#diagnostic triad
Note
hey, i don't want to put you out or anything, i was just wondering if like off the top of your head if you knew any disability studies articles/books/whatever that center (or even just feature) tic/involuntary movement disorders?
so the answer to this was pretty much no but i spent a bit of time poking around and turned up this 2023 undergraduate honors thesis (link) by a student with tourette’s which seems like a solid starting point for going down the citation rabbit hole!
that piece is “The Embodied Performance of Tics and Tourette Syndrome in the Academic Environment” by Benjamin Allen; i’m only ~1/4th through rn but they argue for a continuum of ticcing + criticize the diagnostic system so i’m comfortable reccing it on that front! the (non-medical) tic-related works cited there are:
Buckser, Andrew. “Before Your Very Eyes: Illness, Agency, and the Management of Tourette Syndrome.” Medical Anthropology Quarterly, vol. 22, no. 2, 2008, pp. 167-192.
Buckser, Andrew. “The Empty Gesture: Tourette Syndrome and the Semantic Dimension of Illness.” Ethnology, vol. 45, no. 4, 2006, pp. 255- 24. https://www.jstor.org/stable/20456601.
Curtis-Wendlandt, Lisa. “Time and the Tic Disorder Triad.” Philosophy, Psychiatry, & Psychology, vol 27, no. 2, 2020, pp. 183-199.
Curtis-Wendlandt, Lisa, and Jack Reynolds. “Why Tourette syndrome research needs philosophical phenomenology.” Phenomenology and the Cognitive Sciences, vol. 20, no. 4, 2021, pp. 573-600.
Miller, James. “The Voice in Tourette Syndrome.” New Literary History, vol. 32 no. 3, 2001, pp. 519-536. Project MUSE, doi:10.1353/nlh.2001.0039.
Trubody, Ben. “Ticced off: An Interpretative Phenomenological Analysis of The Experience of Tourette’s Syndrome.” Journal of the Society for Existential Analysis, vol. 25, no. 2, 2014.
i also searched a handful of disability studies journals for a variety of keywords (movement disorder, tic, tourette’s, involuntary movement, chorea, huntington’s) but didn’t turn up much unfortunately, so all but the first of this next list include someone with tics and/or involuntary movements rather than being about moving involuntarily.
haven’t read these so i can’t speak to the politics / quality (although i’ll make a post if i’m able to read more) but here’s what seemed potentially relevant! also if anything is paywalled please don’t give T&F your money lol, try SciHub or if you can’t find something i can ask around for somebody with institutional access!
Cultural Differences in Reactions to Tics and Tic Severity (2021)
Using virtual reality to implement disability studies’ advocacy principles: uncovering the perspectives of people with disability (2023)
I had every right to be there: discriminatory acts towards young people with disabilities on public transport (2020)
From comedy targets to comedy-makers: disability and comedy in live performance (2015)
From the Case Files: Reconstructing a history of involuntary sterilisation (2010)
i also want to mention “Movements of the Uncontrollable Body Part Two” by Bronwyn Valentine (2019), a creative writing piece about her experiences of embodiment + ableism with spina bifida that i first read pretty soon after it was published & went looking for after developing my movement disorder a year ago because it was so impactful. @fndportal also has some incredibly vital work.
also if you haven’t already read Rosemarie Garland-Thomson’s Staring: Why We Look, it’s not specifically about involuntary movements but definitely a core text for theorizing any visibilized disability.
i hope some of that is helpful!! if anybody checks any of these out i’d love to hear your thoughts/critiques! all the best to you & i hope these offer some resonance with + understanding of your experiences 💓💓
#tics#ticcing#involuntary movements#movement disorder#disability studies#asks#reading lists#movements of the uncontrollable body
31 notes
·
View notes
Text
My Azula Diagnosis Analysis Part 5: Machiavellianism
As the master post I wrote was too long, I’ve divided it into parts. Find them all here.
Sick of bad armchair diagnosis for Azula? Me too! So in this thread let’s discuss Azula’s most commonly “diagnosed” illnesses and disorders, and find out what she actually meets the criteria for, if any.
Is Azula machiavellian?
Machiavellian Claims
—Azula displays “The Dark Triad” of personality disorders; psychopathy, narcissism, and Machiavellianism. If she displays the other two, she must also have the third.
—Azula is highly manipulative
—Azula shows no empathy and only cares about her own personal gain/success
—Azula sees others only as pawns in her chess game
—Azula favors fear over love
So Is Azula Machiavellian?
Machiavellianism is not an actual personality disorder, but rather a personality trait. This may seem like a small distinction but the difference is quite significant, especially when it comes to diagnosis. As a result, the diagnostic criteria for this personality trait isn’t as firmly agreed upon, and multiple experts have suggested different models for identifying it.
Let’s look at the two most prominent criteria:
#1. Core Features for Identifying Manipulators
—A relative lack of affect in interpersonal relationships: Characterized by a lack of empathy for the victims they manipulate. This doesn’t quite fit Azula, as while she is highly manipulative towards her loved ones, she is also shown to empathize with and understand their traumas, and to be deeply hurt when she is abandoned. She is far less empathetic when manipulating her enemies, but this isn’t unusual in war.
—A lack of concern for conventional morality: This is interesting because while it’s easy to say Azula’s behavior isn’t always moral, this criteria specified “conventional morality”. As-in what’s considered moral relative to her environment. Azula does not display a lack of concern for her nation’s morality, and is in fact usually acting in their interests. The horribly violent, imperialistic culture of the Fire Nation is normal to her.
—A lack of gross psychopathology: In other words, a lack of mental illness that could otherwise explain their behaviors. Once again, Azula doesn’t fit the criteria, as her psychotic breakdown at the end of The Show demonstrates there’s clearly something else going on with her mental health.
—Low ideological commitment: Yeah, no. Azula is loyal to Ozai and the Fire Nation to a fault.
Azula doesn’t fit any of the core features. So let’s try a different model and see how she fares there.
#2. The Five Factor Model (aka Three Underlying Characteristics)
—Antagonism: (Manipulativeness, cynicism, selfishness, callousness, and arrogance.) Azula fits them all except arguably selfishness as most of what she does is in service of her father.
—Planfulness: (Deliberation and orderliness.) Azula fits both very well.
—Agency: (Achievement-striving, assertiveness, self-confidence, emotional invulnerability, activity and competence.) This one is a mixed bag. Azula absolutely strives for achievements, is assertive, and self confident in her abilities though not in her own self worth. She is however not emotionally invulnerable as made clear by her break down. She doesn’t seem to be emotionally active either, choosing to repress and hide her trauma regarding her mother and cowtow to her father despite his abuse. Whether she is emotionally competent or not is complicated too, in that she’s excellent at reading others, but terrible at connecting with them on an emotional level.
Conclusion: Azula has some Machiavellian traits at best, but isn’t a full blown Machiavellian. As machs can be classified as either “high machs” and “low machs”, an argument can be made that Azula is a “low mach”.
There’s not a lot to say other than Machiavellianism requires a certain level of agency that Azula just doesn’t have in The Show. She is under Ozai’s influence, control, and orders for almost all of it, and the two seem to have an unhealthy enmeshment as is common for narcissistic parents and their Golden Child victim.
In the comics, Azula is disregulated and struggling to find herself, ping-ponging between ally and enemy, desperate to find her destiny and place in the world.
Not exactly the well calculated and controlled nature of a true Machiavellian.
Nonetheless, she does display some concerning Machiavellian traits, likely a result of being so enmeshed with her father and forced to reflect his behaviors and tendencies to survive. But not all of her behaviors can be fully attributed to mimicking Ozai, as while Ozai is shown to be highly manipulative—in the comics especially—he also seems to be less of a long-term planner than Azula, sometimes making hotheaded decisions to his disadvantage out of ego. Azula is more calculating and tactical.
Just as with Sociopathy/ASPD many of the claims made to support Azula as a Machiavellian personality are either exaggerated or inaccurate. “The Dark Triad” concept has been foisted on her so heavily that many accept it without question. Even Wikipedia lists her as having it.
But the evidence for this claim is scant, as Azula doesn’t meet the criteria for either ASPD or NPD, nor would the presence of the other two automatically mean she must have the third.
The claim that Azula prefers fear over love is also strange, as during her argument with her hallucination of Ursa, it’s revealed that Azula utilizes fear because she believes it’s “the only way”, not because it’s her preference. “What choice do I have?” It’s clear in-context that Azula yearns for real love, the kind of love Zuko got from Ursa growing up, but fears she is inherently monstrous and unloveable so fear is all she has.
That isn’t a preference. That’s desperation.
16 notes
·
View notes
Note
(P-word warning)
ASPD culture is being so good at manipulating ppl's perceptions of you that you even managed to convince yourself you didn't have ASPD (or NPD tbh) for a while, even after taking that "dark triad" test as a joke and scoring extremely high in both narcissism and psychopathy and unusually high in machiavellianism.
(Disclaimer: that test is NOT a diagnostic tool nor was I using it as one, I had just convinced myself ASPD wasn't even a possibilty for me)
aspd-culture is
#tw psychopath#valid#mood#aspd-culture-is#aspd culture is#aspd culture#actually antisocial#actually aspd#antisocial personality disorder#aspd#aspd awareness#aspd traits#anons welcome
7 notes
·
View notes
Text
"Narcissistic abuse" vs NPD
Hey guys, i feel like I need to talk about something, if only because i was one of those ppl who ended up watching a lot of videos about "narcissistic abuse" which demonized tf out of ppl with NPD so now i feel a moral obligation to do something, whatever that may be. So I guess this is one of my attempts to do something.
Because im someone who ended up watching a lot of those videos, it really forged my perceptions of people with NPD, but i think theres an important distinction here to be made. I do personally feel like narcissistic abuse exists, but i dont think it exists *only* within the realm of people with npd as a lot of these videos and articles suggest. I think just about anyone can engage in narcissistic abuse because the point is the abuse is incredibly selfish and self centered on part of the abuser. I dont think it has to be connected with people with NPD and the only connection is made with the similar names, so maybe we need to come up with a new term for it, because ive personally found a lot of value out of those videos, it helped explain to me what was going on, the way people abused me, the way their mind worked, what they were likely to do, etc. And has pretty much been on the nose. I dont think multiple videos like this would exist if there wasnt a common experience. I just dont think its something people with npd exclusively do like a lot of these videos suggest. Im like 90% sure one of my bullies abused me this way, would do anything to maintain their social standing and keep me on the bottom, but i do not believe that person has npd and it wouldnt be fair for me to diagnose that person anyways because i barely know anything about that person personally.
Part of the reason these videos kinda revealed to me its not just an npd thing is the fact that they kept having to come up with new, scarier words for ppl with npd. Like "the dark triad" or whatever because the realization that their trauma is the reason they act the way they do makes the victim upset and not want to have to sympathize, which is understandable, but its not healthy and it means they have to make it sound like its something more extreme to have a justification for essentially wanting that person to be kicked off the planet, which i can understand why an abuse victim might feel that way, i just dont think its helpful to shunt all the responsibility on to ppl with npd and obviously that abuse victim needs to be more practical, empathetic and realistic because you cant control other people and you're likely to not actually do anything to your abuser to get revenge, so sitting here seething in your contempt does nothing but hurt you long term while your abuser has essentially forgotten you exist. But i digress.
The biggest issue with these videos is the name of the abuse and the association with ppl with npd, because theres many reasons why people would want to keep their social position outside of an extremely insecure sense of self or whatever tf. The other issue with these videos is the huge demonization and misunderstanding about people with npd. The idea that theyre all abusive, that they cant change, that they hold every Bad diagnostic criteria and it makes them *evil* or whatever tf. The way people talk about ppl with npd in those videos is pretty horrendous actually. It gets to a point where you wonder if the person posting the video wants to essentially genocide ppl with npd, which i think is kinda fuckin crazy ngl, i dont think thats a solution nor do i think all ppl with npd are such a huge problem that we need to get rid of them or exile them from society or whatever tf. Ppl with npd more than anything need therapy of some sort, and these videos 100% can talk about this form of abuse without throwing ppl with npd under the bus every 5 seconds.
I know people dismiss this as just "any kind of abuse" but i really dont think it is, its a really specific, insidious type of abuse where someone will do anything to maintain their position, they will toss away all their morals bc maintaining that position is the most important thing to them. They are people who are very driven by their ego, and anyone can be driven by their ego, so no, its not just an npd thing. Theres other forms of abuse that arent driven by a need to maintain their social position, so also no, its not all the same and i dont think it should all be labeled as general abuse, because the trauma this can cause is notable and having a space to talk with people who've had similar experiences is really important and helpful. We just gotta stop demonizing ppl with npd since its very much not their sole issue, nor would i say its a guarantee ppl with npd will treat you that way, and its pretty toxic to assume that, especially since ppl without npd routinely engage in this form of abuse. I dont believe theres truly any justification for ostracizing and wanting to essentially kill off an entire group of people and ppl should stop trying to find excuses to do so.
Anyways, thing i wanted to say and have been thinking about for a while has been said, you may proceed with whatever judgements you seemingly endlessly have about me.
#narcissistic abuse#npd#also uh... i think we gotta be not so judgemental about ppl who have consumed that content bc theyre going off of what they were told.#those videos make a point of you apparently not needing the nuanced understanding of your abuser so ppl naturally dont look up the sad or#sympathetic parts of ppl with npd.#and bc those videos see narcissistic abuse and npd as essentially two sides of the same coin theres just a lot of confusion for the ppl#consuming those videos. the onus is on the ppl vreating that content to actually educate themselves and stop demonizing and generalizing an#entire population of people.#anyways yeh#my phone kept trying to write nod like every time i wrote npd. omg it just did it too. im so upset i hate my phone shsjkssk
1 note
·
View note
Photo
Algorithm 1: Nmet: normetanephrine; Met: metanephrine; MRI: magnetic resonance imaging; CT: computed tomography; 68-Ga DOTATATE PET: gallium 68 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid-octreotate; FDG: fluorodeoxyglucose; PET: positron emission tomography.
Table 1: Medications that may increase measured levels of catecholamines and metanephrines: tricyclic antidepressants, levodopa, drugs containing adrenergic receptor agonists (e.g., decongestants), buspirone and most psychoactive agents, amphetamines, prochlorperazine, reserpine, withdrawal from clonidine and other drugs, ethanol.
The diagnosis of pheochromocytoma is made based upon biochemical confirmation of catecholamine hypersecretion, followed by identifying the tumor with imaging studies. Many patients are tested for possible sporadic pheochromocytoma, but few will ultimately be diagnosed with the disorder (approximately 1 in 300).
Biochemical evaluation – We suggest initial biochemical testing based upon the index of suspicion that the patient has a pheochromocytoma. If there is a low index of suspicion, we suggest 24-hour urinary fractionated catecholamines and metanephrines; if there is a high index of suspicion, we suggest plasma fractionated metanephrines (algorithm 1). Medications that can interfere with results are reviewed above (table 1). Indications for testing — Pheochromocytoma should be suspected in patients who have one or more of the following:
●The classic triad of headache, sweating, and tachycardia, whether or not they have hypertension.
●Hyperadrenergic spells (e.g., self-limited episodes of nonexertional palpitations, diaphoresis, headache, tremor, or pallor). However, most patients with spells do not have pheochromocytoma.
●Onset of hypertension at a young age (e.g., less than 20 years), resistant hypertension, or hypertension with new-onset or atypical diabetes mellitus (e.g., new onset of apparent type 2 diabetes in a slender person).
●A familial syndrome that predisposes to catecholamine-secreting tumors (e.g., multiple endocrine neoplasia type 2 [MEN2], neurofibromatosis type 1 [NF1], or von Hippel-Lindau [VHL]).
●A family history of pheochromocytoma.
●Lipid-poor (unenhanced computed tomography [CT] attenuation >10 HU) adrenal incidentaloma with or without hypertension.
●Pressor response during anesthesia, surgery, or angiography.
●Idiopathic dilated cardiomyopathy.
●A history of gastric stromal tumor or pulmonary chondromas (Carney triad).
Discontinue interfering medications — Although it is preferred that patients not receive any medication during the diagnostic evaluation, treatment with all antihypertensive medications may be continued. Tricyclic antidepressants interfere most frequently with the interpretation of plasma fractionated metanephrines and 24-hour urinary catecholamines and metabolites. To effectively screen for catecholamine-secreting tumors, treatment with tricyclic antidepressants (including the muscle relaxant cyclobenzaprine) and other psychoactive agents (but not selective serotonin reuptake inhibitors [SSRIs]) listed in the table (table 1) should be tapered and discontinued at least two weeks before any hormonal assessments.
There are certainly clinical situations for which it is contraindicated to discontinue certain medications (e.g., antipsychotics), and if biochemical testing is positive, then computed imaging (e.g., CT scan of the abdomen and pelvis) would be needed to exclude a catecholamine-secreting tumor. Furthermore, catecholamine secretion may be appropriately increased in situations of physical stress or illness (e.g., any significant illness requiring hospitalization, stroke, myocardial infarction, congestive heart failure, obstructive sleep apnea). Therefore, the clinical circumstances under which catecholamines and metanephrines are measured must be assessed in each case.
Levodopa is the most common and only pharmacotherapeutic agent that causes markedly abnormal levels of dopamine.
For patients with biochemical confirmation of the diagnosis, the next step is radiologic evaluation to locate the tumor.
•Imaging – Biochemical confirmation of the diagnosis should be followed by radiologic evaluation to locate the tumor [57,59], not the other way around (algorithm 1). In sporadic pheochromocytoma, computed tomography (CT) or magnetic resonance imaging (MRI) of the abdomen and pelvis is usually performed first. Either test detects almost all sporadic tumors because most are 3 cm or larger in diameter. (See 'CT and MRI' above.)
If CT or MRI is negative in the presence of clinical and biochemical evidence of pheochromocytoma, one ought first to reconsider the diagnosis. If it is still considered likely, then iobenguane I-123 (also known as metaiodobenzylguanidine [MIBG]) scintigraphy may be done; this scan can detect tumors not detected by CT or MRI. (See 'Iobenguane I-123' above.)
Other imaging studies are more sensitive than iobenguane I-123 and CT/MRI for detection of metastatic disease. (See 'FDG-PET' above and '68-Ga DOTATATE PET' above.)
•Genetic testing – Genetic testing should be considered in all patients with pheochromocytoma or paraganglioma. (See 'Genetic testing' above.) (table 3)
●Pheochromocytoma in pregnancy – Pheochromocytoma is a rare cause of hypertension during pregnancy, with clinical features similar to those in the general population. The approach to diagnosis is the same as for nonpregnant women. Maternal and fetal mortality rates are high, particularly in those who are not diagnosed until delivery. Optimal medical therapy for pheochromocytoma in pregnancy is not clearly defined. (See 'Pheochromocytoma in pregnancy' above.)
In sporadic pheochromocytoma, both CT and MRI are quite sensitive (98 to 100 percent) but are only approximately 70 percent specific because of the higher prevalence of adrenal "incidentalomas." The choice between CT and MRI depends upon the cost and certain other factors described below.
●With CT, there is some exposure to radiation but no risk of exacerbation of hypertension if current radiographic contrast agents are given. CT with low-osmolar contrast is safe for patients with pheochromocytoma even without alpha- or beta-adrenergic blocker pretreatment, as illustrated in a report of 22 such patients [74]. After intravenous (IV) low-osmolar contrast administration for CT scan, there was a significant increase in diastolic blood pressure but no increase in plasma catecholamine levels or episodes of hypertensive crises.
●With MRI, there is neither radiation nor dye. This more expensive test can distinguish pheochromocytoma from other adrenal masses; on T2-weighted images, pheochromocytomas appear hyperintense and other adrenal tumors isointense, as compared with the liver. However, MRI lacks the superior spatial resolution of CT.
●Familial pheochromocytoma – In patients with the multiple endocrine neoplasia type 2 (MEN2) syndrome, computing imaging may miss approximately one-quarter of the tumors. In a selected group of patients with a 40 percent incidence of pheochromocytoma, the respective positive and negative predictive values of CT were 69 and 98 percent.
●Imaging phenotype of pheochromocytoma/paragangliomas:
-Increased attenuation on nonenhanced CT (most are greater than 20 Hounsfield units [HU])
-Increased mass vascularity
-Delay in contrast medium washout (10 minutes after administration of contrast, an absolute contrast medium washout of less than 50 percent)
-High signal intensity on T2-weighted MRI
-Cystic and hemorrhagic changes
-Variable size and may be bilateral
Additional imaging Iobenguane I-123
●If abdominal and pelvic CT or MRI is negative in the presence of clinical and biochemical evidence of pheochromocytoma, one ought first to reconsider the diagnosis. If it is still considered likely, then iobenguane I-123 (diagnostic) (also known as metaiodobenzylguanidine [MIBG]) scintigraphy may be done. Iobenguane I-123 (diagnostic) is a compound resembling norepinephrine that is taken up by adrenergic tissue. This scan can detect tumors not detected by CT or MRI or multiple tumors when CT or MRI is positive.
●Iobenguane I-123 scintigraphy is superfluous in patients with sporadic solitary adrenal pheochromocytoma identified on CT/MRI.
●Iobenguane I-123 scintigraphy is indicated in patients with large (eg, greater than 10 cm) adrenal pheochromocytomas (increased risk of metastatic disease) or paraganglioma (increased risk of multiple tumors and malignancy).
●Surgery is never indicated based on iobenguane I-123 findings alone; MIBG findings should always be corroborated by findings on computed imaging. Normal adrenal glands take up iobenguane I-123, and the uptake may be asymmetric.
2 notes
·
View notes
Text
[14-1-2024]
Between the yellow paint and blood- all you can see is the blood. Your mistake was costly, and can't be repeated. Another day of living in Cinci, right? Right. Doesn't make it any better. //RRH
Glass hits you. You're caught in a crossfire, and all hell is breaking loose around you. Nearly deaf, simply confused. How quick can you move? You feel heat pumping from your chest. //RRH
Your whole life is a calculated risk. Good days feel like that. Just a deal, but everything if you pull it off. Another day, another week, another month. Just keep working. //RRH
Buried treasure? No, you want to think that. But, it's just another dead drop. Some cash, a few thums, and a spike. SensPerience. Could be game changing but it's doubtful. //RRH
Your eyes lose focus, and you force yourself to blink. Keep putting one foot in front of another, just figuring out where you're going and if you have a reason to even go there. //RRH
Your heart is beating, and somehow that's all that matters right now. They're fast, but you're more limber. You turn down an alley, and then another, and keep going until they're gone. //RRH
Something's wrong. Your ports are still itchy. The diagnostic is red, and the spike ports are... Is this the shakes, or the treatment last month, or... You need help, and soon. //RRH
You keep plodding along. Just one foot in front of the other towards the city, through its gates. Something bad will happen, but something worse will happen if you keep doing nothing. //RRH
He's ragged. Ragged at best. You listen, and glide your pen over the scrap. All he has are names and numbers. And, they all need to know. Not your job, but someone has to do it. //RRH
Does the name mean anything to you? No. Whoever they were is gone. You try to focus, but they're not in your programming now. You've lost something, but, does that matter? //RRH
Self-styled 'nanite artist' Genetrix Io's latest work is a dismal affair. An implant 'seeding' flowers in the human body? Blossom-matrixed keratin for petaled nails; pistil-patterned tonguebuds for pollened saliva? Trite, grotesque, and kitsch-ridden thriftshop fare. //TruthWave
There's new grub down at Gamble. Steamed streetfood tightly scribbled all over with Chinese calligraphy. Triad thing? Tried to get the lowdown from an Asian head, but it's all hush-hush, some secret lingo or dialect she didn't know. Looks killer though, real eyecandy. //TruthWave
Found a derelict SensPerience parlour once. A Chinese sign that looked like a melting sundae outside, men lying silent like mannequins inside. When I came back, the men were dead. Only one remained. He came to the window and smiled. Golden eyes, mouth red as blood. //TruthWave
Corpo exec went poof at the airport and there's still no buzz on the news. Tale got nixed the moment they sniffed something shady in the footage. All those tunnels down there—it's the goddamn catacombs. One wrong step and you're gone. Swallowed. Total black hole zone. //TruthWave
Individuals experiencing retinal implant-induced hallucinations are advised to refrain from interacting with visual anomalies to prevent the misdirection of retinal nanites onto unintended neural pathways. Cases of people falling into unrousable dreams are escalating. //TruthWave
Our bash got stormed by the pigs and yeah, our bad for not fisting their asses full of dough beforehand, but they nabbed some real weird shit. Drugs and guns chillin', but the houseplants? Every last pot gone. The hell? Anyway, we're hittin' Tower back to save Fernie. //TruthWave
Met a man claiming to live not on food, not on water, but air; a proprietary blend of gases some exclusive clinic deep in the Projects injects into his lungs. Made a bet with a sniper; she's now down 15k and up a brain-splattered, half-chewed burger. Ho hum. //TruthWave
Rip Van Winkle spike ain't a myth—it completely ruined my Ma. She's just a shell cryin' over some ghost life, now. A lifetime lived in a blink. Irony is you don't came back to a future world like the tale. You come back to a world that you no longer have any use for. //TruthWave
Ready to sing like Xara One? Insiders report that Sens star Genetrix Io is spearheading a partnership between CinnTech and SensPerience for her hotly anticipated new Sens series, said to use a revolutionary next-gen Sens spike designed to leave bio-imprinted souvenirs.//TruthWave
Fears of implant sentience gain awareness as anecdotal accounts of pain controller implants 'Pavlovian-conditioning' individuals become widespread. "It's deliberately choosing when to turn the pain tap on or off," one man says. "Subtle, insidious manipulation." //TruthWave
0 notes
Text
# Keeping the Eyes Healthy: Revealing the Knowledge of **Eye Care Professionals**
With regard to the complex field of ocular health, **eye care specialists** stand out as the watchful custodians of our most valued sense: vision. These committed experts, also known as **Shreveport Eye Specialists**, are sentinels of knowledge, providing a wide array of services to protect and improve our vision. We explore the complex world of **eye care specialists** in this thorough examination, emphasizing the importance of choosing the best **eye doctor in Shreveport** while delving into their groundbreaking work in **non-invasive eye surgery** and the game-changing potential of **Lasik Shreveport**.
## What Makes **Eye Care Specialists** Unique
**Eye care specialists** are a broad group of medical practitioners who each provide their own talents and expertise to the complex fabric of ocular health. They include ophthalmologists, opticians, and optometrists, each of whom specializes in a different area of eye care. Let's analyze their functions, highlighting the importance of what they do to uphold and improve our vision.
**Optometrists**: Guardians of Visual Wellbeing
**Optometrists** are the pioneers of eye care, frequently acting as the first point of contact for those seeking ocular well-being. These specialists, who hold Doctor of Optometry (OD) degrees, have received extensive training in the diagnosis and treatment of a broad range of ocular disorders.
**Optometrists** are essential to the standard eye examination process. They carefully measure visual acuity, check for refractive defects including astigmatism and myopia, and do a comprehensive examination of the health of the eyes. Using a variety of cutting-edge diagnostic instruments, they examine the complex anatomical features of the eye, looking for early signs of diseases such as diabetic retinopathy or glaucoma.
Additionally, **optometrists** are skilled in writing prescriptions for contact lenses and glasses that are specific to each patient's needs. Their in-depth knowledge of ocular optics guarantees that corrective lenses offer the best possible visual comfort in addition to clear vision.

## **Ophthalmologists**: Master Surgeons in Eye Health Surgery
*Ophthalmologists** are medical professionals who specialize in the diagnosis, treatment, and surgical management of illnesses and ailments of the eyes. They represent a higher standard of care in the field of eye care. Their knowledge is essential for protecting and regaining vision.
eye specialist shreveport **Ophthalmologists** are the heroes of **non-invasive eye surgery**, like **Lasik Shreveport**. They carry out complex operations that realign the cornea, fix refractive problems, and free people from the limitations of contact lenses or spectacles. The accuracy of these procedures, which are often called "refractive surgery," exemplifies the science and art of vision correction.
**Ophthalmologists** are excellent at treating problems including cataracts, glaucoma, and macular degeneration in addition to refractive surgery. Their expertise in surgical procedures like as retinal and cataract surgery has changed the lives of innumerable people and opened the door to a better future through improving vision.
**Opticians**: Artists of Visual Accuracy
The final member of the triad of **eye care specialists** is **opticians**, who are craftspeople in the field of eyewear. These knowledgeable experts are the ones that save your prescription, converting the advice from ophthalmologists or optometrists into actual eyeglasses or contact lenses.
The specialization of **opticians** is precision. They meticulously make the lenses, making sure they match the prescription exactly, whether it's for multifocals, bifocals, or single vision. They also practice the fine art of frame fitting, which means they help you choose eyeglass frames that go well with your lifestyle and personal style in addition to enhancing the features of your face.
## Lasik Shreveport's Power: An Overview of Non-Invasive Eye Surgery
As a spectacular example of **non-invasive eye surgery** that has completely changed the field of vision correction, **Lasik Shreveport** is a monument to the success of contemporary ophthalmology. "LASIK" stands for Laser-Assisted In Situ Keratomileusis, and it has a very significant positive effect on improving vision.
The cornea, the outermost layer of the eye, is first prepared by creating a thin, hinged flap. What happens next is a marvel of accuracy as the cornea is softly reshaped by an excimer laser that flashes cold ultraviolet light. As a result, the curvature is optimal and light beams are redirected into the retina with astounding accuracy.
The **Lasik Shreveport** procedure is renowned for its short recovery time and little pain. Within a day or two, the majority of patients report better eyesight, with many expressing instant clarity. People are no longer bound by the limitations of glasses and contact lenses thanks to this ground-breaking technique, which has given them the gift of clear vision.
Selecting the Appropriate **Ophthalmologist in Shreveport**: A Wise Choice
Choosing the best **eye doctor in Shreveport** is the first step on the path to excellent eye health. Here are a few crucial things to remember:
1. **Qualifications**: Verify that the **eye doctor Shreveport** you have selected is licensed and has the necessary qualifications. Professionals with board certification often follow very strict requirements for their education and training.
2. **Experience**: Expertise and experience are frequently interchangeable. Experienced **Shreveport Eye Specialists** often have a thorough grasp of a wide range of eye diseases.
3. **Technology** : Examine the diagnostic tools and technological resources that the clinic has to offer. Modern equipment can improve the precision of your ocular examinations and the standard of treatment you get.
4. **Patient Reviews**: Reading through patient endorsements and reviews may bring you a wealth of information about the standard of treatment that your preferred **Shreveport eye doctor** provides.
5. **Compatibility** : Take into account how well you and your **eye doctor Shreveport** get along. A successful patient-physician relationship is built on trust and open communication.
## The Ocular Wellness Continuum
To sum up, **eye care specialists** are the guardians of our visual health, assisting us in navigating the many nuances of eye health. Their combined knowledge in ophthalmology, optometry, and optics guarantees that our eyes get the careful attention they require.
These experts are prepared to support and improve our vision, whether we need regular eye exams, contact lens or spectacle correction, or the life-changing wonder of **Lasik Shreveport**. These committed specialists protect and enhance the gift of sight in Shreveport, a city known for its culture and energy. We may welcome a future filled with the clarity and beauty of unhindered vision under their leadership.
1 note
·
View note
Text
Applied Kinesiology: What Is It and How Can It Help Me

Applied Kinesiology (AK) is a distinctive and multifaceted therapy that combines various aspects of conventional and alternative medicine. Developed in the 1960s by chiropractor George J. Goodheart, it's an approach that offers a holistic view of a person's health, focusing on the triad of health - structural, chemical, and mental factors.
Understanding the Basics of Applied Kinesiology
At its core, Applied Kinesiology revolves around the concept of muscle testing. An Applied Kinesiologist, a trained practitioner, uses muscle strength testing as a diagnostic tool. The fundamental belief is that each major muscle group is linked to a specific organ or gland, and muscle weakness can signal distant internal problems such as nerve damage, reduced blood supply, chemical imbalances, or other issues.
The Diagnostic Process
An Applied Kinesiologist may apply light pressure to a muscle during a session and assess the response. A force that resists well indicates good health, while a power that fails to withstand the pressure suggests an underlying problem. This diagnostic process allows the practitioner to uncover imbalances in the body's structure, chemistry, or emotional state.
Beyond Muscle Testing
However, Applied Kinesiology isn't limited to just muscle testing. It's a holistic approach that can include elements of:
Nutritional Analysis: Suggesting dietary changes or supplements to address chemical imbalances.
Chiropractic Techniques: To correct structural imbalances.
Acupuncture and Meridian Therapies: For energy balance.
Counseling: To address emotional factors.
How Can Applied Kinesiology Help?
People often turn to an Applied Kinesiologist for various reasons. Some of the potential benefits include:
Identifying Allergies: Discovering sensitivities to foods or environmental factors.
Pain Relief: Especially for musculoskeletal pain like back pain, neck pain, or joint issues.
Stress and Emotional Well-being: Managing stress and emotional issues by better understanding the body's responses.
Improving Overall Health: Gaining insights into the body's needs, whether nutritional, physical, or emotional.
Selecting a Qualified Applied Kinesiologist
When seeking an Applied Kinesiologist, it's essential to choose a properly trained and certified practitioner. Look for someone with a healthcare background, such as a chiropractor, physician, or physical therapist, and who has additional training in Applied Kinesiology.
Conclusion
Applied Kinesiology offers an intriguing blend of traditional and alternative medical practices. It's a holistic approach that looks beyond the symptoms to the underlying causes of health issues. While it may not be suitable for everyone or every condition, it provides an additional avenue for those seeking a comprehensive understanding of their health and well-being. As with any therapy, it's crucial to consult with healthcare professionals to determine the best approach for your individual needs.
0 notes
Text
En 1908, le professeur autrichien Théodore Heller décrit un trouble qu'il présente comme une « démence juvénile » et qui sera dénommé plus tard sous le nom générique de « trouble désintégratif de l'enfance ».
La première formalisation clinique d'un trouble infantile distinct des schizophrénies a été faite en 1943 par Leo Kanner qui définit les « troubles autistiques du contact affectif » à travers onze cas correspondants
Il l'utilisait alors pour distinguer l'un des trois comportements typiques des schizophrénies pour faire face à une réalité oppressante.
Ce premier comportement, nommé « autisme », consistait pour y faire face à l'ignorer ou à l'écarter un deuxième consistait à la reconstruire,
c'est la psychose et un troisième consistait à la fuir par dé-socialisation, ce qu'il associait aussi à la plainte somatique (hypocondrie).
Le besoin de distinguer et d'isoler un trouble propre au jeune enfant
Lorna Wing redécouvre le travail oublié de Hans Asperger qui, comme Leo Kanner la même année, avait isolé des cas cliniques d'un trouble spécifiquement infantile qualifié d'« autistique
Elle publie en 1981 sa propre étude sur ce qu'elle nomme syndrome d'Asperger
elle propose l'idée d'une continuité entre les distinctions faites par Kanner et celles faites par Asperger ce qu'elle met en évidence en définissant trois critères de référence.
troubles de la communication verbale et non verbale
altérations des interactions sociales réciproques
comportement présentant des activités et des centres d'intérêt restreints, stéréotypés et répétitifs.
Cette « triade autistique » reste aujourd’hui une référence pour identifier et définir l'autisme et le trouble envahissant du développement.
Cette catégorie est apparue avec le passage du DSM III au DSM IV mais la tendance en 2011 semble être à la préférence de la notion de spectre autistique et à la simplification de la triade en deux critères :
l'un social, l'autre comportemental.
Cette description clinique a permis le développement, de la recherche en génétique et en neurophysiologie sur les causes et le traitement de l'autisme, puis du spectre autistique.
Dans ce contexte, divers·e·s auteur·e·s, intervenant·e·s et organisations militantes explorent la question des influences réciproques entre expérience vécue de l’autisme et influence du genre :
existe-t-il, et si oui dans quelle mesure et avec quelles conséquences, des liens significatifs entre identité de genre, orientation sexuelle et autisme ?
Quelle est l'expérience vécue par les personnes autistes qui s'identifient membres de la communauté LGBTQ
qu'« il existe une plus grande prévalence des personnes des minorités de genre chez la population autiste qu’au sein de la population neurotypique et, réciproquement, une plus grande prévalence de l’autisme chez les populations trans et non binaires que chez les personnes cisgenres
Ces relations entre autisme, identité de genre et orientation sexuelle sont actuellement des cooccurrences démontrées, et non des relations de causes effet.
Ce constat laisse penser qu'il existe une aggravation des difficultés quotidiennes pour les personnes à la fois autistes et LGBTQ.
Des recommandations émergent pour aider ces personnes souvent doublement stigmatisées via par exemple une plus grande ouverture à la diversité sexuelle,
à la pluralité des genres et à la neurodiversité dans l'éducation à la sexualité,
la prévention des souffrances et agressions sexuelles, la création d'espaces sécuritaires, ect.
En psychiatrie, la notion de trouble du neurodéveloppement (TND), ou trouble neurodéveloppemental,
se substitue en partie aux notions de trouble du développement présente dans le CIM-10 et de trouble envahissant du développement présente dans le DSM-IV.
Elle inclut notamment le TDA/H, les TSA et troubles dys
Un trouble du spectre de l'autisme est un diagnostic de l'autisme dans la 5e édition du Manuel diagnostique et statistique de l'Association américaine de psychiatrie (DSM-5).
Les éditions antérieures du DSM, et la 10e édition de la Classification internationale des maladies de l'Organisation mondiale de la santé (CIM-10),
utilisent la dénomination troubles envahissants du développement (ou TED).
L'expression « trouble du spectre de l'autisme » témoigne d'une façon différente d'envisager l'autisme.
Description
Les affections (symptômes, maladies, lésions traumatiques,
empoisonnements) et les autres motifs de recours aux services de santé sont répertoriés dans la CIM avec une précision qui dépend de leur importance,
c'est-à-dire de leur fréquence et de l'intensité du problème de santé publique qu'ils posent
(par exemple, le chapitre des maladies infectieuses est le plus gros et le plus détaillé parce que ces maladies sont la première cause mondiale de morbidité et de mortalité).
La CIM est une classification statistique Elle est statistique en ce sens que l'entité faisant l'objet d'un codage ne peut être attribuée qu'à une et une seule catégorie de la classification.
La sixième révision devint la Classification statistique internationale des maladies, traumatismes et causes de décès :
elle cessait en effet de ne répertorier que les causes de décès pour s'intéresser de façon plus générale à la morbidité.
La CIM a été conçue pour « permettre l'analyse systématique, l'interprétation et la comparaison des données de mortalité et de morbidité recueillies dans différents pays ou régions à des époques différentes »
CIM-6
La CIM-6, était le premier manuel contenant une classification des troubles mentaux.
CIM-7
C'est la première version, qui s'intitule officiellement « Classification internationale des maladies ».
Une rubrique « Perversions sexuelles » y est intégrée, au sein de la catégorie « Personnalité pathologique » ;
elle comprend entre autres l'homosexualité, la déviation sexuelle, l'exhibitionnisme, le fétichisme, le sadisme et la sexualité pathologique
CIM-8
La huitième révision de cette classification Les manuels diagnostiques sont plus détaillés, mais limités ; les descriptions cliniques sont absentes.
L'homosexualité devient une sous-rubrique à part entière (comprenant la sodomie et le lesbianisme),
toujours rattachée aux « Perversions sexuelles », désormais catégorisées en « Névroses, troubles de la personnalité et autres troubles mentaux non psychotiques
CIM-9
La CIM-9 Elle est finalement remplacée par la CIM-10 qui donne une plus grande expansion des données.
Il est impossible de convertir les données exposées dans la CIM-9 avec les données exposées dans la CIM-10,
CIM-10
Les projets de la CIM-10 Le système de classification permet à l'aide des diagnostics et procédures, une expansion significative
Plusieurs facilités sont disponibles sur le site officiel de l'OMS pour aider à son utilisation, et incluent un manuel, un mode d'emploi et des données à télécharger
Chaque chapitre est divisé en catégories affectées d'un code à trois caractères, par exemple : asthme J45.
La majorité des catégories propose un niveau de détail supplémentaire ou sous-catégorie dont le code est précisé par un quatrième caractère
(séparé des trois premiers par un point), par exemple : asthme allergique J45.0
Cette version est la première à ne plus comporter, dans la liste des maladies mentales, l'homosexualité.
L'introduction précise : « les troubles de la préférence sexuelle sont nettement différenciés des troubles de l'identité sexuelle.
L'homosexualité, en elle-même, n'est plus considérée comme une catégorie »
L'OMS a révisé la CIM en fonction de la CIM-11.
Son développement a eu lieu sur un espace de travail basé sur Internet qui continue d'être utilisé pour les discussions et les propositions de mises à jour de la CIM.
N'importe qui peut soumettre une proposition fondée sur des données Les propositions sont traitées d'une manière ouverte et transparente, avec des examens des preuves scientifiques.
La version officielle est accessible en ligne Une traduction française est disponible.
Il s'agit de la CIM-11 pour les statistiques de mortalité et de morbidité.
La CIM-11 est beaucoup plus facile à utiliser que la CIM-10.
Son infrastructure ontologique permet un meilleur guidage de l'utilisateur par rapport à la CIM-10.
Le recours systématique à l'utilisation de combinaisons de codes et de codes d'extension rend la CIM finalement cliniquement pertinente.
Avec les combinaisons, n'importe quelle condition peut être codée au niveau de détail désiré.
Les soins primaires, le codage du cancer, la médecine traditionnelle,
et une section pour l'évaluation du fonctionnement sont maintenant inclus.
Des versions spécialisées, comme pour la santé mentale, les soins primaires ou la dermatologie sont produites à partir du noyau commun, la fondation.
Pour l'autorisation des traductions, les demandes doivent être adressées à l'OMS.
Dans la CIM-11, chaque entité pathologique a une description qui donne des descriptions clés et des conseils sur la signification de l'entité/catégorie en termes lisibles par l'homme, afin de guider les utilisateurs.
Les Définitions ont une structure standard selon un modèle avec des modèles de définition standard et d'autres caractéristiques illustrées dans
Propriétés de classification - maladie, trouble, blessure, etc.
Termes - synonymes, autres inclusions et exclusions
Sévérité des propriétés des sous-types - mild, modéré, sévère, ou d'autres échelles
Propriétés de manifestation - signes, symptômes
Propriétés causales - étiologie : infectieux, cause externe, etc.
Propriétés fonctionnelles - impact sur la vie quotidienne : activités et participation
Propriétés de l'affection spécifique - relation avec la grossesse, etc.
Propriétés du traitement - considérations spécifiques au traitement
Critères diagnostiques - définitions opérationnelles pour l'évaluation
Le but de la CIM est de permettre l'analyse comparative internationale, mais cela se heurte à plusieurs difficultés.
Les révisions périodiques de la classification doivent concilier la continuité des définitions (stabilité) tout en l'adaptant à l'évolution du savoir médical (pertinence),
De même, si la classification gagne en précision et en raffinement, cela accroit le besoin d'expertise sur le terrain (moyens et technique de diagnostic).
Il peut alors se produire un décalage de qualité de collecte des données entre les pays selon le niveau de leur service de santé
Par ailleurs, le fait qu'elle ne reprenne pas les « axes » du DSM fait que la liste des diagnostics aurait tendance, selon certaines critiques à s'allonger sans fin et sans qu'on puisse clairement hiérarchiser ceux qui sont pertinents actuellement,
Enfin, la partie des diagnostics pédopsychiatriques (enfants et adolescents) serait insuffisante, ce qui aurait tendance à confondre pédopsychiatrie et psychiatrie
Le Manuel diagnostique et statistique des troubles mentaux (également désigné par le sigle DSM, est un ouvrage décrivant et classifiant les troubles mentaux.
Le manuel évolue initialement à partir des statistiques collectées depuis des hôpitaux psychiatriques la dernière édition, la cinquième, Largement utilisé, le manuel fait toutefois l'objet de critiques.
L'ouvrage est utilisé aux États-Unis et dans le monde par des cliniciens, des chercheurs, des compagnies d'assurances et des entreprises pharmaceutiques, ainsi que par les pouvoirs publics. Les diagnostics de pathologie psychiatrique du DSM, depuis la troisième révision, reposent sur la description de symptômes et de leur articulation en cinq axes. Un bon nombre de professionnels de la santé mentale utilisent le manuel pour déterminer un diagnostic et le communiquer à un patient. Le DSM est également utilisé pour catégoriser les patients à des fins de recherche. DSM-IV a montré que l'ancienne édition était trop utilisée à des fins médicales tandis que la dernière a plus été évaluée pour les recherches
Son contenu est proche du cinquième chapitre de la Classification internationale des maladies (CIM) de l'Organisation mondiale de la santé (OMS), un autre guide communément utilisé dans de nombreux pays. Le système de codage inclus dans le DSM-IV correspond aux codes utilisés dans la CIM-10, bien que certains codes ne correspondent pas car les deux publications n'ont pas été synchronisées lors de leur révision textuelle.
DSM I et II
La Première Guerre mondiale et surtout la seconde implique beaucoup de psychiatres américains — essentiellement psychanalystes — pour faire face aux traumatismes de guerre des soldats Cela a particulièrement changé l'habitude des institutions psychiatriques et les perspectives cliniques traditionnelles. l'Organisation mondiale de la santé publie sa sixième révision du manuel de la Classification internationale des maladies (CIM) incluant pour la première fois une section des troubles mentaux.
Le DSM-I, et le (DSM-II). Ces deux premières éditions du manuel étaient influencées par la psychopathologie psychanalytique. Elles suivaient la structuration entre deux formes majeures de troubles psychiques, les psychoses et les névroses, en héritage de Freud. Celui-ci était cependant particulièrement réservé à l'égard de l'utilisation de son travail dans la psychiatrie américaine.
DSM-III
Le DSM-III est un outil de classification des troubles mentaux C'est depuis cette révision que le DSM a pris le tournant qu'on lui connaît aujourd'hui, théorique comportementaliste et antipsychanalytique.
Par sa conception et la philosophie qui le sous-tend, il marque donc une rupture radicale avec le DSM-II. En effet, le DSM-III se présentant comme purement empirique il est en réalité descriptif, Le DSM-III repose sur un modèle biomédical et évacue toute considération des troubles psychiatriques. l'hystérie est démantelée en plusieurs catégories diagnostiques, de nouvelles catégories comme l'état de stress post-traumatique ou le trouble de la personnalité multiple font leur apparition. Les catégories sont dès lors définies par des critères diagnostiques quantitatifs dans le but d'augmenter la fiabilité du diagnostic et sa reproductibilité.
La définition la plus largement admise, est celle qui fait des sens un système de cellules sensitives, capable de capter et de traduire plusieurs formes d'énergie (stimuli) et de les transmettre au système nerveux central sous forme d'influx nerveux. Ces influx nerveux, L'influx nerveux est ensuite codé sous forme de potentiels d'actions et l'information transmise à des régions spécialisées du cerveau. Selon le type de stimulation, les centres de traitement du cerveau diffèrent. Il existe en effet une zone spécialisée dans le traitement des stimuli olfactifs, visuels, tactiles, etc.
Selon une définition plus large, l'utilisation des sens équivaut à une forme ou à une autre de communication non verbale et corporelle, ce qui amène à mieux comprendre les individus et les sociétés selon les manières dont ils mobilisent les leurs, puisque c'est entre autres par les sens que les humains mettent en ordre leur monde.
Le toucher chez l'humain est le sens le plus fondamental qui apparaît vers le troisième mois de la vie utérine : la peau tactile est le premier-né des organes humains et le plus sensible
Cette troisième édition est une version révisée dans laquelle de nombreux critères et syndromes ont été affinés Seuls les adhérents internationaux de l'APA ont le droit de voter la présence des troubles dans le moutures des futurs DSM.
DSM-III-R
le DSM-III-R est publié en tant que révision du DSM-III, Les catégories sont renommées, réorganisées et des changements significatifs dans les critères ont été effectués. Six catégories ont été supprimées et les autres ont été mises à jour. Les diagnostics controversés tels que les troubles dysphoriques prémenstruels des femmes et troubles de la personnalité masochiste ont été considérés. Le « troubles de l'identité sexuelle » a également été supprimé, mais il est inclus, parmi d'autres, dans la catégorie des « troubles de la personnalité autrement non-spécifiés »
La quatrième édition (DSM-IV), prolongeant et approfondissant le DSM-III, reconnaît 410 troubles psychiatriques. La dernière version utilisée du DSM-IV est une révision mineure de ce texte, le DSM-IV-TR,
DSM-5
Le manuel comprend de nombreux changements, incluant des suppressions proposées dans la section schizophrénie
Système multiaxial
Le DSM-IV, afin de permettre une approche globale et intégrative des patients, rend systématique l'approche axiale des patients porteur de pathologies psychiatriques. Il retient pour cela cinq axes d'analyse incluant :
Axe I : Les troubles majeurs cliniques
Axe II : Les troubles de la personnalité et le retard mental
Axe III : Aspects médicaux ponctuels et troubles physiques
Axe IV : Facteurs psychosociaux et environnementaux
Axe V : Fonctionnement global (tel que mesuré par l'échelle d'évaluation globale du fonctionnement)
Une section est consacrée aux troubles habituellement diagnostiqués pour la première fois pendant la petite enfance, l'enfance ou l'adolescence. Les troubles qui peuvent débuter à tout âge (y compris chez les jeunes) sont décrits dans la section générale. Le nombre minimum de symptômes par diagnostic, la fréquence et la durée des symptômes sont des données quantitatives. DSM-IV individualise des entités diagnostiques qui sont fréquemment associées, comme les troubles anxieux et dépressifs.
Les troubles communs de l'Axe I incluent dépression, troubles anxieux, trouble bipolaire, TDAH, troubles du spectre autistique, anorexie mentale, boulimie et schizophrénie.
Les troubles communs de l'Axe II incluent les troubles de la personnalité : trouble de la personnalité paranoïaque, trouble de la personnalité schizoïde, trouble de la personnalité schizotypique, trouble de la personnalité borderline, trouble de la personnalité antisociale, trouble de la personnalité narcissique, trouble de la personnalité histrionique, trouble de la personnalité évitante, trouble de la personnalité dépendante, névrose obsessionnelle et retard mental.
Les troubles communs de l'Axe III incluent les lésions cérébrales et autres troubles médicaux et/ou physiques qui peuvent aggraver les maladies existantes ou symptômes présents similaires aux autres troubles.
Catégories diagnostiques
Les 16 catégories de troubles mentaux que regroupe le DSM-IV sont :
En conclusion, le DSM-V apparaît comme « une combinaison dangereuse de diagnostics non spécifiques et imprécis, conduisant à des traitements d'efficacité non prouvée et potentiellement dangereux ». Il recommande enfin aux praticiens de garder leur distance avec le DSM
critiques sur le processus de décision quant aux diagnostics qui d'après « de nombreux témoignages de psychiatres ayant participé au développement du DSM » repose sur des « échanges chaotiques qui ne correspondent guère à un processus de décision de nature scientifique étayé sur des faits empiriques En ce sens Allen Frances, affirme — entre autres critiques virulentes — qu'au cours des réunions « ce sont les voix les plus fortes qui prennent l'ascendant lors des controverses suscitées à chaque nouvelle édition du DSM
que « le DSM n'est donc pas le fruit d'un consensus reposant sur des critères scientifiques, mais la conséquence d'un rapport de force qui s'établit suivant des logiques de pouvoir Cela contribue aussi à expliquer l'apparition et la disparition de divers troubles
le DSM, à partir de sa troisième édition, n'a donc pas réussi à faire disparaître la subjectivité et le jugement humain dans le processus diagnostique, permis d'améliorer la fiabilité et la qualité des diagnostics
Limites
Le DSM est en définitive un « catalogue » des pathologies mentales En lien avec la CIM-10, le DSM se veut être international.
Limites :
Étiquetage : l'individu n'est défini qu’à partir d’une attribution.
Catégorisation : si un diagnostic est fait, il faut savoir quelle portée il va avoir, il ne faut pas emmurer les gens, définir ce qui fait que ceci ou cela est un trouble psychique.
Évaluation restreinte : quand un individu se présente et que seul le DSM est à disposition, un diagnostic peut lui être attribué. Il faut d’autres moyens d’évaluer (ne pas oublier de regarder les ressources du patient, regarder ce qui va bien, évaluer le vécu subjectif du trouble, ce qui lui est difficile ou non). Il faut évaluer la personne autant que la maladie.
Risque de céder à une médicalisation excessive de l’état de souffrance : Le DSM se veut athéorique, il ne fait que décrire les maladies.
Comorbidité : pour un profil, il y a la présence simultanée de plusieurs diagnostics, ce qui n'implique pas nécessairement la présence de plusieurs maladies mais l'impossibilité du DSM à émettre un seul diagnostic.
La faiblesse du DSM est son manque de validité. DSM sont fondés sur un consensus sur les groupements de symptômes cliniques, mais sur aucune mesure objective en laboratoire.
Or nous savons qu’à eux seuls, les symptômes indiquent rarement le meilleur choix de traitement
Critiques venant du courant psychanalytique
La valeur clinique du DSM, depuis la troisième édition, est également l'objet de critiques de la part des psychiatres et psychologues cliniciens qui se référent à la psychopathologie psychanalytique
le fait que pour satisfaire l’industrie pharmaceutique, les experts font du disease mongering : en recyclant et renommant d’anciennes maladies, ils inventent des maladies douteuses, appelées vaguement « troubles » pour la plupart
Le DSM-IV se veut dégagé de tous points de vue non fondés scientifiquement mais il fait constamment référence au béhaviorisme qui est une théorie
La situation devient caricaturale : on réduit la souffrance d'un être unique à un symptôme, décrit dans un catalogue et on ignore son contexte social ou personnel Cette logique génère un appauvrissement des entretiens cliniques ; elle néglige l’éventuelle réticence du patient ; elle est porteuse d'idéaux normatifs
la quatrième édition du DSM et les éditions précédentes de la CIM retiennent trois principaux critères pour classer les troubles autistiques : les troubles des interactions sociales, les troubles de la communication et du langage et des comportements, et des activités et intérêts restreints et répétitifs La cinquième édition du DSM regroupe les appellations de cette triade autistique permettant le diagnostic
Terminologie
qui regroupe les troubles liés à une altération (devenue un « déficit ») de la communication et des interactions sociales permet de caractériser en deux parties les troubles du spectre de l'autisme (ou TSA) dans une seule et même catégorie permettant ainsi le diagnostic
un « déficit persistant de la communication et des interactions sociales observés dans les contextes variés » et
un « caractère restreint et répétitif des comportements, des intérêts ou des activités ».
Niveaux de sévérité
Le DSM-5 présente 3 niveaux de sévérité.
Niveau 1 : nécessite un soutien
Niveau 2 : nécessite un soutien important
Niveau 3 : nécessite un soutien très important
Conséquences
Depuis le 1er janvier de cette année La publication de la CIM-11 confirme que ce manuel plus officiel au niveau international présente les deux mêmes catégories que le DSM-5, même s'il existe des divergences pour d'autres critères
Du point de vue de la physiologie, les sens sont les systèmes sensoriels de la perception. Leur fonctionnement, leur classification, et la théorie épistémologique qui soutient leur étude sont abordés par plusieurs disciplines, principalement les neurosciences, mais aussi la psychologie cognitive (ou science cognitive), et toutes les philosophies et études sociales
Longtemps, en Occident, à la suite d'Aristote, on a considéré que l'être humain possède cinq sens. Mais ce chiffre est maintenant souvent porté à sept :
système tactile, relatif aux informations de pression, de toucher, de température, de vibration ou de douleur ;
système visuel, relatif à la couleur, la forme, la distance ou l’intensité lumineuse ;
système auditif, qui localise les sons, différencie leur intensité, fréquence, et renseigne sur le rythme ;
système olfactif, relatif aux substances odorantes par voie directe (flairage) ou rétro-nasale (qui renseigne sur les saveurs) ;
système gustatif, qui discrimine des classes de substances chimiques (amer, acide, sucré, salé et umami) via des récepteurs linguaux ;
système vestibulaire, qui permet la perception du sens de la gravité, et l'ajustement des mouvements corporels et de leur vitesse ;
système proprioceptif (proprioception), relatif aux muscles, viscères, nerfs, articulations, pression sanguine, glycémie, faim, soif...
Les cinq sens, Aristote : la vue, l'odorat, le goût, l'ouïe et le toucher.
Ouïe
L'ouïe ou l'audition est la capacité de percevoir des sons. Le pavillon de l'oreille externe focalise et amplifie l'onde qui passe dans le conduit et met en vibration le tympan humain. Puis il est transmis par la chaîne d'osselets jusque dans l'oreille interne. Le son est transmis au cerveau par les cellules nerveuses Il est ensuite analysé et interprété
Écholocalisation
Particulièrement développée chez certaines espèces animales telles que les chauves-souris et les cétacés, l'écholocalisation est la perception d'un environnement et la localisation d'obstacles à l'aide de l'ouïe, par l'analyse de la réflexion (ou échos) d'ondes sonores ou ultrasonores émises par le sujet.
Certains aveugles utilisent l'écholocalisation pour se déplacer dans leur environnement. Ils émettent des sons, que ce soit en tapant avec leur canne, en tapant du pied ou en produisant des clics avec leur bouche
Proprioception
La proprioception est la perception du corps. C'est une perception à laquelle les gens ont fréquemment recours sans savoir qu'elle existe.
Plus facilement démontrée qu'expliquée, la proprioception est la perception « inconsciente » de l'endroit où se trouvent les différentes parties du corps, et ce à chaque instant (ceci peut être démontré à une personne en lui demandant d'effectuer un mouvement quelconque, comme celui de lever la main, alors qu'elle a les yeux fermés ; la personne en question aura, à chaque instant du mouvement effectué, la connaissance de l'endroit où se trouve la partie du corps déplacée, en l'occurrence sa main ; cette connaissance est permise par la proprioception, puisqu'en principe les autres sens ne peuvent être renseignés à son sujet).
Équilibrioception
Le sens de l'équilibre est principalement lié au système vestibulaire de l'oreille interne. Pour faire simple, les cellules réceptrices ont des cils situés dans une cavité remplie de liquide. Lorsque le liquide bouge sous l'effet d'un changement d'orientation de la tête ou sous l'effet d'une accélération, les cils bougent et les cellules transmettent un signal au système nerveux, renseignant sur les caractéristiques du mouvement.
Chimioréception
La langue compte 3000 papilles gustatives formées de cellules spécialisées dans les saveurs de base : acide ou aigre, amer, gras salé, sucré et umami. On croyait autrefois que chaque saveur disposait d'une partie de la langue qui lui aurait été réservée, toutefois des études ont démontré le contraire par application d'une goutte de substance salée ou sucrée au même endroit : le sujet parvenait à reconnaître la saveur quelle que soit la localisation de la goutte, la « cartographie des saveurs » est donc obsolète Les cellules réceptrices captent les stimulations et transmettent au cerveau les signaux correspondants. Ce qui permet de ressentir le goût.
Odorat
Le nez est un organe très sensible qui est capable de percevoir des milliers d'odeurs. L'olfaction est le deuxième des sens après le goût à utiliser une réaction moléculaire donc « chimique ». Si on respire par la bouche, l'air passe directement dans la gorge et une toute petite partie arrive alors aux cellules olfactives. Ces cellules vont transmettre des impulsions informatives au nerf olfactif qui envoie un signal électrique au cerveau, lui permettant de reconnaître l'odeur par le système olfactif.
Thermoception
La thermoception est le sens de perception de la chaleur et de l'absence de chaleur (froid) par la peau. C'est le premier sens non identifié explicitement par Aristote.
Réception polymodale
Le principal exemple de réception polymodale est la nociception : c'est la perception des stimulus lésionnels ou potentiellement lésionnels. Elle est associée à la douleur. Elle peut être regroupée en un à trois sens, ceci dépendant de la méthode de classification. Les trois types de nocicepteurs sont :
les récepteurs cutanés au niveau de la peau ;
les récepteurs somatiques au niveau des articulations et des os ;
les récepteurs viscéraux au niveau des organes viscéraux.
L'hypersensibilité, en psychologie, est une sensibilité plus haute que la moyenne, provisoirement ou durablement, pouvant être vécue avec difficulté par la personne concernée elle-même ou perçue comme « exagérée », voire « extrême », par son entourage Dans le registre sensoriel, l’hypersensibilité peut concerner un seul ou plusieurs des sens du système sensoriel.
Les caractéristiques de cet ensemble découlent d'une plus forte réactivité à une même stimulation, ce qui a des aspects positifs — Jung parle de « caractère enrichissant » — et des aspects négatifs, comme une sensibilité accrue à la peur.
Le terme « individu hautement sensible » est ici traduit par « hypersensible ».
Une même personne (avec autisme par exemple) peut être à la fois hyposensible à certains stimuli (ex. : température de l'eau, avec brûlures possibles), et présenter une hypersensiblilité très marquée pour d'autres stimuli (typiquement : au bruit, à l'agitation
Cette co-existence entre hyper- et l’hyposensibilité chez un même individu semble fréquente chez les autistes :
L'hyposensibilité évoque une intensité inhabituellement basse de la perception pour un ou plusieurs canaux sensoriels, ce qui « implique un niveau de stimulation de l’environnement très élevé pour initier une réponse. Selon les comportements stéréotypés et les autostimulations, fréquemment observées dans l’autisme, qu’il appelle « sensorismes », constitueraient des mécanismes d’autoprotection inconscients des personnes avec autisme pour lutter contre les hypo- et les hyper-sensibilités
Une même personne peut être hypersensible pour un sens (l'ouïe par exemple) et hyposensible pour un autre. Ceci est fréquent chez les autistes.
la timidité et l'introversion ne doivent pas être confondues avec l'hypersensibilité, même si ce sont des réponses possibles, car il existe des hypersensibles extravertis et la thérapie peut révéler une tendance refoulée à l'extraversion chez certains hypersensibles
Lien entre sensibilité élevée et pathologie
c'est un caractère enrichissant, qu'on ne peut pas considérer en lui-même comme pathologique, Néanmoins, si cette sensibilité a des conséquences destructrices pour le sujet, on doit bien admettre qu'on ne peut pas la considérer comme bien normale
la sensibilité élevée n'est ni une maladie ni une anomalie Elle n'a donc pas besoin d'être soignée. « Devenir humain est une conquête quotidienne, affirme-t-il, et celle-ci passe par la fierté d'être sensible
En tant que telle, l'hypersensibilité n'est ni une maladie ni un symptôme précisément défini. Ce mot fait plus simplement partie du jargon paramédical. Toutefois, elle peut être liée à une autre cause de souffrance qui peut nécessiter dans ce cas une prise en charge psychologique.
Puisqu'il ne s'agit pas d'une maladie, il n'y a pas lieu de parler de thérapie destinée à soigner ou corriger l'hypersensibilité à proprement parler. On mentionnera des thérapies exclusivement pour des troubles identifiés distinctement à côté de l'hypersensibilité, comme les difficultés sociales, les troubles de l'humeur, l'angoisse, le stress post-traumatique, etc.,
Certains auteurs envisagent néanmoins de « traiter » l'hypersensibilité d'une manière ou d'une autre. En ce sens, les techniques et thérapies existantes sont jugées adéquates du moment qu'elles ne tentent pas de réprimer l'hypersensibilité mais, au contraire, tant qu'elles permettent à l'hypersensible de vivre avec son « excès » de ressentis, de l'assumer et de trouver des occupations mettant en valeur ce qui a pu lui sembler une source de problèmes
la haute sensibilité serait liée à un trait génétique conservé pendant l'évolution par un grand nombre d'espèces animales, laissant supposer qu'il a certains avantages ; mais elle également l’existence d'« interaction » avec l'environnement durant l'enfance comme cause de ce tempérament hypersensible.
générale, après une enfance difficile, un hypersensible s'est construit un ensemble de protections psychologiques lui permettant de se protéger ou d'éviter un monde perçu comme excessivement violent. Ces mécanismes d'adaptation, à leur tour, peuvent générer une mauvaise adaptation sociale des difficultés relationnelles de la souffrance et de la frustration
la sensibilité élevée n'est pas génétique, mais découle de l'histoire singulière de chaque personne, comprenant les influences possibles du contexte familial, de la généalogie et de la société.
Perception et réaction
Un premier défaut pointé est le fait que la réaction comportementale à un stimulus n'est pas nécessairement proportionnelle à son intensité. Une autre lacune pointée est le raccourci fait dans l'assimilation d'Aron entre stimuli sensoriels avec ceux environnementaux et sociaux, les premiers demandant bien moins de ressources cognitives que les seconds. Elle assimile également la sensibilité aux seuil de détection et au seuil de discrimination.
Tempérament et personnalité
Le terme « tempérament » faisant référence à une forme de caractère « définitif », Stéphanie Aubertin s'oppose à cela en notant que la sensibilité est susceptible d'évoluer au fil de la vie ou selon le contexte et que l'hypersensibilité n'est donc ni une fatalité, ni définitive.
Les chercheurs suggèrent que le modèle théorique de l'hypersensibilité se superpose fortement aux traits de personnalité établis par le modèle du Big Five, notamment ceux de névrosisme et d'ouverture à l'expérience. Toujours selon ces chercheurs, ces traits suffisent déjà à expliquer la capacité de reconnaissance des émotions.
Justifications défaillantes
Aubertin critique Elaine Aron sur le fait que celle-ci justifie des temps de réponses plus long aux tâches effectuées dans ses études de la part de sujets définis comme hypersensibles selon son questionnaire comme « une pause pour réfléchir », mais également qu'Aron justifie un temps de réponse plus court de cette même catégorie de personnes car elles auraient besoin de moins de stimuli pour répondre. Est donc dénoncé le fait que tout motif pourrait justifier la sensibilité élevée détectée au préalable selon Elaine Aron.
Questionnaire
Le questionnaire d'hypersensibilité d'Aron est noté comme effectivement validé par des analyses factorielles (il mesure bien « quelque chose »), mais rien n'indiquerait
Polysémie
Nous pouvons retrouver le caractère polysémique de l'hypersensibilité dans le DSM-5, où le mot est utilisé 16 fois : une fois pour « hypersensibilité au rejet » (trouble dysphorique prémenstruel), trois fois pour « hypersensibilité aux jugements négatifs » (trouble de la personnalité évitante), deux fois non spécifiées (personnalités paranoïaque et schizotypique), une fois pour une « hypersensibilité personnelle » (personnalité Borderline), quatre fois pour spécifier une hypersensibilité aux neuroleptiques, une fois pour spécifier une « hypersensibilité des capteurs médullaires du dioxyde de carbone », et enfin quatre fois pour une hypersensibilité à la lumière ou au bruit.
Le mot hypersensible est utilisé deux fois, une fois pour « hypersensible à la lumière vespérale » (trouble de l'alternance veille-sommeil) et une fois pour définir un des niveaux d'empathie sur l'échelle du niveau de fonctionnement de la personnalité L'hypersensibilité n'est donc bel et bien pas une pathologie et n'est pas non plus un symptôme précisément fixé par une définition unique.
Dangers
La polysémie du mot mêlée à certaines lacunes théoriques et méthodologiques du concept ainsi que son intérêt médiatique permet à beaucoup de personnes de s'y identifier (ou d'identifier une autre personne) et cela très facilement, De plus, une caractéristique redondante de l'hypersensibilité est qu'elle serait une souffrance cachant en réalité un potentiel exploitable lorsque cet attribut serait maîtrisé par l'individu
A cela vient s'ajouter le caractère définitif allant souvent de pair avec des définitions communes de l'hypersensibilité, pouvant mener certaines personnes à ne pas travailler sur eux ou à ne pas soigner une éventuelle pathologie sérieuse.
Johann Friedrich Karl Asperger, dit Hans Asperger (né le 18 février 1906 à Hausbrunn et mort à Vienne le 21 octobre 1980), est un psychiatre autrichien, auteur d'une étude pionnière sur l'autisme. Son nom a été donné au syndrome d'Asperger, une forme d'autisme définie en 1981 par Lorna Wing.
Son rôle dans l'Autriche annexée par les nazis est longuement resté méconnu, jusqu'à l'étude de documents d'archive. Ceux-ci démontrent qu'Hans Asperger, qui travaillait sous la direction de son ami Franz Hamburger, a collaboré avec le gouvernement nazi, bénéficié d'avancées de carrière grâce à la fuite des médecins juifs, et a participé à la sélection d'enfants envoyés vers Am Spiegelgrund, où certains d'entre eux ont été tués. La question de son adhésion personnelle à l'idéologie nazie reste controversée,
les informations biographiques disponibles à propos de Hans Asperger sont limitées En dépit de son rôle dans l'étude de l'autisme, les documents d'archives le concernant ont longuement été ignorés Aussi les diverses opinions émises à son sujet restaient-elles invérifiables
Certaines informations biographiques proviennent de sa fille Maria Asperger-Felder, qui les a délivrées en 2006, à l'occasion de ce qui aurait été le 100e anniversaire de la naissance de son père.
ces sources « véhiculaient une image non critique et parfois apologétique du rôle d'Asperger pendant la période nazie
Les pigeons ou les dauphins sont capables de percevoir les lignes du champ magnétique terrestre ou ses variations.
Une pseudo-science, la métapsychique, a proposé à différentes époques, un sixième sens qui permettrait la communication entre l'être vivant et d'autres êtres vivants, sans que soient connus les organes de perception, les énergies et mécanismes médiateurs, ou les organes effecteurs, à la source de ces phénomènes.
Mais le terme de sens peut revêtir deux aspects différents suivant que l’on soit en présence d'une communication immédiate (donc instinctive) ou médiate (donc rationnelle, scientifique). Les sens sont les voies de la perception, un lien reliant la conscience et l'organisme au monde extérieur et à ses organes et qui lui permet de reconnaître, grâce à l'interprétation donnée par la pensée et la connaissance, les informations qui, parmi l'ensemble de celles lui parvenant, pourraient lui être utiles.
Certaines cultures ne divisent pas leur perception du monde selon cinq sens, elles peut faire primer l’importance d’un sens sur un autre, et associer des valeurs individuelles et sociales différentes aux sens
De par cette définition assez vaste, plusieurs sens peuvent être identifiés.
Tous les animaux présentent des récepteurs sensoriels leur permettant de percevoir le monde autour d'eux, incluant plusieurs de ceux précités, valables pour les humains. Cependant, les mécanismes et capacités peuvent varier.
Par exemple, les chiens ont un sens de l'odorat plus fin que chez les humains, bien que le mécanisme mis en jeu soit le même. Les mites ont des récepteurs olfactifs sur leurs antennes, et des récepteurs aux vibrations sonores sur leurs ailes. Les cténophores ont un récepteur de l'équilibre (un statocyte) qui fonctionne très différemment des canaux semi-circulaires mammaliens.
La partie la plus importante de l'œil est le globe oculaire qui est le véritable organe de la vue. Le globe oculaire a la forme d'une sphère, et il est formé de trois couches de tissus superposées :
la sclère ;
la choroïde avec l'iris et la pupille, qui forment ensemble l'uvée ;
la rétine où se trouvent les cellules nerveuses d'où part le nerf optique.
Électroperception
L'électroception (ou électroréception), le plus significatif des sens non humains, est la capacité à détecter les champs électriques. Beaucoup d'espèces de poissons, requins, raies, peuvent sentir des modifications du champ électrique dans leur proximité immédiate. Certains poissons sentent passivement des changements dans le champ électrique proche ; d'autres génèrent le leur, d'intensité faible, et peuvent sentir la répartition du potentiel sur leur surface corporelle ; d'autres encore utilisent ces capacités de génération et de sensation pour la communication sociale.
Le seul ordre de mammifères connu pour présenter la faculté d'électroception est l'ordre des monotrèmes, parmi lesquels l'ornithorynque a le sens le plus développé
Les humains (et probablement les autres mammifères) peuvent détecter les champs électriques indirectement, par le biais de l'effet qu'ils provoquent sur les poils. Par exemple, un ballon électriquement chargé exercera une force d'attraction sur des cheveux, ce qui peut être senti par le toucher, et être identifié comme provenant d'une charge électrique (et non du vent ou autre chose).
🟢
Approches psycho-éducatives
Des interventions cognitives et comportementales, notamment l'Analyse du Comportement Appliquée (ABA), dont est aussi dérivé le Modèle de Denver, le TEACCH, et le PECS sont proposées pour aider les personnes autistes à gagner en autonomie et à développer des habitudes de communication
il existe quelques preuves d'efficacité des groupes d'habiletés sociales pour les personnes entre 6 et 21 ans
Les personnes militant pour la neurodiversité sont globalement opposées aux approches de type ABA, qu'elles jugent non éthiques il est aussi suggéré qu'une exposition répétée aux approches de type ABA génère un trouble de stress post-traumatique chez la personne autiste
Médicaments
il n'existe pas de traitement curatif » de l'autisme
Aucun traitement médicamenteux n'est recommandé officiellement le niveau très faible voire l'absence de preuve d'efficacité des ISRS (avec effets délétères constatés des preuves contradictoires concernant les antidépresseurs tricycliques
(là aussi avec effets secondaires délétères et l'absence totale de preuve d'efficacité des injections intraveineuses de sécrétine
Certains traitements médicamenteux ciblent les troubles associés à l'autisme.
La prescription de mélatonine pourrait améliorer significativement le temps de sommeil total
Un nombre important de personnes autistes étant épileptiques, elles reçoivent des médicaments anti-épileptiques afin de prévenir les crises
Des améliorations du langage et de la communication ont été constatées grâce à l'utilisation d'une forme de vitamine B9 (l'acide folinique),
L'influence psychanalytique remise en question
Le rapport de la psychanalyse avec la notion d'autisme est complexe et fortement relié aux travaux des précurseurs de la psychanalyse (Jung, Freud ou Bleuler, cf. l'Histoire de la notion d'autisme).
Dans l'ensemble, l'approche psychanalytique reste source de vives controverses, qu'elle concerne les théories sur l'origine des troubles autistiques ou leur prise en charge
Des associations de familles militant pour que l'approche psychanalytique soit considérée comme « non recommandée » ont exprimé leur déception et certaines associations de psychanalystes ont protesté
Faisant suite à la dénonciation répétée de la psychanalyse dans la prise en charge de l'autisme une proposition de résolution parlementaire visant à l'interdire a été formulée soutenu publiquement par le porte-parole du collectif Autisme
Cette controverse est notamment centrée sur l'importance des théories psychanalytiques culpabilisant le rôle de la mère dans le développement de l'autisme.
Notamment les théories émises par Bruno Bettelheim, qui a proposé l'idée de « mère réfrigérateur » en s'inspirant des propos de Leo Kanner pour désigner des mères comme cause de l'autisme de leur enfant
Bien qu'il prône une prise en charge psychoéducative et qu'il exclue de sa définition de l'autisme les causes innées (là où Kanner fait le contraire il reste le symbole du refus d’entendre la part génétique, innée de ces troubles.
Ses théories ont souvent été reprises en psychanalyse de l'autisme
Les faibles possibilités de prise en charge autre que celles d'inspiration psychanalytique ont été dénoncées par des associations de parents, accusant les théories psychanalytiques de guider un nombre important de pédopsychiatres français
Ces théories culpabilisantes seraient progressivement abandonnées par les praticiens d'inspiration psychanalytique actuels, certains prenant acte des avancées scientifiques et mettent l'accent sur une position éthique de respect de la souffrance des patients et de leur famille
pédopsychiatre, ont souligné le manque de fondement scientifique de la psychanalyse et récusé sa prétention à guérir une maladie biologique comme l'autisme
l'approche psychothérapeutique de l'autisme, qu'elle soit d'inspiration psychanalytique ou d'inspiration cognitivo-comportementale, donne des améliorations significatives de l'état des enfants autistes
L'étude fait l'objet d'une bonne réception de la part de divers psychiatres, psychologues cliniciens et psychanalystes mais également de critiques venant du cognitiviste Franck Ramus
Cette étude n'est qu'un premier pas, et montre le besoin d'un plus grand nombre d'analyses scientifiques rigoureuses à grande échelle pour estimer les effets de la psychothérapie, qu'elle soit d'orientation psychanalytique ou autre, dans la prise en charge de l'autisme.
Traitements « alternatifs » et dérives
L'autisme reste mal compris.
Ceci peut entraîner une grande anxiété dans les familles, et un douloureux phénomène d'impuissance
Ce contexte a favorisé le développement de méthodes « alternatives » soi-disant miracles, souvent facturées à des prix très élevés
Une pseudoscience s'est développée autour de l'autisme, de ses causes hypothétiques, de son accompagnement, voire d'une supposément possible « guérison », impliquant un grand nombre de thérapies non conventionnelles.
Certaines sont basées sur des régimes
De prétendus traitements oraux se révèlent parfois dangereux et parfois simplement inefficaces
La « thérapie par chélation » a entraîné la mort d'un enfant autiste et de même que l'exposition à l'oxygène en caisson hyperbare, n'est pas recommandée
Certaines méthodes classées comme alternatives ou complémentaires montrent des bénéfices pour certains enfants.
C'est le cas par exemple du contact avec des chevaux (encore à confirmer c'est aussi le cas de méthodes dites sensorielles basées sur l'eau (le snoezelen, la natation, la plongée sous-marine et d'autres méthodes de balnéothérapies ou d'hydrothérapie durant 10 à 14 semaines sont appréciés de nombreux autistes qui peuvent trouver une source d'amélioration de confiance en soi, des interactions sociales et des comportements mais certaines formes d'hydrothérapie sont inadaptées aux cas d'hypersensibilité proprioceptive, faisant que des stimuli externes appliqués avec une force excessive (ex. : jet d'eau)
« conduisent souvent à une réponse des systèmes de stress qui ne correspond pas aux capacités de compensation du corps
Mais beaucoup de méthodes ont un niveau de preuve encore insuffisant et certaines n'ont simplement pas pu démontrer la moindre efficacité
Grâce aux importants revenus générés par ces pseudo-thérapies, de puissants instituts se sont formés aux États-Unis pour promouvoir et centraliser ce genre de méthodes appuyés par une communication et un lobbyisme actifs, Cette communication est généralement basée sur des témoignages isolés et invérifiables et une grande force de persuasion, parfois assortis de fausses études scientifiques En réponse, la FDA américaine a publié un guide intitulé « Beware of False or Misleading Claims for Treating Autism et des associations d'aide aux victimes se sont montées, comme la Autism Rights Watch, en lien en France avec la Mission interministérielle de vigilance et de lutte contre les dérives sectaires
🟢
🔴
(Y aurait-il moins d'autisme autour de lieux où il y a moins de pollution de l'air Sur 129 222 naissances dans la région métropolitaine de Vancouver de 2004 à 2009, suivies jusqu'en 2014 : 1 921 enfants (soit 1,5 % de ces naissances) ont été diagnostiqués TS porteurs TSA. Ces données ont été croisées avec sur une modélisation géographique rétrospective de l'exposition à trois polluants connus et suivis : particules de moins 2,5 µm (PM2.5), monoxyde d'azote (NO) et dioxyde d'azote (NO2-, calée sur la proximité de l'habitation avec un espace vert lors de sa grossesse.
Les auteurs ont conclu que « l'exposition prénatale aux espaces verts était associée à une probabilité réduite de TSA », mais sans preuves que cela soit dû à une moindre exposition à la pollution atmosphérique.
l'autisme n'est génétique qu'à hauteur de 50 %, à parts égales avec les facteurs environnementaux. Il est cependant difficile de distinguer les facteurs génétiques et les facteurs environnementaux, l'autisme étant un caractère phénotypique issu d’interactions complexes. 50 % des cas d'autisme s'expliqueraient par des mutations de novo.
Les structures cérébrales caractéristiques étant acquises durant la grossesse il n'est pas possible d'isoler l'effet de l'environnement en étudiant les jumeaux monozygotes qui sont exposés aux mêmes conditions de développement prénatal. Les interactions des gènes liés à l'autisme entre eux et avec l'environnement sont complexes : un même profil génétique et le même environnement peut produire des individus autistes et neurotypiques, les jumeaux monozygotes n'étant pas systématiquement autistes ou neurotypiques. Dans les années 1990, l'autisme était considéré comme une maladie polygénique de 5 à 15 gènes à transmission non mendélienne. Or, depuis les années 2000, plusieurs centaines de gènes à transmission mendélienne impliqués dans l'autisme ont été mis en évidence. L’autisme serait lié à 1 034 gènes différents,
🔴
🟠
Les parents peuvent percevoir des premiers signes de l'autisme durant les deux premières années de leur enfant, par l'absence ou la présence d'un certain nombre de comportements, par exemple : une impression d'indifférence au monde sonore et aux personnes ; l'absence de tentative de communication avec l'entourage par les gestes ou le babillage ; la difficulté à fixer le regard ou un regard périphérique. Le décalage avec les comportements des autres enfants apparaît de plus en plus important avec l'avancée en âge, néanmoins certains enfants se développent d'abord « normalement », puis « régressent » soudainement.
Des indices laissaient penser que des maladies inflammatoires de l'intestin (MII) parentales puissent prédisposer l'enfant à naître à l'autisme. En combinant quatre approches complémentaires, les auteurs y estiment « avoir trouvé des preuves d'un lien de causalité potentiel entre les MICI parentales, en particulier maternelles, et l'autisme chez les enfants. Un dérèglement immunitaire périnatal, une malabsorption des micronutriments et une anémie peuvent être impliqués
Facteurs environnementaux
Quelques facteurs ont été positivement corrélés à la survenue d'un TSA :
L'exposition in utero à l’acide valproïque, un antiépileptique formellement contre-indiqué pendant la grossesse
L'hypothyroïdie maternelle non équilibrée durant le premier trimestre de sa grossesse
Les situations de détresse respiratoire aiguë ou d'hypoxie en périnatal
L'exposition de la mère à des maltraitances durant son enfance
La prématurité, les petits poids de naissances, et l'accouchement par césarienne
L'hypothèse qu'une concentration amniotique élevée de testostérone lors d'un stade critique de la vie fœtale, qui pourrait favoriser un cerveau « hyper-masculin », alors source de comportements stéréotypés masculins tels que la systématisation, la construction de machines, et d'une moindre capacité d'empathie et de vie sociale (qualités supposées plus féminines selon cette approche) et l'apparition de traits autistiques, fait l'objet de diverses études. qu'une exposition fœtale à la testostérone peut modifier certaines structures cérébrales mais elle a été au moins remise en cause en par une étude qui n'a trouvé aucun effet de la testostérone sur l'empathie
L'exposition fœtale à l'hyperglycémie lors d'un diabète gestationnel
La proximité du lieu de résidence de la mère durant la grossesse avec des champs traités par des insecticides de la famille des organophosphorés et des pyréthroïdes
Dépistage précoce (12-30 mois)
Environ la moitié des parents d'enfants présentant un trouble du spectre de l'autisme remarquent la présence de comportements inhabituels chez leur enfant avant l'âge de 18 mois, et environ les 4/5 avant l'âge de 24 mois. La présence d'un ou plus des signes d'alerte suivant nécessite de consulter un médecin spécialiste
absence de babillage à 12 mois ;
absence de gestes communicatifs à 12 mois ;
aucun mot isolé prononcé à 16 mois ;
aucune phrase de deux mots prononcée spontanément à 24 mois (à l'exception de phrases écholaliques) ;
toute régression des capacités sociales et langagières, quel que soit l'âge de l'enfant.
🟠
L'hypothèse qu'une concentration amniotique élevée de testostérone lors d'un stade critique de la vie fœtale, qui pourrait favoriser un cerveau « hyper-masculin », alors source de comportements stéréotypés masculins tels que la systématisation, la construction de machines, et d'une moindre capacité d'empathie et de vie sociale (qualités supposées plus féminines selon cette approche) et l'apparition de traits autistiques, fait l'objet de diverses études. qu'une exposition fœtale à la testostérone peut modifier certaines structures cérébrales mais elle a été au moins remise en cause en par une étude qui n'a trouvé aucun effet de la testostérone sur l'empathie
L'exposition fœtale à l'hyperglycémie lors d'un diabète gestationnel
La proximité du lieu de résidence de la mère durant la grossesse avec des champs traités par des insecticides de la famille des organophosphorés et des pyréthroïdes
L'hypothèse qu'une concentration amniotique élevée de testostérone lors d'un stade
Perceptions de la famille
Dans le processus d’un diagnostic du trouble du spectre de l’autisme, les parents sont aussi affectés par cette situation de plusieurs manières
Selon une étude les pères ont peu de connaissances sur le trouble de l'autisme. Ce qu'ils savent généralement sont les problème de language ou d'audition, sur les interactions sociales, des retards de développement et des intérêts particuliers.
La transition vers les services est difficile à cause d’un manque d’accessibilité, mais les pères sont habituellement satisfaits des services reçus malgré tout. Ces services ont des effets positifs pour l’enfant sur le langage, la communication, la motricité, les comportements et l’autonomie.
Des mères croient que l'intégration scolaire d'enfant autiste est influencée par le personnel scolaire car il est important d'avoir les connaissances et compétences pour leur besoins.
L'environnement à aussi une influence sur l'intégration et qu'il est apportant d'avoir un accès aux services et au besoins.
Il est encore plus facile de ciblé les besoins de l'enfant quand un proche à connaissance des besoins spécifiques de l'enfant.
L'autisme est officiellement reconnu comme générant un handicap, cependant une évolution est possible notamment en matière d'autonomie.
Par exemple la figure Donald Grey Triplett, premier enfant diagnostiqué autiste par Leo Kanner.
Sortie des critères diagnostiques
Certains diagnostique de l'autisme peuvent être interprété comme des guérison. Certain enfants ne rencontre plus les critères diagnostiques à l'âge adulte car la plupart on appris à "masquer" leur traits afin de paraître acceptable socialement ce qui n'est pas sans conséquence (troubles dépressifs, troubles anxieux). Ils apprennent à mimer et se fondre dans la masse afin d'avoir l'air "normaux" ou "guéris" en grandissant.
Intégration sociale et professionnelle
Les difficultés de l'autisme et l'exclusion sociale font qu'ils sont peu intégrées dans la société :
Accès à l'école, à un travail...il es difficile pour eux de faire des liens relationnel, car une part ne peuvent pas parler, n'ont pas de travail régulier et on sont dépendants des parents.
Une étude à montré que les situations de stress des familles sont nombreuses et douloureuses.
Dépistage
Le diagnostic se fonde sur divers arguments clinique avec la collaboration des proches tout patient ou représentant légal du patient à le droit de s'opposer au diagnostic y compris "en contre" qui n'a pas été réalisé selon les recommandations et à demandé un diagnostic d'autre praticien.
Des indications sur les signes d'alerte qui indiquerai un autisme pendant l'enfance son proposé.
Un dépistage peut être effectué à partir de 18 mois assez fiable (test M-CHAT) par le pédiatre ou les parents.
En cas de doute il est recommandé d'effectuer un teste plus précis (ADOS et ADI-R.
Le dépistage permet une mise en place permet une mise en charge adaptée au plus tôt et d'augmenter les chances de développement de l'enfant.
La Fondation FondaMental, bien qu'acceptant la notion de trouble du spectre de l'autisme et de syndrome d'Asperger, considère que l'autisme est « assimilé aux maladies mentales.
En France le retard en matière d'autisme est principalement à cause d'utilisation persistante de la psychanalyse.
Parmi les sujets de controverse, on trouve la notion de psychose, le rapport à la psychanalytique et les déduction sur le rôle des parents.
Les résultats des premières structures expérimentales de « Centres Experts sur ABA » de l'eutisme 3 montrent que que très peu des enfants autistes ont intégré l'école ordinaire et les résultats sont en deçà des études originelles des méthodes comportementales.
Droit international
La France a été épinglée par l'ONU plusieurs fois à propos des situations des autistes dans le pays. L'ONU dénonce la violation des droits des autistes. En cause : l'utilisation persistante de la psychanalyse. L'ONU a demandé à la France de cesser l'institutionnalisation d'un enfant autiste dans un hôpital psychiatrique. Il y à très peu de données officielles aux personnes autistes ainsi que les soins psychiatriques sans consentement. L'ONU s'est dit préoccupée encore du fait que les autistes soient particulièrement concernés par le recours aux médicament et à la surmédication en France. L'ONU constate que les autistes en France soient soumis à des traitements qui visent à « faire disparaître » leur autisme, ce qui constitue une atteinte à leur identité.
📝❌
0 notes
Text
Elevate your liver health with Portal Triad Clinic. Our renowned liver specialists in Chennai provide cutting-edge diagnostics and personalized treatment plans. Experience excellence in hepatic care for a vibrant and healthier life.
0 notes
Text
Thoughts on the DSM
I’m going to preface this by saying that I am not a psychologist. I have no formal training whatsoever. But man is there a lot of mental illness in my life. I both have mental illness and have encountered it in others. So I have thoughts.
The DSM is The Diagnostic and Statistical Manual of Mental Disorders. Homosexuality used to be listed in the DSM, but it has since been removed. And I no longer know if such a decision serves us well because I have yet to meet a single LGBT person who can say they came from a household without sexual abuse. So...hm.
But uh, I’m just going to give a brief overview of what I know about mental illness and personality disorders.
ADHD almost feels like a gateway into further mental illness. Everyone seems to have it. And that’s bad because attention is how you control your life. If you can’t control your attention, you can not be the master of your destiny.
I know a lot about narcissism and the dark triad (narcissism, psychopathy, and sociopathy). That’s how we classify evil these days. Of course not every narcissist is the pinnacle of evil...yet. I don’t know. I do know that the narcissist worships a false self, whereas the true self appears to be a desiccated skeleton under the floorboards of their soul. This false self will never be satisfied with what it has. The narcissist also likes to construct a web of “flying monkeys” (people who prop up the narcissist) and creates an environment of triangulation and group gaslighting.
The only reason I can fathom that we have evolved to have psychopaths and sociopaths among us is that if we were ever under attack, sociopaths and psychopaths could still function among the wreckage. And if they were loved well, they may look around and decide to help the rest of us.
I think psychopaths are actually filed under Antisocial Personality Disorder these days. And then Borderline Personality Disorder (BPD) is the female version of Antisocial Personality Disorder. I’ve encountered BPD and it’s pretty intense. From what I can tell, people with BPD - when they sense they will be abandoned - will be triggered into a psychopathic rage and man...it’s a lot. It can get pretty abusive.
Honestly I’ll take a narcissist over someone with BPD. Maybe it’s because I grew up with narcissists and I know how to maneuver around them. Maybe I just don’t like psychopathic rage. But you have to push a narcissist pretty far to get them to fly into a psychopathic rage. You have to utterly destroy their reputation. Whereas with BPD it can happen at the drop of a hat.
Finally, we get to schizophrenia and Dissociative Identity Disorder. These two are scary for completely different reasons. This is the part of the DSM where reality tends to unravel. And colloquially, informally, it’s identified as “hearing voices.”
Now for me, someone with DID, all those voices are me. That’s just me talking to myself. I am quite literally talking to someone else who is still somehow me. It still shocks me how different and distinct they are from me. Incredible. In fact, I am so damn dissociated, that I have to make the effort to tell different parts of myself certain things to get the information across even though we share the same brain. I’ve been resisting this because it’s just so damn absurd, but it has to happen.
Schizophrenia...I don’t know much about that. I do know schizophrenia has some genetic component whereas DID is induced through trauma. It is possible to recover from DID, whereas schizophrenia can be managed at best.
Sometimes I wonder if what we call schizophrenia is an ability that was evolved to protect us and we now live in some sort of hell world where this ability is seen as the most shameful thing one could possibly possess. But that’s just silly. Ha ha.
I mean, even if that was true, just because you had it wouldn’t mean you are automatically prepared to help others. Just like having 10/20 vision doesn’t make you a great pilot.
This essay got pretty weird. Although the world’s pretty weird these days. So let’s just take a few more steps into that weirdness, eh?
One of the best ways we can tell we’re alive and exist is with Descartes proclamation: “I think, therefore I am.”
With DID, I can’t always tell when or what I’m thinking. It’s an existential nightmare. And my version of it is pretty advanced. With “naturally-occurring” DID, there’s a lot of amnesia that happens when different alters take over. So eventually the host should figure out that this isn’t normal. You were there on Tuesday doing dishes and now it’s Friday and you’re in a ditch. Something is going on.
As for me, I’ve never had that experience which made it very, very hard to detect. I, the host, am always present in my waking life. But like other people with DID, I can’t recall much of my childhood. I can only recall snippets of all my childhood homes (my family moved around a lot) and apparently that’s not normal.
What I’m trying to relay to you, internet people, is that DID is a great way to enslave another without their awareness.
0 notes
Text
Outer-membrane-acting peptides and fat II-targeting prescription medication cooperatively eliminate Gram-negative pathoenic agents.
Venous blood samples had been attracted regarding malaria diagnosis (microscopy and also RDT), way of life and handle blood rely. Left over spots had been stored with -80 levels H as well as useful for extra RDT investigation as well as PCR. A good RDT focusing on both PfHRP2 along with Pf-pLDH has been executed upon most trials regarding direct assessment of diagnostic precision with microscopy since guide technique. PCR ended up being executed to discover false-positive RDT benefits. Results: Throughout 376 regarding 694 (Fifty four.2%) integrated kids, malaria had been microscopically confirmed. Level of sensitivity, uniqueness, good predictive benefit (PPV) and also damaging predictive price ended up A hundred.2, 70.Being unfaithful, Sixty nine.Some and A hundred.0%, correspondingly with regard to PfHRP2-detection along with Ninety eight.Several, Ninety four.2, Ninety one.Half a dozen and also 99.1%, correspondingly for Pf-pLDH-detection. Specificity as well as PPV were considerably lower pertaining to PfHRP2-detection (p < 2.001). For both discovery antigens, specificity was most affordable for youngsters 1 to 5 years and inside the rainy season. Pay per view for antigens has been highest within the wet period, because of greater malaria prevalence. Bogus positive PfHRP2 effects were related to preceding anti-malarial remedy as well as good PCR benefits (98/114 (86.0%) trials analyzed). Conclusion: Among kids showing along with significant febrile sickness in the in season hyperendemic malaria tranny location, the actual research observed equivalent level of responsiveness however decrease specificity and Cpv regarding PfHRP2 in comparison with Pf-pLDH-detection. Further reports need to assess the analytic precision as well as protection associated with an appropriate Pf-pLDH-detecting RDT in field options and if enjoyable, replacement of PfHRP2 by simply Pf-pLDH-detecting RDTs is highly recommended.All of us statement the case of your 20-year-old man which has a unusual constellation associated with imperfections * a practical thyroglossal cyst along with concurrent Etomoxir ectopic hypothyroid inside the floorboards of the oral cavity, lacking any orthotopic thyroid gland. To our information, here is the 3rd these kinds of statement inside the otolaryngology materials. It is important to know about the possibility of concurrent ectopic thyroid and thyroglossal cysts even without the a good orthotopic thyroid gland. Nearly all described installments of thyroid ectopy arise with the lower dialect. The occurrence of a great ectopic thyroid within the flooring with the mouth area is both strange instead of open for you to scientific examination. Even though there's very good usage about atomic imaging, the ectopic thyroid might be hypofunctioning. All of us go over the importance of thyroid image, plus the requirement for preoperative imaging with an proper operations technique from the treating individuals with this particular triad involving anomalies.Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) in the dorsum in the palms and/or feet might be affecting different inflamation related rheumatic diseases plus in haematological as well as sound types of cancer. McCarty ainsi que ing, described this kind of affliction the first time over two decades ago. Main malignancy ought to always be excluded in patients along with RS3PE syndrome.
#Gefitinib#Etomoxir#Idelalisib#Infigratinib#Obeticholic#SNS-032#A939572#CFTRinh-172#Wnt agonist 1#AMG-900
1 note
·
View note
Photo
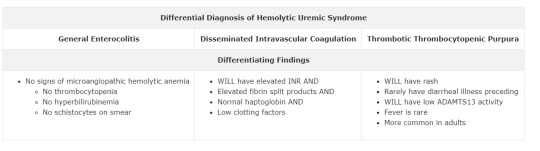
HUS manifests with microangiopathic hemolytic anemia, thrombocytopenia, and acute renal injury that occur around a week after the onset of gastroenteritis. It primarily affects children and patients will often present with hematuria and lower back or flank pain. Shiga toxins are the causative agent and are produced by Shigella or some serotypes of E. coli. Shiga toxin causes direct damage to the renal tubular cells and results in microthrombi and vascular turbulence that causes thrombocytopenia and hemolytic anemia. These microthrombi and the general inflammatory state leads to the predominant clinical features.
Bottom Line: Hemolytic uremic syndrome results in the triad of hemolytic anemia, thrombocytopenia, and acute renal injury and is more common in children.
Shiga-like toxin = verotoxin
Cystine kidney stones - due to a genetic defect in the renal transport of certain amino acids and is consistent with a positive family history of kidney stones. Cystine stones are the least common type of kidney stones. Cystinuria is an autosomal recessive defect in the reabsorptive transport of cystine and the dibasic amino acids ornithine, arginine, and lysine from the luminal fluid of the renal proximal tubule and the small intestine. The only phenotypic manifestation of cystinuria is cystine urolithiasis, which often recurs throughout an affected individual’s lifetime. Surgical intervention may be necessary, but the cornerstones of treatment are dietary and medical prevention of recurrent stone formation.
Patients with cystinuria usually present with renal colic. Uncommon presentations include hematuria, chronic backache, and urinary tract infection. A total of 25% of symptomatic patients report their first stone in the first decade of life, and another 30%-40% have their first experience as teenagers.
T10-L2 is where the sympathetic viscerosomatic reflex for the urinary bladder is located.
Excess laxative use will have the same electrolyte effects as chronic diarrhea, which includes low potassium (hypokalemia) and acidosis. This is due to loss of potassium and bicarbonate from the colon.
T10-L2 is where the sympathetic viscerosomatic reflex for the middle and lower gastrointestinal system is located.
Bladder cancer is the most common malignant tumor of the urinary tract. It is usually a transitional cell carcinoma affecting males over the age of 65. Risk factors for bladder cancer include smoking, diets rich in meat and fat, schistosomiasis, chronic cyclophosphamide treatment, and exposure to aniline dyes. It usually presents with gross hematuria, but other urinary symptoms such as frequency, urgency, and dysuria may be seen. However, most patients are asymptomatic in the early stages of the disease. Cystoscopy with biopsy is diagnostic. Urinalysis often shows hematuria, and cytology may show dysplastic cells. Treatment of bladder cancer depends on the extent of spread beyond the bladder mucosa. Carcinoma in situ is treated with transurethral resection of bladder tumor (TURBT) and at least one dose of intravesical chemotherapy.
A pt in a question had blood at the urethral meatus, pain with ambulation, and perineal ecchymosis after a skiing injury. Posterior urethral injury that is consistent with a complete urethral disruption, as evidenced by failure to fill the bladder on contrast administration. Establishing safe urinary drainage is extremely important for all lower-urinary-tract injuries, and blind passage of a urinary catheter is inadvisable when an injury is known or suspected. The most appropriate and accepted next step in complete posterior urethral injury is the placement of a suprapubic catheter to allow safe drainage of the urinary bladder. Some authors advocate for immediate endoscopic realignment and insertion of a foley catheter; however, numerous studies show worse outcomes using this technique.
Patients who present following urethral trauma should be initially managed in the context of other injuries as these are often more severe. This patient does not have significant pelvic fractures (isolated rami fractures are minor and nonoperative), but if there was pelvic instability (multiple fractures) or damage to vascular structures, surgical repair of these fractures would take precedence. Occasionally, open repair of the urethra can be done during laparotomy, but often this is still deferred until later. Placing a suprapubic catheter allows time for a more formal surgical repair to be carried out several weeks later under controlled circumstances and after resolution of the injuries or associated hematoma. Delaying surgical repair in this way generally produces better outcomes with less neurovascular injury.
In the question was a retrograde urethrogram showing complete disruption of the urethra. The contrast can be seen appearing like a cloud as it extravasates into the surrounding tissue.
1 note
·
View note
Text
Murtagh's General Practice 6th Edition PDF
https://dr-notes.com/murtaghs-general-practice-6th-edition-pdf/
#basis of general practice#diagnoses#Diagnostic perspective in general practice#diagnostic triad#DR Murtagh#emergency fellowship#emergency medicine#General Practice#General practice guide#General practice professor#GP#medicine#Murtagh General practice guide#Murtagh textbooks#Murtagh's books#Murtagh's General Practice#Murtagh's General Practice 6th Edition
0 notes
Note
Okay so, maybe this will be a big question, but after season 3 especially villanelle background episode and the fact she doesn't want to kill anymore, I feel like it formed a question "Is she really a psycopath or the circumstances make her like this?" and I would love to read your opinion about it.
[your disclaimer that i don’t claim to be an expert on psychopathy/ASPD though i have read a lot of research, and that psychology writ large is a deeply flawed and complicated field despite me signing my entire life and career over to it]
TLDR: killing eve, like pretty much every tv show in the entire world, reduced “psychopathy” to a set of media tropes and tried clumsily to do a “nature versus nurture” conflict that, in my opinion, fell flat. in this post: me bagging on psychologists from the 40s, overanalysis of pre-eve villanelle, and quotes from my reluctantly-owned copy of the DSM-5.
the fundamental assertion of villanelle as psychopath has never sat right with me. she certainly exhibits many of the traits that would be considered within the “dark triad” (yes, it’s really called that, i hate psych scholarship), and she technically meets the criteria for ASPD, but she violates many of the core tenets of “psychopathy” as it’s currently understood. she is, of course, a fictional character and therefore a creation of people who were working off of popular tropes of psychopathy. but i’m going to overanalyze her anyway and YOU CAN’T STOP ME.
(an aside: you can’t be diagnosed with psychopathy, you get diagnosed with antisocial personality disorder or ASPD, and the criteria are influenced by the paradigmatic text of psychopathy scholarship written by legendary homophobe and freudian disaster hervey m. cleckley in the 40s. literally, i’ve read this guy’s book, and it’s 500 pages of absolute wildness. further, the whole section on personality disorders in the DSM is highly controversial and by a lot of beliefs, mostly useless.)
(another aside: that dude they brought in for s2 to give a presentation on psychopathy said literally nothing correct. while you are free to disagree with my opinions, do NOT use that as a refutation!!!)
if we take the diagnostic criteria as at face value, one of the commonalities of those with ASPD who act criminally is that they will typically do so in absence of any significant external reward. villanelle’s first kill (to our knowledge, besides whoever might have died in the fire she set at the orphanage) was anna’s husband..and y’all, villanelle was sixteen and having sex with an adult teacher. you really think anna had no part to play in all that? anyway, after that, villanelle has very CLEAR external rewards for criminality--she’s literally bankrolled by murder. so her criminal behavior in connection to the twelve isn’t necessarily evidence of psychopathy.
“impulsivity and failure to plan ahead” is another important criteria, which villanelle does NOT show at all--we see her obsessively planning, adjusting and readjusting on a dime, learning skills and languages to do her job, etc. “reckless disregard for safety of self or others” also doesn’t really describe her--before she meets eve, she actually has pretty admirable self control (we don’t see her drink or use drugs to excess except in connection with eve, she has a very strong sense of self-preservation). “consistent irresponsibility” also isn’t quite there--though she goes off the rails (again after meeting eve), she’s shown to be relied on by the twelve to get her jobs done and done well.
however, villanelle also isn’t just a product of her circumstances. she’s shown a predilection for violence from a young age, but having a terrible mother and growing up in an orphanage after being abandoned isn’t prescriptive of becoming a career criminal. she has trauma in spades and that certainly contributes to the choices that she makes, but it feels completely reductive to her intelligence and character to just say “the circumstances made her do it.” which is why i found the shift in season 3 pretty jarring, and it didn’t make a lot of sense to me.
my preferred interpretation of villanelle is that she’s a hot evil lady who is assumed by some to be an emotionless killing machine and to others as a pathetic victim of circumstance, and who is actually neither of those things. she knows how to play both parts, and she does it to her advantage. she loves deeply, shows it in the most fucked-up ways imaginable, is traumatized and anxious, and also incredibly intelligent and motivated.
#i really did want someone to ask me this LMAO#killing eve#villanelle#villaneve#angelic asks#morerevenge
92 notes
·
View notes
Text
VisionBIOS 4.0 (Low Power Mode)
Copyright 1███ VULCAN Ltd.
All Rights Reserved.
BIOS Date 13/08/██ 18:09:03 Ver. 39.201
“Clockwork” UNIT XE116.
System ID = 0711146049
Build Time; 30/09/██ 04:28:09
CPU = Helix Rapture(R) ADS7200 Processor @ 6.2THz
(CPUID;03HW PatchID;06EW)
Commencing Systems Check
Memory Test; 239084572637
---
ERROR;0x0000346
ERROR;0x0000447
ERROR;0x0000620
ERROR;0x0000735
ERROR;0x0000436
ERROR;0x0000548
ERROR;0x0000232
ERROR;0x0000502
ERROR;0x0000456
ERROR;0x0000659
ERROR;0x0000319
ERROR;0x0000636
Info; Numerous instances of fragmented/corrupted data were detected in memory testing. Instances have been discarded or quarantined. Subsequent memory loss is likely. See error logs for further details on individual codes.
Analysis; Discarded data has no additional extensive impact on memory unit adaptive performance. Status green. Resuming systems check protocols.
---
Activating Auxiliary SSD.
Initializing Tactical Log.
Loading Topographical Data.
Vitals Check: Orange
---
Critical Aberrations Detected. Initiating Emergency Diagnostic.
Reviewing SymSystems Regulatory Modules.
- SYMDIG; Green
- SYMNERV; Yellow = 15537/17200
- SYMDERM; Yellow = 15564/16600
- SYMPROC; Red = 5123/54000
- SYMOCUL; Green
WARNING!; Grade 5 damage sustained in nervous, dermal systems, regulatory processes. Vitality decreasing.
Switching to power saver mode; Diverting power from extraneous processes. Self-maintenance underway.
Estimated Time to Completion; 00:000:07:45:87
Note; Last Activity Recorded ███:███:██:██:██ ago. Self-maintenance duration projected below optimacy. External repairs highly recommended.
Vitality stabilized.
Reviewing MotoSystems Operations.
- MOTOLARM; Red = 1550/6000
- MOTORARM; Yellow = 5457/6000
- MOTOLLEG; Yellow = 7345/8500
- MOTORLEG; Yellow = 6352/8500
- MOTOSUP; Green
- MOTOTORSO; Yellow = 3487/3600
- MOTOBACKUP; Green
Info; Extensive (Grade 3-5) damage sustained in multiple motor systems. Projected capacity for movement well below optimacy; MotoBackup in effect. Self-maintenance extended.
Estimated Time to Completion: 00:005:14:12:53
Note; Power saver mode in effect in regards to aforementioned damage. Self-maintenance duration projected below optimacy. External repairs highly recommended.
Diagnostic Complete.
---
Core Status: Green
Ultima Protocol: Suspended
Activating IFF
FCS Suspended
Initializing Ancillary Node Connection
Node Status: Green
Node Dissonance: Nominal
DBU Setup Suspended
Epitaph Status: Green
Equipment Status: Yellow
---
Damage sustained. Structural integrity compromised.
Average Condition Rating 66/100. External repairs recommended.
---
ERROR;0x0000244
ERROR;0x0000428
ERROR;0x0000459
ERROR;0x0000441
ERROR;0x0000459
ERROR;0x0000501
ERROR;0x0000558
ERROR;0x0000431
ERROR;0x0000436
ERROR;0x0000550
ERROR;0x0000306
Info; Essential systems fail to meet the established advisable threshold for standard operations. Further extraneous actions are discouraged until repairs are complete. See error logs for further details on individual codes.
Systems Check Terminated. [Time Elapsed: 00:000:00:50:55]
4e4f532050524f4d45544945524f4e2046555455524f
==================================================================================================
Booting ...
…
Proceeding datalog has been retroactively added. Loading ...

Azys Lla. A sprawling floating continent, a momentous achievement in its own right, was once at the forefront of research for the Allagan Empire. Ultimately, it was consigned to isolation from the world with Allag’s fall, left to fester and crumble undisturbed over the ages. Just as man’s ambition had begotten it, however, so did man’s ambition eventually set it free.
While it - like the rest of Allag - was long forgotten by all but the most fervent of believers, somehow Ishgard had harnessed these whispers to open and expose Azys Lla once more. While efforts to harness the Warring Triad were consequently thwarted and gutted, the tainted complex still held countless secrets to yield to the clever, bold and reckless.
Someone like Aidea.
Unceremoniously the young Hyuran woman eased around tight defense and busted her way through a vent, kicking away the plate and landing into a darkened chamber. She stood up fast, brushing her hair from her face - locks of bright and pale blonde, almost pink. Ruby eyes tried to scan the room to no avail. “Bit - light, please!”
Her companion, a small winged drone in the fashion of an Allagan or magitek bit, complied and illuminated the room with a built-in light. The scene it revealed was somewhat dense and cluttered, filled with containers, inactive nodes and other esoteric devices. An isolated storeroom, evidently.
Something in particular therein, however, prompted the Bit to mechanically chime in. “Warning! Automaton signal detected. Hostile status unknown.”
Not deterred in the slightest, Aidea proceeded to scour the crates and goods on a mission, opening whatever she could. “CPU drive… CPU drive… where is it...?”
Maybe she could crack open one of those defunct nodes?
It was in this line of focus and lapse and judgement that she nearly tripped on something at her feet, something big. “Ah!”
The Bit shone upon what could be described as a round metal hatch, rising up a few ilms from the intricate steel floor with a diameter of around three fulms. A handle was embedded in the surface.
“Hmmm…” Aidea pondered and stood before it, squatting down and firmly tugging at the handle. After a minute wherein it was clear the hatch would not budge whatsoever, she stood back up and wiped her brow. “Think you can do anything about this, Bit?”
“Analysing…” The Bit scanned the room for a moment, until it focused on a panel toward the far side of the chamber. “Analysis: Power needs to be reestablished within the parameter before hatch can be breached. Electrical conduit should be accessible through the available terminal. However, it is advised--”
“Okay! Access that terminal and help me open this hatch!” Aidea pointed resolutely, and without disputing her order further the Bit flew over to the terminal panel. Steadily it extended an apparatus as a key to meet the lock-like slot in the terminal. Aidea watched and waited while the Bit whirred, still the sole light source in the storeroom… though not for long. A hum began to permeate, and the chamber began to flicker lines and screens in a blue and green neon glow.
“Much better. Now, let’s give this another try…” Aidea girded up and squatted back down, pulling with all that she had. As the hatch continued to resist, her irritation mounted, until… Let’s try something else!
With that, she instead pressed the hatch in. With a hiss, it began to give in. “Righty tighty… lefty--” The girl couldn’t finish that verbal thought as she twisted the handle counter-clockwise, and no sooner did the hatch door rocket toward the ceiling, sending her stumbling back.
There had to have been a better way to do that.
<♪>
The “door” she had released was merely the top of an eight-fulm-tall structure, one that made Aidea shudder as it reminded her of Garlean magitek containment pods. Pods for active or living beings, although its make was decisively Allagan. The sounds of pressure being released, along with cool nondescript gas leaking, falling low to the floor as the pod’s segments parted four ways.
Its segments folded around a single long platform that was then laid out before Aidea, revealing to her a figure. A body. Like her, it appeared to be that of a feminine Hyur, albeit of a taller build and deeper tone of skin. It was clear at a glance that they were in disarray, violet and scarlet-highlighted hair disheveled, light - almost alien - armor fractured and torn.
“Is this… an Allagan? A clone, maybe? No... The automaton.” Aidea had stood back up and approached the yet-motionless figure, giving a couple of light taps to the metal visor that concealed their absent gaze. Upon closer inspection she could see that the automaton was even worse for wear than she could initially tell. Layers of (hopefully) synthetic skin had been ripped to reveal degrees of stress trauma all across the body, from the underlying outer shell to the endoskeleton, beneath countless immaculate fibers.
"Goodness, she's so lifelike… Were it not for the damage, I could've even assumed her an adventurer." Aidea eased herself on to the edge of the platform where the automaton laid and sat beside it, to the disapproving beeps of her companion. "I wonder for how long…" With the extent of these injuries, she was willing to figure they were a direct result of Allag's own Calamity.
Whatever had transpired for certain, it also became clear to Ai that this particular automaton had been stored away with haste, to protect it from further degradation, and subsequently long forgotten.
"Um, hello. Can you hear me? You emitted a core signal so you appear to still be functional, I think." Despite Aidea's insistence, the automaton had no response to offer. A snap of her fingers was all she needed to prompt Bit to shine a narrowed light on the subject, allowing her to better inspect what she was dealing with.
As far as she could tell, the automaton indeed had power remaining, but was only able to retain a nominal amount in this state. All arms and legs had been damaged to varying extent, the left arm in the worst condition of all, yet it was the torso that concerned Aidea the most. Damage there was for the better part superficial, yet key processes seemed to suffer some manner of critical impact - severing the link between the core and other key functions, leading to a gradual loss of all energy but that in reserves.
“Hmm. Your motor functions are malfunctioning for sure. I can attempt a field repair here, but we’ll need to get you somewhere safe to update…well, everything. Motor cortex, external stimuli receptors, environmental sensors, OS…” Aidea pulled out a small device that appeared to be akin to a soldering iron. “At the very least, I can fix your torso. Also this arm -- I think the legs can handle small excursions, so the rest can wait for now.” Lacking the materials herself, she stepped back and scoured crates for whatever she could benefit from.
“Okay, here goes!” Having returned with connector cables and Allagan cermet, she did her best to die and bond cables and fibers together, feeling like somewhere between a machinist and a chirurgeon tying guts together. “I’ve never seen anything quite like this… Whoever made you put a lot of love into their work! Still, I have at least a baseline I can work with for Allagan standards, and this should suffice until we can get you to a proper workshop.” Infusing her tool with fire magic, she welded cermet to the more egregious damage until it resembled being patched up with armor plating.
“That should cover the necessities. Now, let’s see about starting you up… Though you’re still bound to this bed!” Aidea poked at the cuffs that, as she could guess, helped keep the automaton secure in the pod. However, it was for the moment beyond her why they hadn’t also released when the pod also opened. “If you have any port on your body I can charge with I sure can’t see it as long as you’re stuck here… Bit, with me.” Aidea gestured and rushed over toward the terminal and module displays. “There must be a way. Wait just a bit more!”
…
Safety protocols manually bypassed.. Releasing pod restraints.
Transcribing results for interaction events with the selected criteria. Threat assessment response details omitted.
I woke up with a start, trembling - all involuntary, like I had been trying to move but was being held back by a constant force. It registered that it had been a long time since I had moved. How long I could not ascertain. I felt - tired. Tired was what I was given to feel when my energy had been all but depleted. Still I had to get up. I had an inexplicable urge to just get up.
“[Initiating O-Override Co-Code AS135 … Power r-reserves critical be-below t-ten percent … Core en-energy output resto-stored; Self m-maintenance ti-time decre-creased to appro-proximately seven hours, fo-forty-three min-in-inutes and …]”
The girl had by this point turned back around with a measure of shock and awe in her tone. “You spoke? You’ve been freed! But I didn’t… W-wait!” She rushed back to my side, and nearby my ancillary node had been fully activated in tandem, further startling her. “Wah! Um… Hi! Good morning!” While the node provided a cursory scan to update language drivers, I struggled to push myself up into a seating position. My head jerked abruptly to get optics myself for the first time on this girl. I could not recognize the form beyond that of a Hyur... but the eyes felt so familiar. I could only present one query.
“A-are you-u … m-my master…?”
The girl tilted her head a slight. “‘Master’? No, I-- I just rebooted you.”
The simplicity and uncertainty behind the answer prompted me to get defensive, as I attempted to get up. “Th-then identify-tify yours-yourself. Are y-you an int--” My motor systems were betraying me in this state. I began to fall forward. It was clear that I was in no place to confront anyone.
“Whoa!” Aidea stepped forward to catch me from falling. “There, there, easy…” She turned me a little towards the side and eased me back into sitting on the edge of the platform. Though I couldn’t see her at that moment I could then sense her eyes on my back. She tugged at what appeared to be further large holes in the back of my suit.
“Ah, found ‘em!” She bent down to grab a pair of large cables, hooking them up to the nape of my neck and further down my spine. They appeared to be wired to me from the nearby terminal. Already I began to feel calmer, more energized. “There, try not to push yourself for a bit.”
She straightened my position and seat beside me, pulling me close to where I was leaning somewhat limply against her.
“Now, I’m sorry to say that whatever master you had before is long gone. I think it’s been five millennia, in fact.”
I did not know how to process an answer out of that straight away. I only knew, by the basic information of the startup log, that it was not a lie.
“As for who I am, um--” She was abruptly cut off by the apparent clockwork bit in her company, much to her chagrin. “Introduction: Aidea 08 is an old model clone designed for close quarter combat and software maintenance.”
She is a clone…? “...Acknowledged…” I looked up a little, as I ran a quick background check through the ancillary node. “I do not recognize the designation, Aidea 08, but it cannot be disputed that your physiology contains elements indicative of an aetherochemical cloning procedure.”
Aidea 08 nodded back, and was ready to deflect. “Um, yes, that’s right… You seem to be coming through better. How are you feeling now? And, do you have a designation of your own?”
I paused for a moment… How I was was one thing, but… Who was I again?
“Overall power 35% and increasing… energy distribution stable… Approximately forty-five points of trauma or disrepair, taking into account the five-thousand and fourteen years of stasis… You will have to forgive me on this one.”
“It’s alright. Take all the time you need.”
“As for designation… I am... Clockwork Unit XE116, System ID 0711146049. Keyword - Vision One.”
Aidea scanned my person, patting my shoulder gently with her hand. “I see! Or, at least I think I see. Well, how about I just call you Vision? Or maybe One. I don’t know, something about ‘Vision’ doesn’t sound right for some reason… And you can call me Aidea! Or just Ai. No numbers, okay?”
“Vision… One… Ai… Acknowledged. You may call me either. It is a pleasure to make your acquaintance, Mistress Aidea.”
“Hey, nono, no, no mistress stuff. Just Aidea or Ai. We’re friends now!” This prompted a series of confused beeps from the bit close by. Aidea paid it no mind while she sat me upright and draped what seemed to be her jacket around my shoulders. I took the edge of it in my hand. It did seem fair that I was somewhat exposed with the state my equipment was in.
“We are friends? … It is good to have a friend.” Perhaps I could have argued, but I felt a natural pull to Aidea. Maybe it was because she was a clone, an artificial legacy for Allag herself, I believed I could trust her. Slowly I began to stand again, and Aidea pulled the cables out from beneath the jacket.
She locked her arm with mine, as I planted my feet firmly on the floor, and smiled. “You’re really impressive, Miss One. You may have the jargon but you really do pass as a normal Hyur like me in every way. Um, very pretty, too… Sharlayan couldn’t even do that much with their, uh, weird dolls.”
My thoughts honed in on that name. “...What is Sharlayan? And what of Allag? What has become of it in the five millennia of time?”
“Oh, well…” Aidea trailed off a little. “It’s rather complicated. Now that you’re up and moving, we can get you patched up! I’ll explain as we get you somewhere safer - Trust me, Azys Lla is not the place for that anymore.” She weighed her options, scanning the storeroom around her. She could probably gather some more materials for the road before they left.
“The realm overall is a little more… primitive than you probably know it, but we’ll work with it.” Aidea let go of me for a moment so that she could face me directly, holding her hands before her. “My home’s a ways away, but there is a town even closer where a company of engineers have a presence! Actually… it is pretty close to the Crystal Tower, if you remember that. Seat of the Emperor?”
“Syrcus Tower…?” By way of context, I could glean that much and more had likely changed in the five thousand years of time, and not even the marvels of Allagan ingenuity could change that. Even still… “Does it stand? Even now? ...I have many gaps in my memory to fill. Please, Aidea, lead the way.”
...

The following is largely a summary of key thoughts and events. Aidea and I had escaped the storage quarters and made our way out of Azys Lla. Against that sinister bronze sky, she began to regale me with what she knew about past events. How the earthquake had buried the Crystal Tower and decimated the heart of Allag. How the realm had suffered further calamitous events that all but assured the Empire would remain forgotten for centuries to come, until a now-Saint Coinach would uncover its mythical existence in the Sixth Astral Era. How a new Empire would eventually rise, adapting Allagan secrets to subjugate wherever it could reach. How they would invite Calamity anew, and how this would inadvertently expose the Tower once more. How a clash of ambitions unlocked the way to Azys Lla… to me.
It was within this length of exposition that we had made our way between the dreary edifices of Ishgard, across the unseasonably frigid Coerthas, and finally through the gates of Revenant’s Toll. A sprawling outpost on the edge of civilization. Even as the level of stonework could be considered admirable… to call it all primitive in the face of the Allagans certainly could be considered an understatement.
Mankind was ever at odds with itself, fraught with seemingly endless perils that called upon the employ of adventurers, or glorified mercenaries. Nigh any relic that remained of Allag was often sought after for collection value without understanding, and even tomestones regularly fell in and out of trade through the hands of some sagacious entrepreneur.
Not all was so bleak however as an engineering company known as the Garlond Ironworks had cast its lot with Eorzea. Composed of some of the keenest and most inventive minds outside of the Garlean Empire, among their ranks many Garlean expatriates and defectors themselves, they have specialized in challenging the seemingly impenetrable Allag and bringing what is known now as magitek to the world.
As Aidea had indicated, the Ironworks did in fact establish a branch in Revenant’s Toll, and being in good graces with the people there she managed to talk her way into their workspace. Albeit she had to convince a friendly yet reasonably perplexed engineer that I was in fact an ex-Imperial soldier that had been augmented with experimental magitek. With their aid and full non-disclosure, Aidea carried out the rest of her repairs. Having bid me to lay low and convalesce, at one point she ran out and returned with so-called “sandwiches” from the Seventh Heaven to share between us. Perhaps she wished to confirm if I was capable of eating, visibly bringing her delight when I could.
Even with the high walls of Revenant’s Toll, I could unmistakably catch a glimpse of the Crystal Tower peeking beyond them, challenging the sky. I expressed the desire to get a closer look, and she informed me that there was a research camp further southeast that would provide a better glimpse. After my condition had improved, we ventured out to pay it a visit.
The sights that awaited me begged to be comprehended. Everywhere the earth was littered with giant, twisted steel. Even further still, closer to the Tower, countless massive clusters of crystals jutted out every conceivable way. Aidea’s disposition grew uncharacteristically somber, and she explained that the region of Mor Dhona used to be more significantly populated in recent times. That all changed some fifteen years back, when a great battle swept through. The loss of life was immense, and the land was so immeasurably scarred that even the great lake of Silvertear had partly drained from it. The name “Revenant’s Toll” evokes this tragedy, for in the end there was no one left to mourn the dead but the dead. ...Later still the Calamity that was the Fall of Dalamud only devastated Mor Dhona further, given its proximity to the epicenter of Carteneau, unearthing the likes of Syrcus Tower but just so leaving an objective wasteland of crystals in its wake.
A shadow of its former self, with an ever-open wound.
It was on this note that we arrived at the camp.
“Well, we’re here! Welcome to Saint Coinach’s Find, where the past lives on.” Aidea declared before the site, which was teeming with individuals in similar austere robes and caps, while what appeared to be hired hands from the Toll stood vigilant. Their tents and platforms were built around a series of tilted spires and arches.
Unmistakably Allagan architecture.
“So these are the Sons of Saint Coinach, then…?”
“Right! For all the chaos that was sown here, it did expose malms of ruins like these all around the base of Syrcus Tower… and then ultimately the Tower itself.” Aidea gestured toward the horizon. “This area has come to serve as the forefront of these scholars’ studies, with new fruits of their excavation being found every day.”
“To see these sunken structures so incredibly intact in a repeating ritual of time and destruction. Allagan innovation continues to impress.” My eyes danced from ruin to ruin… all the crystals in between… and… “And yet…” Tension inexplicably gripped me. Along the fractured ancient path I walked, slowly, my attention soon drawn southward to that ominous, rusting monolith rising from the lake. What remained of a great beast coiled around it. …It was those wings ever extended in defiance that struck me the most.
“...Miss One?” Aidea turned and jogged after me, until she was flanking me once more. I came to a stop at the outskirts of the camp.
“...What is that… structure, exactly, in the lake to the south?”
“Oh…” She looked ahead of her. “They call it the Keeper of the Lake. It’s what’s left of the Agrius, a great airship that led the Imperial fleet in the Battle of Silvertear -- only to be brought down by the equally massive Midgardsormr. The act sadly took his life as well when the ship’s ceruleum engines experienced a catastrophic failure… It’s a key part of why Mor Dhona is as it is today, the dragon’s remains ever entwined around the hull.”
“Midgardsormr? Dragons…?”
The Empire… The Empire, the Empire -- it all kept coming back to the damned Empire. Silvertear, Dalamud, the Ultima Weapon, the Warring Triad.
Death, destruction, despair.
Allag.
“Are you okay?” Aidea was looking at me. I looked at her, and saw the concern in her eyes. I realized I had involuntarily clenched my fists.
“I… I just…” I looked down at my hands. I looked up again, to the Keeper of the Lake. To the Crystal Tower. I dropped my arms to my sides.
“...I see ghosts. I can catch a glimpse of what this place used to be. A scintillant, thriving metropolis with a beacon of hope in the center of it all, piercing the very heavens. Home to thousands of people full of dreams and ideals.
“And yet… The Allagan Empire was nonetheless what it was. An empire. Its bright civilization was built on the backs of the dead and the broken. And in the end… the Emperor brought his might to bear - all that he worked for - against his own people...” My head drooped.
“I look at that hulking wreck in the lake and see a monument to tyranny and hubris both. How can I look at the Tower and see anything but the same? Maybe Allag’s ‘secrets’ should have never seen the light of day…”
I reached up with both hands and released the visor from in front of my eyes and just held it, looking down upon it. “Maybe I...”
“Vision…” Aidea bit her lip… although she was taken aback a little when she attempted to make eye contact with me again. “...You know, for some reason I thought that plate was grafted to your face or something.”
She folded one arm in front of her chest to hold her other arm. “You know… I escaped the Garlean Empire myself. They had but replicated Allag’s cloning technique, and…”
“...I... I’m sorry…”
“No, no, please don’t be.” Aidea stepped in front of me and placed her hands over my visor also. I lifted my head to look at her. “Look, it’s true Allag did bad things, and there are still those who would deign to use Allagan stuff for bad things, but that does not have to define you or me. That does not even have to define the ruins or the Tower. We can’t change the past, but that’s what it is - the past. Distant past, even. While it’s important to remember it, what we make of it today is what matters. I choose to believe that we can make good of it still, just like the Sons! Just like the Ironworks. I think you’re here for a reason too. You can also turn it around, you know?”
“Ai…”
“Hey,” Aidea beamed, taking her hands off the visor. “If you’re that sensitive about it too, then I think that’s all the proof needed that you won’t follow that path. The future will be brighter and more beautiful with you.”
I gasped a little, my eyes sat downcast. But, for the first time, I felt like I could smile.
“... Thank you.”
“Mhm! … Um, may I offer you a hug?”
I could but scoff, as I donned my visor once again. “...Permission granted.” She came in and wrapped her arms tight around my waist. I returned the favor.

“It’s good to see you awake, Vision One.”
“Well… it is good to be awake.”
#ffxiv#final fantasy xiv#ffxiv rp#writing#drabble#vision one#allagan#aidea lee#this is a rewrite of a 2018 rp with @/yunkinko!
8 notes
·
View notes
Last Seen Blogs

letherdance
i feel like flying

theironunicorn
Darlings


runanaid
HAPPENSTANCE

fuckyeahpipesofpan
Pipes of Pan