshid=NGJjMDIxMWI=
1 note
·
View note
Last Seen Blogs

namrata00
Untitled

mrprincee0
_mr.princee


within-infant-rind
l'appel du vide

tarmiches
Elizabeth's Closet