#covid-19 infection cases in US
Text



"If a pig catches both a human influenza A virus and an avian influenza A virus at the same time, it can spark a process known as viral reassortment — a genetic exchange in which flu viruses swap gene segments."
"Those swaps can introduce dramatic changes, producing a new virus with certain properties of a non-human strain coupled with the capacity to infect and spread between people."
"The death rate in humans may be upwards of 50 per cent, World Health Organization data suggests, though it's possible that milder infections are getting missed, skewing the case fatality ratio. Still, in a population that's never been exposed, the global impacts could be dire."
"More human cases could also be happening under the radar among farm workers who've moved to the U.S. from abroad, don't speak English as their first language, and may be hesitant to seek medical help, he added."
"So I think there's probably underreporting on both sides," Armstrong said."
"If [H5N1] gets into a population where there's constantly animals going in and out … it might not ever leave."
I've been watching this develop for the past several days, and apart from being terrified most people will not take this seriously (I've seen a handful of people already shout conspiracy on social media and it's alarming to see, as always). What I wanted to point out is that pandemics are going to continue to be our 'normal.' I watched a great video on YouTube a while ago (I believe it was by Vice?) that touched base on how this is going to become our new reality because of multiple factors (such as our proximity to animals, and environments/etc). It was when Covid hit and they did a piece debunking some of the misinformation floating on the internet. If I can find it I will post it here because it was informative and relevant to pretty much any world crisis we will see around any virus that spreads among a human population.
This post isn't trying to fear monger anyone, I just hope more people are aware of what is happening because this is important to talk about. There are already cases (of cows getting this bird flu) in the US, and I won't be surprised if there will be instances in more countries around the world. As usual, keep washing your hands/keeping good hygiene practices, masking up (and if you aren't I hope you consider it), and taking precautions if you do happen to visit/work or go near a pig or poultry farm too:
I'll keep track of this here of course, but please stay informed folks. And also FU to any governments who will try to minimize this or try to diminish the severity until it's too late and community spread happens like Covid because their actions are influenced by capitalistic interests.
Update (April 7th, 2024, 9:32pm EST): to anyone wondering where some of the source information originates from -here is a link to the CDC. They are tracking documented avian virus outbreaks in the US and the public can access it here:
#current news#current events#global news#united states#cattle#cows#cattle farming#avian flu#bird flu#h5n1#mask up#pandemic#covid#covid isn't over#covid conscious#covid is airborne#covid is not over#viruses#fuck capitalism#anti captialism#healthcare#public health#world health organization#cdc#news update#update
15K notes
·
View notes
Text
What I Want You To Know About Long COVID
Well lads, I've been suffering from Long COVID for over a year now. My life is at a complete standstill. I'm 25 years old and I'm too sick to go back to school, I can't work, I had to move back in with my parents and I'm still stuck here.
Here are just a few things I wish people knew about Long COVID, including things I didn't know myself until I got it.
COVID destroys your immune system. Yes, even if you don't have Long COVID. Are you getting sick more often now? When you get sick, does it last longer? There are many studies showing that COVID causes t cell depletion, even in mild COVID cases! T cells are how your body remembers how to fight off infections you've had before so losing those cells? Bad news.
Your initial infection can be mild and you can still get Long COVID. Right from Yale Medicine, "Most people with Long COVID had mild acute COVID." (This is also a good link for a basic Long COVID overview).
There can be a gap of time between when you "get better" from the initial COVID infection to the onset of Long COVID symptoms. Some people get sick with an initial COVID infection and never get better. Some get better and then weeks or months later start developing Long COVID symptoms. Long COVID symptoms can even fluctuate over time, can go away for months and then suddenly come back.
So many people have Long COVID and don't realize it. Do you feel more tired lately but no matter how much you sleep, nothing helps? Is it harder to concentrate at work or school? Can you just not think like you used to? You could have Long COVID and not even know it. Even mild post-COVID symptoms are still Long COVID.
COVID can do anything to your body. Long COVID has over 200 recognized symptoms and can affect basically any part or system of your body. There is no one mechanism or cause of Long COVID which unfortunately also means there's no one cure either.
The effects of COVID are cumulative. Each COVID reinfection increases your chances of developing Long COVID. COVID is also affecting your body in other ways, yes, even if you're otherwise young and healthy! "Repeat COVID-19 infections increase risk of organ failure, death".
Once you have Long COVID, repeat COVID infections will make your symptoms worse. "80% [of Long COVID patients] saw their symptoms worsen [from reinfection]. In 60% of people who were in recovery or remission from Long COVID, reinfection caused a recurrence of Long COVID."
There is a lot more I want to say about Long COVID but I want to keep this post at least somewhat manageable to read. Like how when COVID is contracted during pregnancy, those COVID-exposed fetuses have a 6.3-fold increased risk of motor developmental delays, or that another study found 50% of babies exposed to COVID in utero had developmental delays.
You need to keep caring about COVID, for others around you and also for yourself even if you're "healthy". Everyone is at risk. And don't forget 40-60% of COVID infections are asymptomatic, which is why masking even if you feel fine is crucial. The only way right now to not get Long COVID is to not get COVID in the first place. It's not too late, if you've stopped masking it's never too late to start again! I know it's easy to get distracted by things in your life that seem more real than the possibility of getting sick some time in the future, and the peer pressure to not mask can be intense. But it only feels less real or less important until your entire life is having Long COVID. Trust me.
I know this is a complicated issue, many people can't afford to stay home when sick even if they want to because of their jobs, there are disgusting policies trying to ban wearing masks, but please if you can. Keep masking. Masking works, masking saves lives.
This post got a bit longer than I wanted so below the cut is a non-exhaustive list of my Long COVID symptoms and some of my experiences as one of the "healthy young people" who got "unlucky". cw brief mention of suicidal ideation.
Welcome to the Thunderdome that is my body with Long COVID. Keep in mind these are just my experiences and symptoms, Long COVID can cause any range of symptoms at varying severities.
Dysautonomia: Exercise intolerance, Post-Exertional Malaise (PEM), fatigue, and heat intolerance. What do those things mean? Here's some specific examples. Absolutely terrible circulation I am so cold all the time but also, if I get a little too warm I will pass out. Eating hot food makes my heart rate spike, I sweat, my body feels heavy. Blood pooling and pins and needles in my feet when I walk. Don't even think about exercising past walking, it's impossible. I used to work out an hour a day 4 times a week and now walking up one flight of stairs makes my heart pound and I can't breathe. Can't take even just warm showers anymore or I will pass out. Heat rashes from being in the sun for 10 minutes.
Digestive issues: Honestly too many to name but: constant bloating, extreme nausea, constipation, slow motility, lack of appetite, just so much cramping and pain. I lost 18 pounds from Long COVID, as someone who was already considered underweight their entire life, and almost had to get a shunt put into my chest to deliver nutrients because I was nearly completely unable to eat. For the first 6 months of Long COVID, if I could manage 600 calories a day, that was a good day.
Histamine intolerance: Oh boy. My worst symptoms, I don't even know where to start with it. If you know Mast Cell Activation Syndrome (MCAS) it's very similar. I can only eat 19 foods. If i eat a single bite of something not on that list, it's 48 hours of absolute hell. Coughing, migraines, itchy eyes, such extreme nausea I cannot even describe it, panic/feeling of doom, racing heart rate, derealization, rash, uncontrollable muscle tremors. I only learned about histamine intolerance 5 months into having Long COVID so before that, I was experiencing these symptoms nearly every single day. Terrifying isn't even a strong enough word to describe how it felt to experience all this and have no idea what it was, how to stop it, or if it would ever stop. Really dark times.
Neurological issues: More of that derealization. Inability to concentrate. Anxiety. OCD-like symptoms such as thoughts getting "stuck" in my head, repeating 24/7 completely unable to stop them, genuinely felt like my brain had cracked open and I had lost my mind. Constant dizziness like I'm on a boat.
Sleep issues: I sleep like garbage. I have insomnia, I wake up dozens of times every night and every single time I sleep I have intensely vivid dreams. I can't sleep longer than 7 hours total no matter how exhausted I am. It is exhausting. I'm exhausted, I'm so so tired.
And finally. Just. Really intense suicidal ideation. My body, my health, my entire life has been stolen from me because someone else decided my life was worth less to them than wearing a mask or staying home if they feel sick. Before I got Long COVID, I was preparing to go to South Korea to teach English, then on to a PhD in neurolinguistics, I was supposed to meet my long distance partner and had already booked plane tickets when I got sick. All of that has been destroyed.
Most of us with Long COVID are stuck in a cycle of being extremely sick, then if you're lucky you'll slowly get better over months, just to get reinfected and go right back where you started or worse. Honestly, I'm not scared of dying from COVID. I'm scared of living for a long time, suffering from Long COVID the entire time. This isn't living.
I don't know how to end this now. I'm still fighting, I'm trying experimental treatments, I'm not giving up yet. I hope everyone reading this stays healthy and well.
7K notes
·
View notes
Text
In 2020, Robert Kuciemba, a woodworker in San Francisco was infected with covid by a co-worker after his Nevada-based Victory Woodworks transferred a number of sick workers to the San Francisco site for a few months.
Through the proceedings of the case it turns out that the employer knew some employees might be sick but they transferred them anyway and ignored a San Francisco ordinance in place at the time to quarantine suspected covid cases.
Kuciemba was subsequently infected and he then infected his wife, who ended up in ICU on a ventilator.
The California Supreme Court just ruled against Kuciemba on the basis that a victory, while, in the court's words, "morally" the right thing to do, would create "dire financial consequences for employers" and cause a "dramatic expansion of liability" to stop the spread of covid.
There’s a few stunning details to note in this case. First, the court agreed that there is no doubt the company had ignored the San Francisco health ordinance. In other words, they accepted the company had broken the law. And then concluded “yeah, but, capitalism.”
Secondly, the case was so obviously important to the struggle between capitalism and mass infection that the US Chamber of Commerce, the largest business lobbying organisation got involved and helped the company with its defence. Remember, this is a tiny company in a niche industry. The involvement of the biggest business lobbyists in the country tells us a lot about the importance of the principle they knew was at stake.
Thirdly, the defence of the company is very telling. They said “There is simply no limit to how wide the net will be cast: the wife who claims her husband caught COVID-19 from the supermarket checker, the husband who claims his wife caught it while visiting an elder care home."
Well, exactly. Capitalism couldn’t survive if employers were liable for covid infections contracted in the workplace, and the ripple effect of those infections. And they know it.
This case is something of a covid smoking gun, revealing what we always suspected but had never seen confirmed in so many words: the public health imperative of controlling a pandemic virus by making employers liable for some of that control is, and always must be, secondary to capitalist profit.
This ruling is also saying out loud what has been obvious to anyone paying attention for the last two years: employers don’t have a responsibility to keep your family safe from covid. You have that responsibility. And if you give a family member covid that you caught at work and they get sick or die – even if it was a result of law-breaking by your employer – that’s on you buddy.
It is the same old capitalist story: the shunting of responsibility for ills that should be shared across society, including employers in that society, onto individuals.
This ruling essentially helps codify workplace mass infection and justifies it as necessary for the smooth functioning of capitalism.
This is not new. This is where the ‘just a cold’ and the ‘mild' narrative came from. It came from doctors and healthcare experts whose first loyalty was to capitalism. Not to public health. To money, not to lives. Abetted by media who uncritically platformed them.
While this ruling tells us little that we couldn’t already see from the public policy approach of the last two years, it is revealing (and to some extent validating) to see it confirmed by the highest law of the land in the United States.
8K notes
·
View notes
Text
It's still not just a cold.
"This study showing that severe acute respiratory syndrome coronavirus directly infects coronary artery plaques, producing inflammatory substances, really joins the dots and helps our understanding on why we're seeing so much heart disease in COVID patients," Peter Hotez, MD, professor of molecular virology and microbiology at Baylor College of Medicine in Houston, told Medscape.
Oh, also?
CDC predicts respiratory disease season will be similar to last year
"The CDC said it expects a similar number of respiratory disease cases this year as last year, with 15 to 25 new weekly hospitalizations per 100,000 people."
"As of Friday, nearly 12 million people have gotten the new Covid-19 vaccine since they were authorized last month, according to HHS. That’s millions more than the week prior, but still less than 4% of the US population."
No one is protecting themselves. And no one else will protect you.
Even if you're not worried for yourself....don't be one of the people that carries it to someone else. We're all responsible for the most vulnerable people in our society. (That could be you, by the way.....)
WEAR. YOUR. MASK.
2K notes
·
View notes
Text

#It's not as a treatment...#When Trump asked if we could use high temperature and high lights to kill the virus#Deborah#who was also in the room#responded:#Deborah's face as Trump talked about his treatment advice#Recalling the day#Deborah said she wanted to disappear.#Birx froze#hands clenched on her lap. “I looked down at my feet and wished for two things: something to kick and for the floor to open up and swallow#Since the pandemic began#the number of people infected with COVID-19 in the United States has repeatedly exceeded worst-case predictions.#On May 21#Popular Science reported that the death toll of COVID-19 in the United States in a single day is now around 300#which is three times the daily death toll from car accidents in the United States.
1 note
·
View note
Text
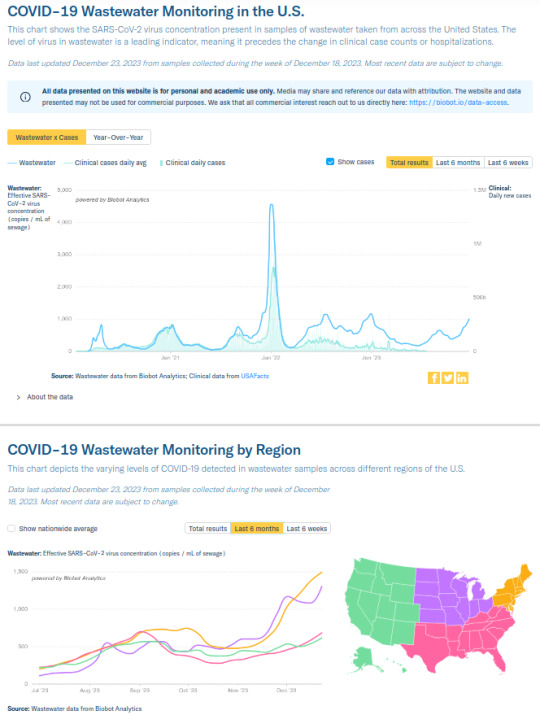
Though the Centers for Disease Control and Prevention has stopped counting Covid-19 cases, according to wastewater data—which emerged early on as an accurate tracker of the ebbs and flows of the virus—we are currently in one of the biggest surges of the pandemic, amid the spread of a new variant, JN-1, as the virus keeps mutating. More than three-quarters of U.S. hospital beds are currently in use due to Covid hospitalizations. Uptake of the most recent booster shot, which should help to protect against the new variant and lower the risk of severe cases and the odds of getting long Covid, hovers around 19 percent.
Meanwhile, the most recent White House response to a question about whether they had any guidance for hospitals, some of which have brought back mitigation protocols in response to the most recent Covid spike, came courtesy of press secretary Karine Jean-Pierre: “Hospitals, communities, states, they have to make their own decisions. That’s not something we get involved in,” she replied, appearing exasperated.
“We are in possibly the second-biggest surge of the pandemic if you look at wastewater levels,” said Dr. Monica Verduzco-Gutierrez, who runs a long-Covid clinic at the University of Texas, San Antonio, and has had ongoing Covid symptoms since August 2022. “There is no urgency to this. No news. No discussion in Congress. There is no education.”
[...]
Since the Biden administration declared the end of the national emergency in May, Americans across the political spectrum have largely followed the example set by the government and entirely disposed of any level of Covid precautions. Liberal and left-wing outlets have participated in the normalizing of Covid too, dismissing or even ostracizing people who still take precautions as if they are tin-hat conspiracy theorists. “We can’t be in lockdown forever,” has become a common refrain, as if wearing a mask on the subway constitutes “lockdown.”
In September, Biden himself participated in the spread of this kind of harmful disinformation when he declared the pandemic “over” on 60 Minutes. “If you notice, no one’s wearing masks,” he said. “Everybody seems to be in pretty good shape.” This is, essentially, governing via “vibes”—so much for “following the science.”
[...]
The consequences of discarding all Covid precautions are becoming clearer, as more people get repeated infections and long-term symptoms, amid an alarming spike in heart problems among healthy young people. People are getting sick more often not due to the myth of “immunity debt,” which posits that the lack of exposure to other people during lockdown has made people less able to fight off infections (three years later), but because Covid weakens the immune system. Each time someone contracts Covid, the odds of long-term complications increase.
520 notes
·
View notes
Text
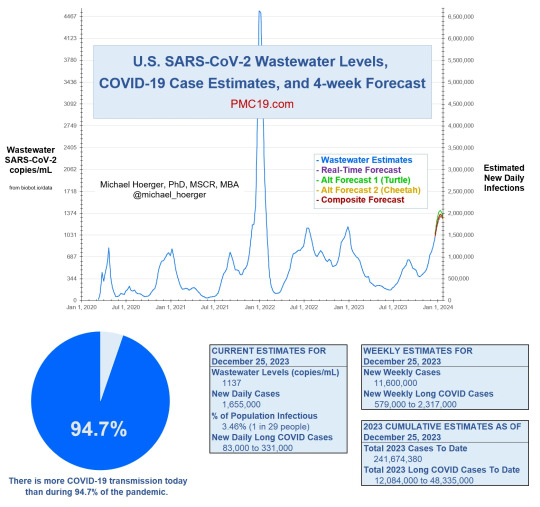
There is more COVID-19 transmission today (January 2024) than during 94.7% of the pandemic.
💉 Please get the updated (new, not a booster) Covid vaccine. If you're in the US, ask your local pharmacy about the Bridge Access Program for free vaccines. You can also search vaccines.gov then select Bridge Access Program participant.
If you do not want an mRNA vaccine for whatever reason, consider Novavax: it is protein-based like other typical vaccines from the last few decades, and many (including myself) report minimal side effects. Talk to your doctor if you have questions or concerns.
😷 Wear a mask in public and/or any enclosed areas. "Mask" means a respirator of KN95/N95 filtration or higher, not a cloth or surgical (blue) mask. Covid is airborne, so an airtight seal and particulate filter is necessary for protection. Different kinds of respirators are used for everything from toxic fumes to asbestos removal; when worn properly, they greatly reduce risk.
Here is a guide for proper use and fitting of a respiratory mask.
Here is a short video by 3M (respirator manufacturer) on the importance of fit-testing.
🧪 Have tests ready. With the new variants it can sometimes take 5-8 days to test positive, so be sure to test twice, 48 hours apart. If you're in the US, you can get 4 free rapid tests sent to your home through USPS. Local schools and libraries also may have free rapid tests. If you qualify for the Test to Treat program, you can receive free at-home NAAT tests and treatment for both flu AND Covid, and access to telehealth. The earlier you test positive, the more likely you will be eligible for treatment with Paxlovid.
🔁 If you can afford it, air purifiers and HEPA filters can help reduce transmission. Making a Corsi-Rosenthal box is simple and inexpensive. If weather permits, keeping windows open helps. Ventilation allows fresh air to circulate.
👃 Nasal sprays and CPC mouthwash are other useful prophylactic measures when used in conjunction with PPE and other modes of mitigation like masking and distancing.
🚬There is still a risk of Covid when outside, similar to exposure from secondhand smoke or a fire. Since Covid is spread through aerosols, it can hang in the air like smoke.
🐶 As with other coronaviruses, many household pets can get Covid. If you have been exposed, avoid contact with animals.
"But I'm not old or weak. Why should I care?"
☣ Covid can still kill you or disable you for life, even if your initial sickness is "mild". Even if you are young and have no preexisting conditions. 90% of the original "long haulers" had "mild" cases.
🩺 Covid increases your risk of stroke, blood clots, and heart disease by 2 to 5 times within a year of infection. It can also cause brain damage, which is part of the loss of taste and smell and cognitive symptoms like brain fog.
🩸 Covid is able to infect multiple organ systems because it travels through the bloodstream and attacks the mitochondria, leading to dysfunction and chronic fatigue.
⚠ Reinfection doesn't make your body better at fighting Covid; it just does more damage to your immune system, akin to HIV. A damaged immune system is worse at fighting off illness, more susceptible to infection, and can lead to serious complications like pneumonia. And with every reinfection, your chances of developing Long Covid increase. Therefore, the best protection for your immune system is to avoid getting Covid as much as possible.
I know everyone is tired of this. But if there was any time to be vigilant, it is now. Please, let's protect each other.
305 notes
·
View notes
Text

Those of you who have watched The Sandman may not realize that the epidemic mentioned early on in the show, where over a million people were affected by a strange sleeping sickness, encephalitis lethargica, was a real thing. …
It didn’t all happen overnight. The first cases were diagnosed in 1917, and the incredibly odd disease continued to turn up in nations around the world over the following decade. Over 500,000 people are thought to have died from the disease over that period …
But dying wasn’t what really marked out the strangeness of the disease. Many of those affected were trapped in a kind of half-life, neither fully awake nor wholly asleep. They could get up and walk, if assisted. But without intervention would sit silently for days. …
The cause of this disease is still unknown. Because it overlapped the massive flu pandemic, many have suspected that lethargica might be a “sequelae,” an after effect of infection by the 1918 flu virus. This theory has fallen out of favor lately, but remains a possibility. …
Like COVID-19, we largely think of flu as a respiratory disease. However, like COVID-19, flu actually effects a number of organs and systems. A sharp increase in heart attacks coming years, and even decades, later, have been connected to the 1918 flu. …
There is even evidence of decreased life expectancy among children born to infected parents. That’s on top of the millions of infants who died as a direct result. The associated health issues generated economic patterns that could still be detected over 50 years later. …
In addition, just as with COVID-19, “long flu” was common. Many people took years to recuperate from their encounter with that flu. Many never did. Again, there are patterns of poverty that are detectable as a direct result. …
What kind of sequelae will COVID-19 generate, and how will they effect not just individual lives, but our socioeconomic future? Absolutely no one knows. What we do know is that 210,000 Americans have already died from COVID-19 *this year*. Millions are experiencing long COVID. …
In absolutely no sense is this pandemic over. As schools start up in America, everyone seems to be, sadly, shockingly, unforgivably left to make their own decisions. Just remember, what we do now will be with us into the next century.
Oh, and I left out that Encephalitis lethargica had its own sequelae: a worldwide increase in Parkinsonism. This was not a kind disease, whatever its origin.
#like the flu#encephalitis lethargica#sandman#covid#long covid#post-viral sequelae#spanish flu#so fucking tired of that ignorant statement#me/cfs
2K notes
·
View notes
Text
"Two-thirds (910 of 1350 [67.4%]) of individuals with long illness were asymptomatic beforehand."
Note the usage of "long illness" instead of Long COVID. This is the upcoming round of minimization and obfuscation rearing its head.
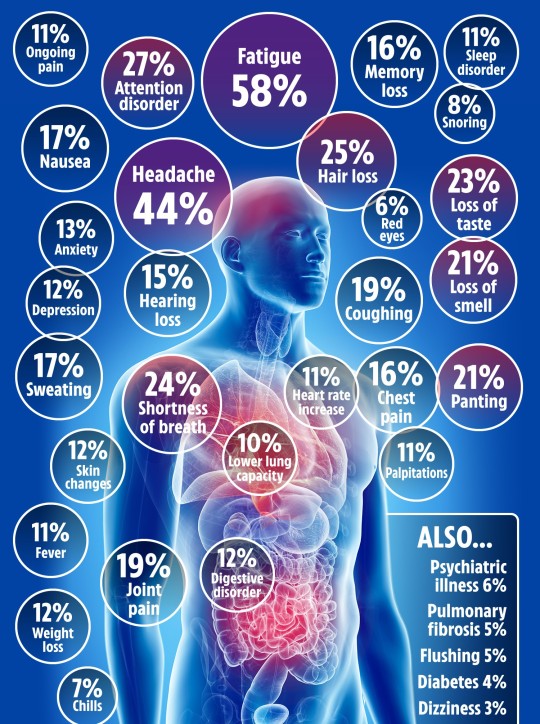
(Infograpic made with info from this 2021 study)
#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#long covid#covid is airborne#wear a mask#coronavirus
40 notes
·
View notes
Text
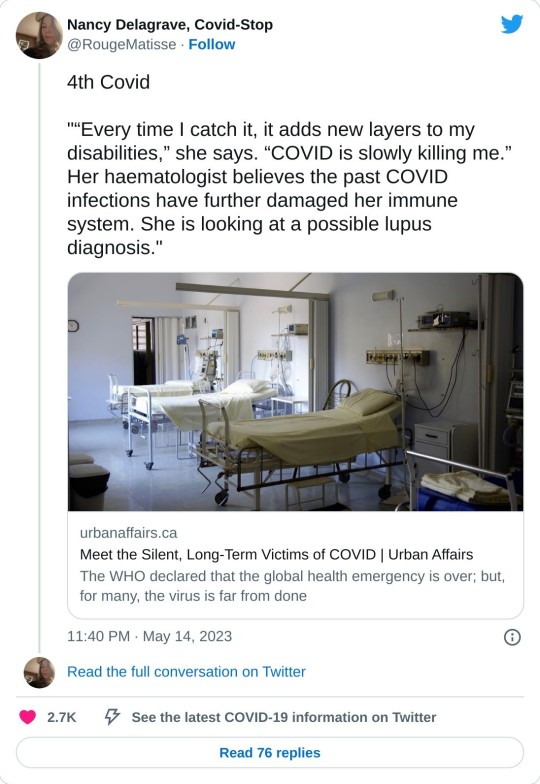
Just a few days before our interview, Jill’s (Ed: not her real name) immunologist sent her to the hospital to rule out pulmonary embolism, which happens when a blood clot gets stuck in an artery of the lung. In Jill’s case it would be a Long COVID symptom amongst many others she had been battling over the last year: including swelling around the tissue of her heart, memory deficits, sudden heart-rate surges, fatigue and abnormal kidney test results.
By that point, she’d had COVID four times, despite taking stringent precautions. She was born with a primary immune deficiency. And, without a fully functioning immune system she needs weekly injections of human immunoglobulins from plasma donations. A very small viral load can make her sick and she’s at a much higher risk of severe outcomes from COVID than most people.
“Every time I catch it, it adds new layers to my disabilities,” she says. “COVID is slowly killing me.” Her haematologist believes the past COVID infections have further damaged her immune system. She is looking at a possible lupus diagnosis.
Her voice is raspy and soft over the phone. She pauses when I ask how she is doing.
“Well, I got COVID,” she says. “Again.”
At the hospital appointment several nurses were not wearing their masks properly, and one kept pulling it down to talk with Jill, who had to remove hers to get her lungs checked. As someone who is very isolated with her family — everyone works and goes to school from home — Jill believes that the appointment led to her most recent infection.
She’s always been careful with her health but in the past, she worked in the school system. By 2020 she moved to a remote position and at that time still had many options for safely connecting with those around her and she could attend health-care appointments without concern. About a year ago, nearly all restrictions were lifted in Alberta and that’s when she got her first COVID infection.
Three years in, nearly everyone she knows has moved on including — most bafflingly to her — many of the medical professionals she sees. But, Jill says, moving on is not a privilege afforded to people like her.
Recently, PCR testing became inaccessible to health-care providers, who, in the past, were able to test regularly. And while Alberta Health Services (AHS) still requires masks, any health-care settings outside AHS can make their own rules. So, once masking was no longer mandated in public settings, many dropped requirements — this includes many of the specialists seeing immunocompromised people, including those Jill now sees due to Long COVID.
“The variants have been left to run rampant and I have really become more and more scared,” she says.
“Governments are saying: Oh we can re-open because we have all these tools. But they are not available to the immunocompromised population. So, the monoclonal antibodies are no longer effective against the current variants. Because the variants are so immune-based, the vaccines were never particularly effective for immunocompromised people because of the nature of our immune systems.”
As well, Jill says that there are many contraindicated drugs that cannot be taken with Paxlovid, the drug which is used to treat COVID patients in specific circumstances. According to Health Canada, Paxlovid “is used in adults to treat mild to moderate coronavirus disease 2019 (COVID-19) in patients who have a positive result from a severe acute respiratory syndrome Coronavirus 2 viral test and who have a high risk of getting severe COVID-19, including hospitalization or death.”
She still takes the vaccines with hopes they will help, and while she believes Paxlovid is saving her life with this current infection, she says it is not a guarantee against more Long COVID symptoms. And, for the infection prior to the current one, the drug was not available due to a kidney infection caused by the virus.
“I have to access my medication, my health care. And by people not masking around me, I have no way to protect myself,” she says. “If you don’t want to wear masks as a society then you are going to leave the immunocompromised people behind.” And she says many high risk people are not able to work from home, or have their kids in online classes or maybe struggle to afford masks or air purifiers — many social and financial issues make individual protections far more challenging or impossible. She is currently in a court battle with her ex.
“He wants increased access, in-person school and group extracurricular activities. All things that put me at higher risk of infection,” says Jill.
Recently, she went to her cardiologist to find that no patients or staff were masking.
“I really realize now I have to be my own advocate,” she says.
She has to constantly think ahead. So, she now calls beforehand to see if the appointment can be done remotely or if the staff can mask. She’s also decided to start carrying around a laminated sheet that explains her medical condition as it is often something she needs to repeat at each appointment or in the emergency room.
Like many others, she’s found ways to navigate her way around a harrowing array of risks. And yet, even with all these precautions, she can not control the actions of others which can directly affect her health.
Holly (Ed: not her real name), is retired and lives in a small community just outside Edmonton. She’s currently thinking about her next visit to her doctor, who hasn’t been taking precautions from the beginning.
“It’s exhausting always trying to get around how there is no protection for us anymore,” she says. “I’m thinking why am I made to feel crazy when my own doctor won’t wear a mask? Won’t acknowledge that it’s airborne?”
But the worst part, she claims, was that he minimized the effects of COVID, saying it was rarely an issue and only affects a certain demographic. Holly does not believe that is true, but regardless it is of little comfort when her husband, who’s in his 70s, has chronic health complications.
“I think patients are rightfully concerned, particularly when they go in for health care,” says physician Neeja Bakshi. “I think the medical community should be doing whatever we can to protect those who are coming in.”
It’s true, she says, that hospitals are no longer overwhelmed, and fewer people are dying; there is less of an acute emergency. But COVID is still circulating, people are still dying, and Long COVID (aka post COVID-19 condition) should be on everyone’s radar.
Recently, the World Health Organization announced an end to the global health emergency. But it also said earlier that “one in 10 infections result in post COVID-19 condition suggesting that hundreds of millions of people will need longer term care.”
COVID can cause organ damage — particularly affecting the heart, kidneys, skin. Plus, there’s risk of brain and immune damage, along with increased risks for cancer and autoimmune disease.
And, while no one knows yet how long that damage could persist, a study published in the Journal of the Royal Society of Medicine says 59 per cent of Long COVID patients had organ damage a year later.
In 2022, Bakshi started a Long COVID clinic at her health facility Park Integrative Health, treating patients from across Canada. Every week she completes upwards of 20 disability forms for people who need to take time off work due to the debilitating effects of Long COVID.
While certain health complications make Long COVID more likely, anyone can be affected regardless of the severity of their infection or the state of their health. The indiscriminate nature of COVID is one of the things that’s been most shocking to Bakshi. She’s treated a number of elite athletes who went from performing at a professional level to struggling to have enough energy to brush their teeth.
Many patients struggle with stigma not just from medical professionals but from family, friends and employers. It’s an invisible illness, says Bakshi, so patients may look fine and are often misdiagnosed as something psychosomatic.
“I’m immersed in the world. But I don’t feel like you can deny it exists. And I think it’s a bit of ignorance on the medical community’s part if they say they don’t know anything about Long COVID. There are very specific disease patterns and symptoms,” says Bakshi.
There is also a lack of support. The most proven management strategy for Long COVID or even any COVID infection is recovery and rest, says Bakshi. But that’s not possible for many people. Initially, in 2020, there was forced rest through quarantine periods, but that time off has become shorter, as employers don’t have to pay for employees to be off at all.
“We are not a society that is built on support. We’ve already set ourselves up to fail from a recovery perspective,” says Bakshi.
Jill has found validation in Bakshi’s clinic as one of her patients. But that experience stands out amongst a sea of specialists who have given up on precautions.
“Instead of recommending upgraded masks, air cleaners and UV, or working from home, immunologists that manage my condition recommend wearing a mask if you want and enjoying your life—as short as that may be. I am not sure if this is complacency, or giving up… Either way, education and change need to happen or far too many valuable lives will be lost and disabled unnecessarily,” says Jill.
Savvy AF. Blunt AF. Edmonton AF.
243 notes
·
View notes
Text
In 2020, Robert Kuciemba, a woodworker in San Francisco was infected by a co-worker after his Nevada-based Victory Woodworks transferred a number of sick workers to the San Francisco site for a few months
Victory Woodworks knew some employees might be sick but they transferred them anyway and ignored a San Francisco ordinance in place at the time to quarantine suspected covid cases
Kuciemba was subsequently infected and he then infected his wife, who ended up in ICU on a ventilator. There's a few stunning details to this case:
First, the court agreed that there is no doubt the company ignored the San Francisco health ordinance. In other words, they accepted the company had broken the law but still...
Second, the US Chamber of Commerce, the largest business lobbying organisation got involved and helped the company with its defence. This is a tiny company in a niche industry. Their involvement tells us a lot about the importance of the principle they knew was at stake.
Third, the defence of the company is very telling. “There is simply no limit to how wide the net will be cast: the wife who claims her husband caught COVID-19 from the supermarket checker, the husband who claims his wife caught it while visiting an elder care home." Well, exactly
The California Supreme Court ruled against Kuciemba on the basis that a victory, while, in the court's words, "morally" the right thing to do, would create "dire financial consequences for employers" and cause a "dramatic expansion of liability" to stop the spread of covid.
This case reveals what many of us suspected but haven't seen confirmed in so many words: the public health imperative of controlling a pandemic by making employers liable for some of that control is, and always must be, secondary to capitalist profit
[author's ko-fi link]
78 notes
·
View notes
Text
The Weather
This week we see a sharp increase of COVID in all regions, likely due to increased travel around the recent holiday long weekend and dropping temperatures that bring a lot of gatherings indoors. As the holiday season continues, we remind our readers to use layers of protection — such as ventilation, air purification, masking with a KN95/N95 or better, and testing via PCR or NAAT or testing serially with rapid antigen tests — to protect themselves and their loved ones both during travel and at your holiday gatherings.
Repeat COVID infection has serious implications for everyone, not just the elderly or those with preexisting conditions. Even if you experience a mild case, COVID is a vascular disease that causes multiple organ damage, autoimmune conditions, inflammation and immune system dysregulation that you might not necessarily experience at the time of your infection. It’s important to note that if you or your loved ones have experienced previous COVID infections, you may have entered a high risk group for severe effects and hospitalization without realizing it.
Some people may feel worn down by the current state of the virus, by fatigue of lack of resources, or from the energy spent protecting one’s self from an infection; with increasing wastewater levels and the onset of a new dominant variant this week, now is really the crunch time to stay strong and endure. For those who have stopped precautions, we invite you to return to masking and other levels to minimize transmission. This is the most important time to return to masking to protect yourself and others.
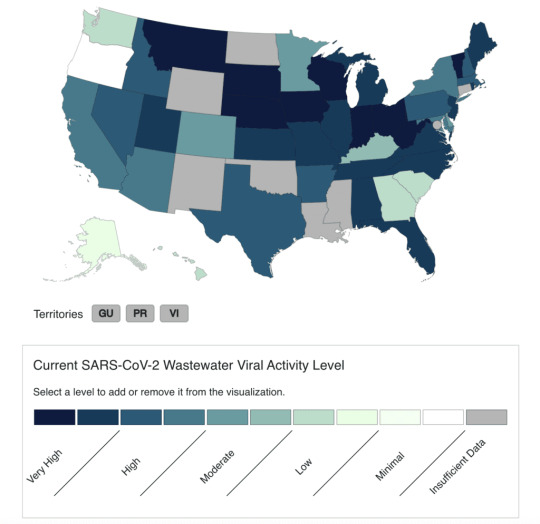
The Current Wastewater Viral Activity Map shows viral activity by state. As of 12/02/23, many states are reporting “very high” to “high” COVID levels with 5 states reporting low levels. Seven states reported no data.
The CDC currently rates our nationally reported COVID wastewater viral activity levels as “high”.
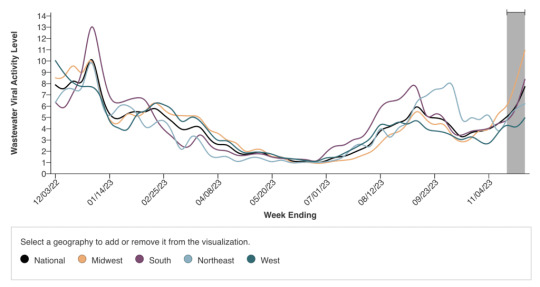
Levels are at an incline in all regions, but the Midwest takes a strong lead with a viral activity level of 10.94. This is a wastewater value that surpasses all readings for the Midwest in the past 2 years, and is the third highest of any reading since the onset of the Omicron variant in January of 2022 where we saw the highest levels of spread we have experienced in the entirety of the pandemic. Current Midwestern wastewater levels were surpassed only by a viral activity level of 13.02 in the South on 12/31/2022 and of 11.79 in the West on 07/02/2023.
As with Biobot data, the most recent two weeks (indicated by gray shading on the graph) are subject to change due to reporting delays.
As we enter the cold and flu season when many in-person gatherings are held, we encourage you to continue monitoring local reports for a more accurate measure of levels. Also, please continue to use and support others in using layers of protection. And as we continue to report on advocacy successes, remember that our actions and voices can enact change — this level of unchecked spread is unacceptable and we must demand better resources and protections from our policy makers!
Deaths
Percentage of total deaths in the US caused by COVID has risen 25% in the past week. Remember that these numbers are an undercount related to reporting delays in place since the Biden Administration ended the Public Health Emergency. Alarmingly, the current increase in deaths is large enough to show despite these changes.

COVID remains the third leading cause of death according to the CDC in the US. COVID is the highest single cause of death, only second to Heart Disease and Cancer which are both umbrella headings for more specific diseases. We mourn all those who have died due to COVID, and in that mourning, call you to take measures to prevent death and disablement for yourself, your loved ones, and your communities.
Ventilation and Air Filtration
Moving activities outdoors or ensuring your indoor setting has consistent fresh airflow is key to ensuring high quality ventilation. We recommend monitoring carbon dioxide levels and making adjustments as needed. Air filtration is important as well. If you’re looking for a HEPA air purifier or Corsi-Rosenthal Box for your family, it is important to get a filtration device that is powerful enough to change out the air for your particular room size. Clean Air Stars has created a free tool to calculate which filter could be right for you depending on the size of the rooms that you wish to clean and how many people will be attending your gathering.
Testing
Whether you are making the trip home or staying in one place this holiday season, with the current level of spread it is important to know your COVID status before engaging in social activity.
Rapid antigen tests are designed to be “the most rapid” at telling those who are symptomatic whether the symptoms they are experiencing are or are not caused by COVID. If you are asymptomatic, presymptomatic, or less than 5 days out from your COVID exposure, using one single rapid test is not an effective way of determining whether or not a person is currently infected with and contagious with COVID.
Persons using rapid antigen tests should take at least 2 rapid antigen tests 48 hours apart from one another and isolate in between, in order to avoid spreading their unconfirmed case as well as avoid exposure to COVID during this waiting period, which could produce a false test negative result. Persons who are experiencing COVID symptoms but test negative on an initial rapid antigen test also need to isolate themselves from others, assume they have COVID, and test again in 48 hours. Persons who are asymptomatic or pre-symptomatic who experience 2 negative serial tests must mask or isolate and wait a final 48 hours to test a third time in order to confirm a negative COVID case. For this reason, rapid antigen tests are only ideal to use in preparation for events where the user has a week prior available to test multiple times and isolate.
FDA approved home Nucleic Acid Amplification Tests or NAATs are a more sensitive home test option, some brands of which have been found to, with only one test, verify both positive and negative results at 92.9% and 98.7% respective accuracy. NAATs can be a more sensitive, quicker option to use in preparation for events.
Another more recent clinical trial found that performing a combined throat and nose sample increased sensitivity for healthcare worker and self-collected specimens. When testing at home with a rapid antigen test, it is worth it to take a combination sample like this one.
To ensure the most sensitive results for both symptomatic and asymptomatic cases, get a PCR test. No-cost PCR testing sites that are available via the federal ICATT program can be found via this search tool. Remember to also check for regional offerings such as NYC’s COVID express test centers that test for COVID, RSV, FLU A and FLU B free of cost with results typically returned by end of day, that could be a more convenient option for you. PCR testing is the gold standard if you are making plans to be in a social setting.
If you do not have fast free PCR testing in your area, demand that it be made publicly available by the government at all levels!
Wins

Grassroots organizing group and “Mask Blocs” continue to take to social media encouraging Pro-Palestine protesters to continue to wear masks in their organizing spaces and during protests highlighting historic use of unrestricted and eugenic viral spread as a weapon of occupation and colonization.
The National Institutes of Health’s Home Test to Treat program has upgraded its free test offerings and now instead of rapid antigen tests, will provide LUCIRA by Pfizer home NAAT tests can that effectively detect asymptomatic and pre-symptomatic COVID infections as well as Flu A and Flu B. Those who are uninsured or underinsured can sign up for this program to access free NAAT testing, telehealth services, and treatment medications for COVID and the Flu.
If your household has not placed a new order for more rapid tests from the federal government through covidtests.gov, you can still place an order for 4 free rapid antigen tests here.
Take Action
If you are out protesting this weekend or planning your trip home to visit family for the holidays, connect with your local COVID advocacy group to pick up high quality masks for yourself and to pass on to those around you.
This Tuesday, December 12th, the director of the CDC and the American Medical Association are hosting a virtual fireside chat to discuss Fall & Winter Respiratory Virus Season (prior registration required). We encourage you to attend. You might ask the CDC why they aren’t ensuring precautions in healthcare settings? Or you could ask why they’re relying on a reactive, vaccine-only approach instead of layers of protection to proactively prevent COVID?
#op#img#covid#covid news#covid pandemic#covid 19#covid-19#covid19#coronavirus#pandemic#medical#medical news#pcdc#people's cdc#wear a mask#covid isn't over#described in alt text
40 notes
·
View notes
Text
In photos of 2023’s World Economic Forum- or Davos as it is commonly called, after the Swiss resort town where it annually occurs- you might not notice the HEPA filters. They’re in the background, unobtrusive and unremarked upon, quietly cleansing the air of viruses and bacteria. You wouldn’t know- not unless you asked- that every attendee was PCR tested before entering the forum, or that in the case of a positive test, access was automatically, electronically, revoked. And if you happened to get a glimpse of the strange blue lights overhead, you could reasonably assume that their glow was simply a modern aesthetic choice, not the calming buzz of cutting edge Far UVC technology- demonstrated to kill microbes in the air.
It’s hard to square this information with the public narrative about COVID, isn’t it? President Biden has called the pandemic “over”. The New York Times recently claimed that “the risk of Covid is similar to that of the flu” in an article about “hold outs” that are annoyingly refusing to accept continual reinfection as their “new normal”. Yet, this week the richest people in the world are taking common sense, easy- but strict- precautions to ensure they don’t catch Covid-19 at Davos.
These common sense, easy precautions include high-quality ventiliation, use of Far UVC-lighting technology, and PCR testing. You’ll also see some masks at Davos, but generally, the testing + air filtration protocol seems to be effective at preventing the kind of super-spreader events most of us are now accustomed to attending.
It seems unlikely to me that a New York Times reporter will follow the super-rich around like David Attenborough on safari, the way one of their employees did when they profiled middle-class maskers last month. I doubt they will write “family members and friends can get a little exasperated by the hyper-concern” about the assembled Prime Ministers, Presidents and CEOs in Switzerland. After all, these are important people. The kind of people who merit high-quality ventilation. The kind of people who deserve accurate tests.
Why is the media so hellbent on portraying simple, scientifically proven measures like high-quality ventilation as ridiculous and unnecessary as hundreds of people continue to die daily here in the US?
Why is the public accepting a “new normal” where we are expected to get infected over and over and over again, at work events with zero precautions, on airplanes with no masks, and at social dinners trying to approximate our 2019 normal?
We deserve better. We deserve to be #DavosSafe as the hashtag going around on twitter puts it. Your children deserve to be treated with the care that world leaders are treating each other. Your family deserves to be protected from the disease which is still- unlike the flu- the third leading cause of death in the US. We don’t deserve to be shoved back into poorly ventilated workplaces while our politicians and press assure us that only crazy people would demand to breathe clean air.
Clean water and clean food are rights we fought for; we have regulatory bodies that ensure we aren’t exposed to pathogens via our water supply nor our food. In 1854, John Snow famously conducted his Broad Street Pump study in London and demonstrated that cholera was water-bourne; however, it took decades for our public policy to catch up with our scientific knowledge.
A public health case study published by the NBCI describes the years that followed:
The first use of chlorine as a disinfectant for water facilities was in 1897 in England. The first use of this method for municipal water facilities in the United States was in Jersey City, New Jersey, and Chicago, Illinois, in 1915. Other cities followed and the use of chlorination as standard treatment for water disinfection rapidly grew. During the 20th century, death rates from waterborne diseases decreased significantly, and although other additional factors contributed to the general improvements in health (such as sanitation, improved quality of life, and nutrition), the improvement of water quality was, without doubt, a major reason.
Forty-three years passed from the initial demonstration that pathogens were being spread via water, and public action and regulation to halt disease.
Can you imagine, in the 1890s, being somebody who argued against cleaning the water?
Can you imagine, in those years of plentiful cholera, calling the people who demanded shit-free water “hold outs”?
One thing COVID realists are accused of is being “doomsayers” and “fearmongers,” so let me share a dose of optimism about the future with you. When we choose- whenever we choose- to get COVID under control, there’s an exciting new world awaiting us. One, not only without constant COVID reinfection, but where our kids can grow up free of colds, flus, RSV, and many other common bugs. And no, contrary to what you may have heard, staying healthy (shockingly enough) is not bad for children!
Once we choose to institute ventilation standards and introduce new technologies like Far UVC lighting- and embrace masking as an easy, kind, and useful tool to control outbreaks- we can bring every nasty airborne pathogen under control the way we did cholera. We didn’t have the science before; now we do. (I mean that quite literally; I can’t recommend enough the linked Wired article cataloguing the long journey to establishing that Covid is, indeed, airborne).
We face a stark choice; down one road, the one with zero infrastructure upgrades, no air quality regulations, and Covid safety only for those who can afford it, you and your family will get Covid this year. You will get Covid next year. You will continue to get Covid over and over and over again, as the health problems - like cardiac damage, viral persistance, and immune system dysfunction- continue to build up. (The billionaires, of course, will not).
Down the other road, we quite simply treat ourselves the way Davos would. We engage with what the science is telling us and we build a safer, better world for our kids. We embrace the lessons this pandemic is teaching us, and let go of things we now know are harming people. We stop clinging desperately to the idea that 2019 will come back if we just get the virus one more time, and we come together to achieve what we’ve been told is impossible: elimination.
The economic elite thrive on our divisiveness and blame casting. They don’t mind that we’re calling each other names, engaging in racial stereotyping, or leaving disabled people to die, so long as we keep their machine running. But we can choose to stop throwing blame at each other, and direct it where it belongs: at the powerful people who’ve left us to suffer, at the politicians who are whipping people into a frenzy over masks instead of over our millions of dead, at the talking heads on TV that work so hard to convince us: you want to get sick. It’s better than being a *weirdo* or a *hold out*.
We needn’t wait 43 years to redirect our energies. France and Belgium have already introduced new air quality standards, and DIY projects to build Corsi-Rosenthal boxes for schools and healthcare settings have popped up around the country. We have the science, we have the technology. All we need now is the political will and the solidarity to truly end the pandemic- the kind of solidarity the super rich always show with one another.
The billionaires at Davos don’t accept continual Covid reinfection. They demand better. It’s time we demand better too.
8K notes
·
View notes
Text
H5N1: What to know before fear spreads
What is H5N1?
H5N1 is a 1996 strain of the Spanish or Avian Flu first detected in Chinese birds before spreading globally across various avian species. H5N1 is similar to H1N1, but spreads slower and has a much higher mortality rate.
H5N1 may also be referred to as Influenza A. The American Association of Bovine Practitioners has seen fit to rename H5N1 to Bovine Influenza A Virus, or BIAV, and are encouraging others to use the same terminology.
I would not be surprised if the colloquial name among the public becomes Bovine Flu or American Flu in the coming months, and may be referred to as the Chinese Flu by the same folks who took the spark of the SARS-CoV-2 (COVID-19) pandemic as an excuse to be publicly racist to East Asian people without social repercussions.
BIAV is a virus, meaning that it is a (probably) non-living packet of self-replicating infectious material with a high rate of mutation. BIAV is structured similarly to SARS-CoV-2, having a packet of infectious material encased in a spherical shell with a corona, or crown, of proteins that can latch to living cells to inject RNA.
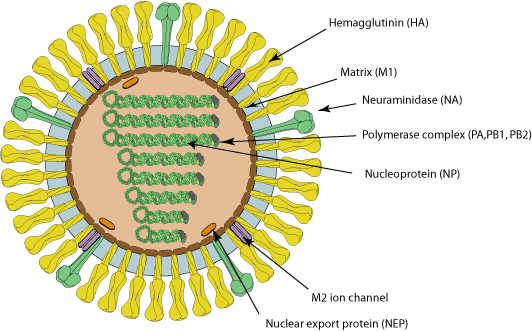
Image source with interactive model: ViralZone - H5N1 subtype
What is the history of BIAV?
In 1996 and 1997, an outbreak of BIAV occurred among poultry and infected 18 people in Hong Kong, 6 of which died. This seemingly isolated incident then infected ~860 people with a >50% death rate.
At the time, BIAV was known as Highly Pathogenic Avian Influenza, or HPAI, and killed nearly 100% of chickens within a 48 hour period.
From 2003 to 2005, continual outbreaks occurred in China and other East Asian countries, before spreading to Cambodia, the Netherlands, Thailand, and Vietnam.
From 2014 to 2016, it began being detected in American fowl, as well as mutating the H5N6 (lethal in birds, no human to human transmission) and H5N8 (largely spread through turkeys, ducks had immunity) viruses.
BIAV has since evolved into a clade known as 2.3.4.4b, and was first detected in 2021 in wild American birds. This then caused outbreaks in 2022 among wild and domesticated birds (such as chickens) alike, but was largely being overshadowed by the pressing SARS-CoV-2 pandemic at the time.
From 2022 to 2023, it was observed to be spreading among various mammals, including humans. Now, in 2024, we're having the most concerning rapid outbreak of BIAV since 2003.
BIAV is known to spread from mammal to mammal, particularly between cows and humans. BIAV may also be spread from cow to cow (highly likely, but not confirmed - this is likely the reason the virus has spread to Idaho from Texan cattle), and is known to be lethal to domestic cats and birds within 48 hours.
How does BIAV spread?
BIAV spreads through fomites - direct contact with infected animals or infected surfaces and then touching parts of your face or other orifices - as well as through airborne particulates, which may be inhaled and enter the sinuses and lungs.
BIAV is known to spread through:
Asymptomatic
Ducks, geese, swans, various shorebirds
Symptomatic, may be lethal
Foxes, bears, seals, sea lions, polar bears, domestic cats, dogs, minks, goats, cows, (potentially human to human, but unconfirmed - there have only been 8 potential human to human cases in 2024).
How can I protect against BIAV?
As BIAV is a type of Influenza A, existing protocols should do fine.
Current recommendations are to wash your hands vigorously after interacting with birds (I would also recommend doing this with mammals), avoid touching your face or other open orifices, and wear N95 masks.
Avoid sick or dead animals entirely - I would also recommend reporting them to your local Animal Control or veterinary centre and warning them about the infection risk. People who work with animals are recommended to also wear full PPE such as N95 masks, eye protection, gloves, and partake in vigorous hand washing.
If you suspect you've caught BIAV, seek medical attention immediately. Existing medications such as oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil can reduce BIAV's ability to replicate.
Standard flu shots will not protect against BIAV. Remember - symptoms of BIAV may not manifest for between 2 to 8 days, and potentially infected people should be monitored for at least 10 days.
How far has BIAV spread?
BIAV is currently a global virus, though the current infection location of note is the United States.
Image Key:
Dark red - Countries with humans, poultry and wild birds killed by H5N1
Deep red - Countries with poultry or wild birds killed by H5N1 and has reported human cases of H5N1
Light red - Countries with poultry or wild birds killed by H5N1
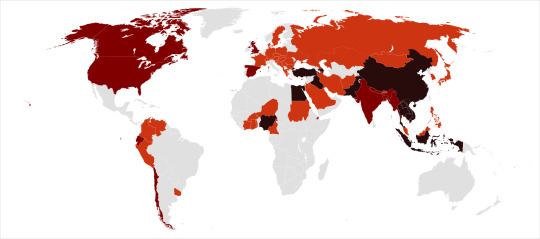
Image source: Wikipedia - Influenza A virus subtype H5N1 - File: Global spread of H5N1 map
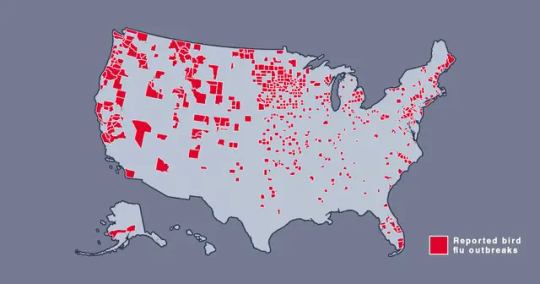
Image source: Metro.co.uk - Map shows where bird flu is spreading in US amid new warning - File: The Centers for Disease Control and Prevention’s H5N1 bird flu detections map across the United States
Should I be afraid?
You needn't be afraid, just prepared. BIAV has a concerningly high lethality, but this ironically culls its spread somewhat.
In the event human to human transmission of BIAV is confirmed, this will likely mainly affect marginalized communities, poor people, and homeless people, who are likely to have less access to medical care, and a higher likelihood of working in jobs that require frequent close human contact, such as fast food or retail jobs.
Given the response to SARS-CoV-2, corporations - and probably the government - may shove a proper response under the rug and refuse to participate in a full quarantine, which may leave people forced to go to work in dangerous conditions.
If this does spread into an epidemic or pandemic, given our extensive knowledge about Influenza, and the US having a backup vaccine for a prior strain of H5N1, a vaccine should be able to be developed relatively quickly and would hopefully be deployed freely without charge - we won't have to worry about a situation like The Stand.
Wash your hands, keep clean, avoid large social gatherings where possible, wear an N95 mask if you can afford them (Remember: Cloth masks are the least protective, but are better than nothing. If you can't afford N95 masks, I recommend wearing a well-fitted cloth mask with a disposable face mask over it to prevent pneumonia from moisture buildup in the disposable mask), support the disabled, poor, and homeless, and stay educated.
We can do better this time.
Further things to check out:
YouTube: MedCram - H5N1 Cattle Outbreak: Background and Currently Known Facts (ft. Roger Seheult, M.D.)
Wikipedia - Influenza A virus subtype H5N1
Maine.gov - Avian Influenza and People
CDC.gov - Technical Report: Highly Pathogenic Avian Influenza A(H5N1) Viruses
Wikipedia - H5N1 genetic structure
realagriculture - Influenza infection in cattle gets new name: Bovine Influenza A Virus (BIAV)
#H5N1#bird flu#avian flu#bovine flu#BIAV#pandemic#epidemic#COVID 19#coronavirus#spanish flu#long post#text post#no id#undescribed#news#politics#us news#us politics#american news#american politics#world news#global news#global politics#world politics#lgbt#lgbtq#queer#trans#communist#socialist
27 notes
·
View notes
Text
Weekly COVID-19 Update for 2023-12-24
COVID is still airborne, and COVID still very much isn't over.
Northeastern and Midwestern USA SARS2 virus levels in wastewater are *soaring*, Northeast is currently at 1500 copies/mL (~750 copies indicates a strong surge), and Midwest is at 1300 copies/mL. Southeastern and Western USA are maintaining relatively lower levels between 600 and 700 overall, but both are still climbing. See https://biobot.io/data for county-specific data as results can vary widely between locales.
How to reduce your risk of infection? The SARS2 virus is airborne and can spread like smoke, so #MaskUp with an #N95 or better, avoid superspreader events and locations, and stay up-to-date on your boosters. Do it for yourself, so you don't catch SARS-CoV-2, and for others, so you don't spread SARS-CoV-2. Even if you're fully vaccinated, your risk of developing #LongCOVID following an infection is lower but not zero, and multiple reinfections increase your odds of negative health outcomes. Plan A always should be to prevent an infection from developing by wearing a respirator with a good seal around your mouth and nose (FFP2, FFP3, KN95, N95, N99, P100, etc.).
Holiday tips:
-If someone tells you that COVID is over, you might ask them why, if we didn't consider COVID to be over in 2020 or 2021, when the COVID wastewater levels were lower, why should we consider it over now, when the virus is circulating in even higher amounts?
-"Fewer cases" doesn't mean much when most of the at-home rapid tests don't get counted in official records, and the most accurate PCR tests are neither freely available nor given to everyone getting on a plane or attending classes.
-"Fewer deaths" also means less when you remember that about 1,200,000 of the most vulnerable people already have died from it, COVID-19 remains the #3 cause of death in 2023 (behind heart disease and cancer, the risk of both of which may be increased by COVID), and the risk of a Long COVID/post-acute COVID syndrome (PACS) disability or other potentially life-shortening organ damage (brain, kidney, lung, immune, etc.) isn't measured just by the death count. Also, the USA's life expectancy still hasn't recovered from the drop it experienced following the start of the pandemic.
source: https://biobot.io/data
source: https://www.webmd.com/a-to-z-guides/news/20231006/these-are-the-top-10-causes-of-death-in-the-us
source: https://publichealth.jhu.edu/2022/covid-and-the-heart-it-spares-no-one
source: https://pubmed.ncbi.nlm.nih.gov/33914346/
source: https://www.usatoday.com/story/news/nation/2023/11/29/average-us-life-expectancy-increased-not-pre-covid/71738611007/
#covid#pandemic#corona#coronavirus#sarscov2#publichealth#science#disease#covidisntover#virus#medicine#sars2#covidisairborne#covidisnotover#health#lifeexpectancy
47 notes
·
View notes
Text
Who knew? Nearly three and a half years after Covid-19 first appeared on the scene, the World Health Organisation has declared the pandemic officially over.
And there we all were thinking it had ended more than a year ago, when the UK and much of the rest of Europe abandoned the last of their Covid restrictions.
Late to recognise Covid as a pandemic, the WHO has also been late to acknowledge that thanks in large measure to Western medicines and vaccines, it is also now essentially part of history.
Perhaps that's because of the continued influence of China, which only very recently abandoned its zero-Covid policy.
As long as a major economy was still imprisoning its citizens at the slightest sign of infection, then I suppose it was indeed hard to declare the disease no longer a public health emergency.
For most of us, the pandemic has nevertheless been over for a long time now.
The grimly dispiriting legacy is, however, still very much with us.
In the UK, the national debt is a fifth of GDP higher than it was, inflation has soared to double digits, economically sub-optimal work from home remains deeply entrenched, labour shortages abide, and many people still complain of long term sickness – much of it unrelated to Covid as such but seemingly triggered by the pandemic's deprivations – with record numbers claiming out of work benefits.
The Government's response to Covid always looked to me like a ruinous over-reaction, and I became something of a lockdown sceptic.
I say “something of” because in the initial stages of the pandemic – call it the “we're all going to die” phase – something fairly dramatic was obviously called for, watching the TV images of emergency hospitals being built in Wuhan and overwhelmed ICU units in Northern Italy.
Politically, it would have been virtually impossible for the UK to have stood alone in remaining open even as virtually the whole of the rest of Europe was closing down.
The Government would have fallen within weeks if it had stood by and done nothing.
Even Sweden, which seems to have got its approach about right, eventually implemented a watered down version of the restrictions imposed elsewhere.
Instinctively, Boris Johnson, then Prime Minister, was against lockdown, preferring instead the idea of “herd immunity”, but then he became seriously ill himself, and ended up fully embracing the made-in-China response.
For some, such as the former Supreme Court judge Lord Sumption – who would regularly warn of police state authoritarianism – the objection was on principled libertarian grounds.
This was, however, very much a minority position. One of the most remarkable things about the whole sorry affair is quite how compliant the country proved, and how quickly we succumbed to instruction.
Somewhat alarmingly, it turned out that supposedly freedom loving societies are remarkably willing to submit to authoritarian rule, especially if paid to stay at home, as was the case with furlough in the UK.
Even the Government was surprised by the obedience.
Yet it was always abundantly clear that these were essentially temporary, wartime measures that would be lifted once the emergency was over, so on those grounds at least, most of us were initially willing to go along with the heavy handed approach imposed.
No, what worried me was not so much the loss of liberty as the economic impact, and once the case mortality rate was confirmed at less than 1 percent for advanced economies, the lack of proportionality and cost benefit consideration.
I could never quite accept the argument that what was being done was similar to putting the economy into a medically induced coma, with the patient reawoken as if nothing had happened once the pandemic was over.
As we can now see, the lasting damage was monumental.
It would no doubt have been disastrous had the health service been overwhelmed, but when the main justification for lockdown becomes the rallying call of “protect the NHS” you have to ask yourself what the whole thing was really all about.
Insulating the health service from a sickness it is there to treat?
You cannot put a price on life, it can be argued, and therefore almost any cost is justified. It is also true that in the fog of war, mistakes are bound to be made; over-reaction is possibly better than under-reaction.
All the same, it now seems abundantly clear that the treatment was in many ways worse than the disease itself. We'll never know the counterfactual, or just how many lives were saved by imposing a strict series of lockdowns.
Most epidemiologists will tell you that it was a lot.
But they are not paid to think about the wider consequences, and it is now patently clear that the lasting damage to education, the economy and to wider public health was off the scale.
What are the lessons? We don't need to wait for the results of the official inquiry, still years away, to know some of the answers.
Let's make a start by examining the death toll, reported on a daily basis during the pandemic as if in some kind of international competition for how effectively each country was dealing with the crisis.
For a long time, Britain seemed to be bottom of the class, which in turn instructed the severity of the counter measures thought necessary.
The worse the numbers looked relative to others, the more draconian and prolonged the restrictions became.
Given differing methodologies and reporting systems, the best way of measuring the impact is not through recorded deaths from Covid, but via the excess death rate over and above what would normally be expected.
On this measure, most major advanced economies ended up in much the same place.
Britain was slightly worse than Germany and France, but not significantly so, and actually quite a bit better than Italy and Spain, according to estimates published in the Lancet.
This was not the impression you got at the time, when the British response was widely viewed as uniquely incompetent.
What is more, Scotland did worse than England, notwithstanding the plaudits the first minister, Nicola Sturgeon, received for outbidding Westminster on the countermeasures needed.
The same is true of Wales, whose first minister, Mark Drakeford, was similarly lauded for a more restrictive and therefore seemingly capable approach.
Well, not according to the numbers.
Culture wars, I'm afraid to say, are as likely to determine your view of the efficacy of lockdown as the underlying facts of the matter.
What we now know, however, is that lockdown is an extraordinarily costly way of dealing with a pandemic.
It is to be hoped that this lesson at least has been learned, and that the response to future pandemics will therefore be better calibrated to the severity of the disease.
A 1pc case mortality rate scarcely seems to justify what was done, even if it was admittedly much higher in older age cohorts.
A more consensual approach that keeps people properly informed but allows them to make their own choices on the degree of risk they are prepared to run must be the way forward.
#nunyas news#who knew?#lots of people did and you censored them#anyone that spoke out was ejected from the room
147 notes
·
View notes
Last Seen Blogs

lillyflover
NIE WOJNIE

suspensionofjudgement
Unconcealed

believexus
Do Not Underestimate Us

sysig
S, y s i g

umameninatimidapensadora
Roseanne Wimmer