#aapm
Text
Chapter 1 of the Good Omens Star Trek Trill AU is here!
0 notes
Photo

#pyaar #dosti #hai? #nah! #pyaar #bhagwaan #hai #aur #bhagwaan #kaha #hai? #aapme #mujhme #animals mai #pakshiyo mai https://www.instagram.com/p/CoV2gbXyYBs/?igshid=NGJjMDIxMWI=
0 notes
Text
Concise Guide to Developing a Neuroscience Based BBC Sherlock Holmes Esq Mind Palace
Following is a condensed and concise guide for you to develop similar sorts of mental mastery as Sherlock displays in the amazing British interpretation of Sir Conan Arthur Doyle's beloved character. I use this mind map everyday for basically everything and I don't think that there is any area of my life that hasn't been improved in someway by engaging with its mechanics.
This mindmap was designed to be useful in almost all life circumstances and there is a great deal of flexibility and modifications that can be made to its use to be tailored to your own particular needs to maximize utility and functionality
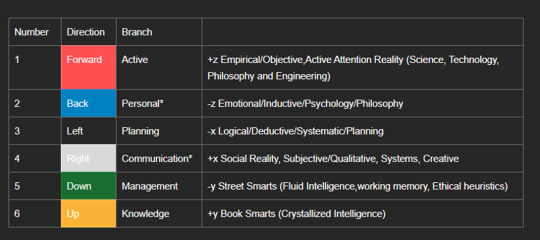
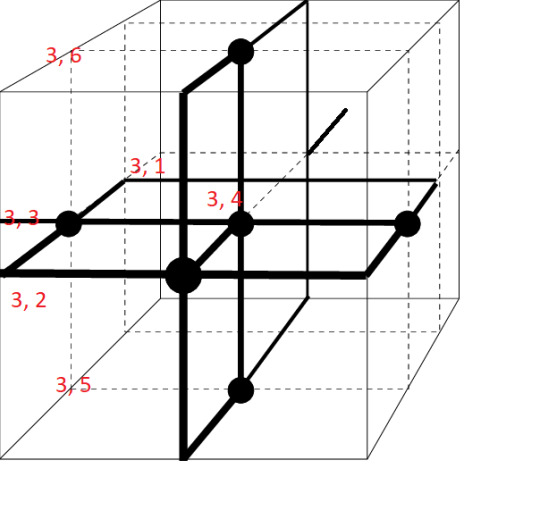
The key to this system is that there are six main inputs of which all you have to do is think of one of the six directions in orthogonal Euclidean space. I chose each direction in correlation to the general theme of the cognitive heuristic that you want to "activate" with the general function of the region of (the majority) of peoples brain has somewhat localized centers dedicated to said cognitive pattern.
The labelling of these directions is arbitrary and feel free to define your own characterization or order of inputs however I just listed my ontology as is I use it IRL.
+z/-z -> 1, 2 (or forward/back) respectively
-x/+x -> 3, 4 (or left/right) respectively
-y/+y 5, 6 -> (pr down/up) respectively
It is key to keep in mind of your mind that -z is essentially just the direction that your eyes face as set in your skull for a point of reference.
Below is a table summarizing these inputs along with a brief description of each directions psychological and cognitive theme
Each "direction" can be further broken down by applying the six inputs again which results in six main branches and thirty six sub branches, the initial thematic aspect behind the choice of the first six inputs are extrapolated and carried through into the assignment of the sub set of the thirty six sub branches so there is a degree of logical organization of the resultant four dimensional meta cognitive structure (four dimensions as inputs will be repeatedly done temporally as needed)
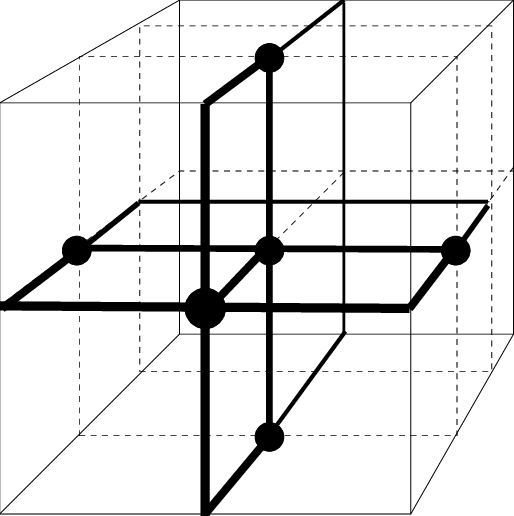
The mental representation of the MM will look like the image above with the caveat that in all Euclidean directions, there would be an addition MR unit facing out of each plane which would be 1, 1/2, 2/3,3/4,4/5,5/6,6 respectively. Also inputs that "bounce back" such as 1, 2/2,1 3,4/4,3 and so on are considered to be unique inputs as its the pathing and tracing out of these inputs mentally which acts non-combinatory to result in a total of thirty six unique sub branches.
There may be a lot of unfamiliar terminology, especially acronyms which I have developed just mostly for my own use before I decided to put this memeplex out into cyberphysical reality, if there are any terms or concepts that anyone is unsure about feel free to ask but I am going to define everything in Unsignificant Sentience eventually.
Key to understanding and using this list is that each integer corresponds to one pole of a base Euclidean axis
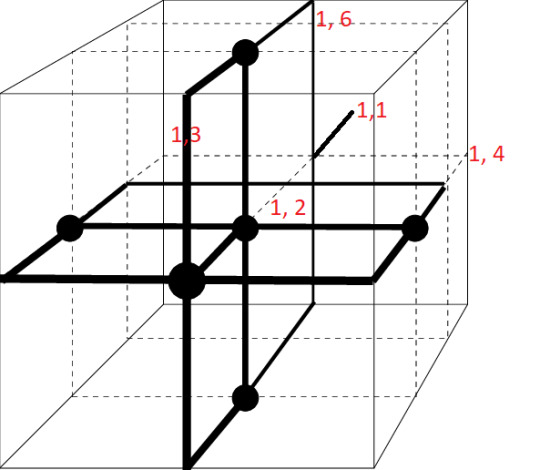
One: active
1 1 Sense, Attention and Action (Non-selective/Selective and/or Undirected/Directed Attention), AAPM (Active Attentional Perception Model)
1 2 Perceiving, Observing, and Introspection, SVD
1 3 Logic, MM Model Axioms and Experimentation, ISR, EGC Outcomes
1 4 Assessment Describing, +y/MR/ME EIOSA Modelling
1 5 CBT, BH, Working Memory
1 6 Specific Thinking, Frame Encoding, and MEs Applications and Management (Inter branch/Sub Branch)
In your minds eye the pathing thought trace input should result in something like this.
Two: personal
2 1 All Current Recursive Conscious Perception (EIOSA Analysis/Awareness)
2 2 Narrative, Identity Management, Frames, Auxiliary SA/EMA, Qualia
2 3 R4, ME, (in vivo UJF Functionality/Integration)
2 4 Beliefs, Values, Hopes, Ethics, Dreams (+DRD4 content)
2 5 Memory, Mnemonics, AE Encoding and Recall
2 6 Consciousness + VSM/UJS Models, Influencers (5 x) and CT Management CTx PPF, PQ
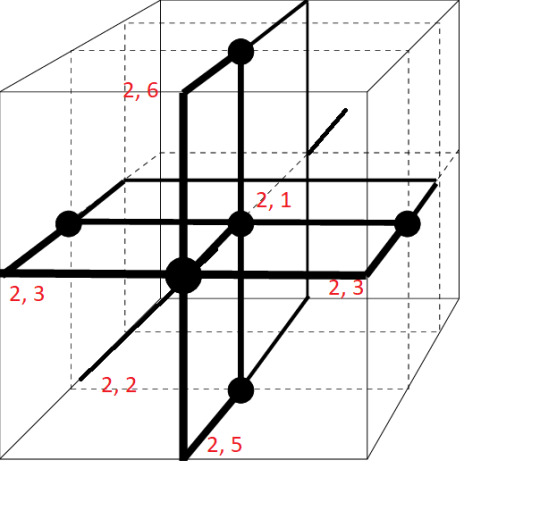
I will only fill out one more guide for the inputs for the Third Branch as it should be pretty easy to extrapolate the pattern by this point
Three: planning, logic, and structure
3 1 Dynamic Planning and Situational Awareness, (ME0002)
3 2 Skills and Technical Application/Adaption/Singular Module: Heuristic Focus
3 3 Active Goals and Projects/Schedule, Mnemonics
3 4 Habits/Predispositions/Routines/Baselines (SETS, Blooms Taxonomy) and limitations, Re (self-imposed and/or Real Boundaries), Frames and Physiological/Psychological Patterns
3 5 Resource Management
3 6 Ideas or Future Goals and Projects/Personal Engineering, USF, CMM, NWF
Four: Systems, Creative, and Communication
4 1 Agent Based, Observance and Interaction with Systems Associated and Context Awareness, ToM EIOSA
4 2 Persona and Ego Management
4 3 Reality, Social and Communication, Systems Identification/Interaction/Alteration/Mechanisms Options, Sets/OMA7, Objective EI IRL Network Corresponding to Meta Frameworks
4 4 MR/ME Grids + Practice/Enactment In Vivo
4 5 Communication and Sapir Whorf Language Management, Social Analysis and Responses
4 6 Ontology and Frame Engineering, Perspective Theory
Five: health
5 1 Physical Health (ER AnE + Diet/Hydration/Sleep/Medication)
5 2 Mental Health (ME0005/ME0010 Checks and Reconciliation)
5 3 Self Management and Contingencies
5 4 State of Other Systems, EISOA x, x,, (MR of Self Same) (States in Regards to Meta-Systems)
5 5 Applied Mindful Meditation, Self Awareness (Recursivity), and Reality Checking, PQ
5 6 Cognitive Health (DRD4 quality + CIA quality)
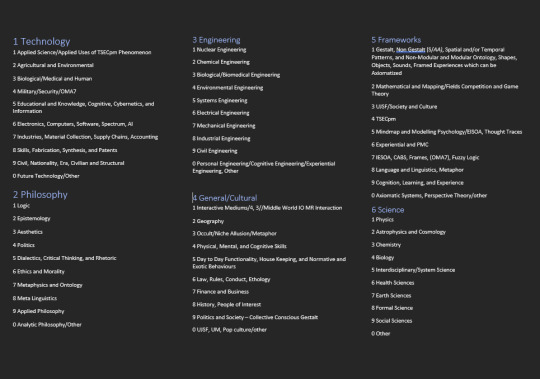
Six: knowledge
6 1 Technology
6 2 Philosophy
6 3 Engineering
6 4 General/Cultural
6 5 Frameworks
6 6 Science
Viable System Model based MM systems
The viable system model is a cybernetic theory and model utilized to model entities so that they remain viable and resilient in the fact of change. The model itself was derived from the physiological evo psych based compartmentation of function present in the human brain. I am going to do a post on VSMs at some point but the Wikipedia link is there if anyone is interested.
Below is a rough guide to what MM outputs correlate to each system in a viable system model
System One: 1 x , 3 3, 3 5, 6 x
System Two 2 1-3
System Three 3 1-3
System Four 4 x, 5 x, 6 x
System Five 2 4-6, 3 4-6
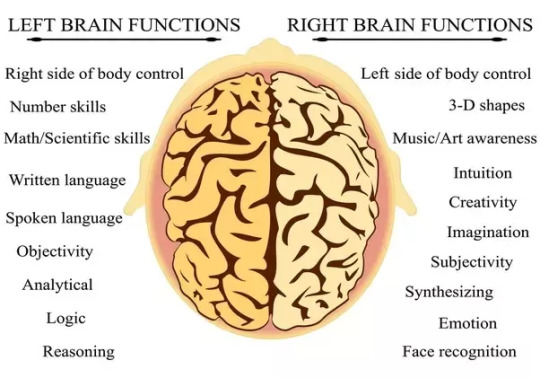
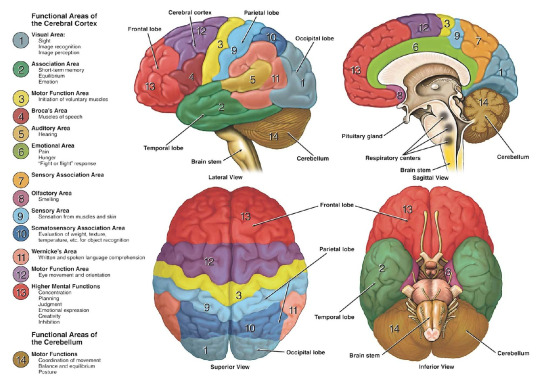
As shown by this highly scientific diagram, there is a general localization of specific cognitive and mental phenomena associated with each hemisphere and I hope that on some level that the mental action of enacting an input to the corresponding area of the brain that is more generally specialized in carrying out that processing might improve the effectiveness and/or efficiency of that given task. I would love to get an hold of an EEG and do some digging but that is a future project
So aside from forcing 42 specific commands into your brain, let alone the time required to practice utilizing this mind map in vivo, there is unfortunately another set within the +y knowledge branch where each domain of knowledge has ten subsets in order to break down learning and assimilating new information into more discrete chunks in order to facilitate recall and synthetizing of a priori knowledge.
This is one module of many such systems I have developed to try to be able to reproducibly able to self actualize on a daily basis.
There is an ungodly amount of extra details and systems that I have curated, developed, and refined regarding the MM and some of them are evident in some of the seemingly occult acronyms scattered throughout this document.
I was going to create an ARG game for later on in this year of 2023 after I finished the Unsignificant Sentience trilogy and I was going to make mechanics such as this MM part of the way to play the ARG and to get players immersed in the world building but I just want to get some of my ideas out there as I have been working on too many projects in a vacuum
I am done screaming into the void
#neurodivergencies#life hacks#mind map#psychology#geek#writing#sherlockbbc#mind palace#unsignificant sentience#neuroscience#science#physics#a guide to disgusie#cybernetics#biology
114 notes
·
View notes
Note
Tumhe apni godi mai chhipa dunga cutie
Sharm-o-haya h ya nahi aapme anon ji?
2 notes
·
View notes
Note
Ye Jo log jab aapke dharm ki beizzati karte hain aur in response agar bhi unke dharam ki beizzati karein? Toh aapme aur unme kya fark hai?
Meine kab kisi dharm ki beizzati ki ???
Meine toh tab bola jab samne Wale neh mere dharm ke mandiro ki jagah apna religious spot bana liya
Jo apne dharm ke liye lade hi na voh insaan hi kaisa.
Apne samne se Hume mauka Diya ki humlog apko kuch bole , vrna hum Hindus waise hi itne shant rehte h
And at the end I will still say I don't have any hate towards any religion
But if someone says against my religion I will definitely fight back, cuz I know my religion didn't colonize anyone's land or religious spots , we Hindus have feelings too towards our religion......
🙏🏼
4 notes
·
View notes
Note
A short haired desi princess! Aapki adaaon pe mar hi na jaaein ham 🫣
Aapke naino pe saare geet vaar dein! Saari shayariyan vaar dein par unke teekhe tevar ka koi muqabla nahi.
😳🤭💖🫶✨ you’re gorgeous Nandini😘
Ayee haaye, ab aapko hum kya kahe saari tareefon se toh aapne hume hi sajaa diya. Bas itna keh sakte hain ki jo khoobsurati aapko dusro mein dikhti hain woh aapme sabse zyaada hain <3
3 notes
·
View notes
Link
0 notes
Text
0 notes
Text
Sunita nahUA kissiki naukrani;Are bhai Woh Krishna KE sakha Sudamaa KE patni hain bhai?Kuchh Lihaz unke liye hona chahiye#@Krishnasudamaa ke kisse Dwapar;TretaSe Leke Kalyug tak zubaan zubaanSE, SABhiOS gyant Hoga;Agar thodaSA bhi insaniyatt Ho baki aapme;To Krishna Ke roop leke AAPSABHi; HiOS LOVE;SAX;DHOKABUHike Kushchit roop Hill Na dhare;Sudamazee Koo Bhalibhanti dhandaulatt Se help karne KE BAAZAI-Artificial Inteligence#@ Unka garibi KA mazaak Uda rahe Ho?Mujhe Mere Krishna Kanhaiya mill Gaye33crore jantaroopeople Hain;AAPSABHiOS,sosAamAdmi;Hum bhikharion Woh bhi Brahma mazaak To mat udaiye!mAadharM ka damana chod ke kissi sache sudamaazeebhole ko Apne pan ka ehsaas To dilaiye Kam SE kam mat rakhiye;Hum Krishna sakha SUDAMAASHANTADI MISHRAJIO
0 notes
Text
okay, the good omens star trek “and they were joined trills” au should be coming out tomorrow! which, of course, means it’s time for the teaser I’ve been promising:

0 notes
Text
Heartstopper's #YasminFinney reveals her Queerpiphany 🫶🏳️⚧️✨
Yasmin opens up to #Tayce & #MunroeBergdorf about what it's like to be a young role model and becoming the first transgender ...
via YouTube https://www.youtube.com/watch?v=AApM-xuDcLg
0 notes
Photo

Thanks for the kind words! ★★★★★ "These turned out adorable, very happy with the purchase!" Kelly V. https://etsy.me/3Y9CQJy https://www.instagram.com/p/CoXKXe-AAPm/?igshid=NGJjMDIxMWI=
0 notes
Text
What are the roles of ketamine in pain management?
Ketamine is a dissociative anaesthetic. The mechanism of action of ketamine in pain management is primarily an antagonism of the N-methyl-D-aspartate (NMDA) receptor. Recently, there has been a rise in research on the use of ketamine, particularly in lower sub-anaesthetic dosages. When used in such small dosages, ketamine acts primarily as an "anti-hyperalgesic," "anti-allodynic," or "tolerance-protective" substance. Therefore, rather than acting as an "analgesic" in and of itself, it plays a part in the treatment of opioid-resistant or "pathological" pain (central sensitisation with hyperalgesia or allodynia, opioid-induced hyperalgesia, neuropathic pain). Ketamine also has "preventive analgesia" qualities at low doses. Additionally, it offers practical and secure sedation and analgesia for unpleasant treatments in higher doses. The role of ketamine in treating chronic pain management and the effects of long-term medicinal use remain unclear.

Uses
Patients with chronic pain who have not found much relief from other painkillers or treatments and those who want to have surgery are typically the two groups of patients who may benefit from this drug.
Several illnesses, such as cancer, CRPS, fibromyalgia, neuropathic pain, phantom pain, postherpetic neuralgia, sickle cell disease, and spinal injury, may bring chronic pain. All of these disorders have seen the usage of ketamine to treat pain. The American Academy of Pain Medicine (AAPM), The American Society of Regional Anesthesia and Pain Medicine (ASRA), and the American Society of Anesthesiologists (ASA), have all concurred that the body of evidence supports the use of ketamine to treat pain associated with these conditions only weakly to moderately.
Ketamine dosage
Ketamine, when added to opioid-based analgesia in 0.1mg/kg - 0.2 mg/kg, reduces pain post 48 hours of surgery. This result is statistically significant but not in terms of clinical. Due to a lack of appropriate randomised controlled trials, the advantages and disadvantages of combining ketamine with potent painkillers like morphine for treating cancer pain have not yet been established. The role of ketamine in chronic pain is due to its effects on NMDA receptors.
In patients at risk for "pathological pain," such as pain associated with opioid tolerance, acute severe pain, neuropathic, ischemic, visceral, cancer, or CPSP, ketamine is most often used as an "anti-hyperalgesic," "anti-allodynic," or "tolerance-protective" substance. Low-dosage peri-operative ketamine has no clinically significant impact on acute postoperative pain in the critical context. Still, it is opioid-sparing and lowers nausea and vomiting in the sensitive postoperative period.
0 notes
Text
Krishnan Suthanthiran, Founder/President of TeamBest Global Companies Honored at AAPM’s First Post-Covid Annual Meeting
Krishnan Suthanthiran, Founder/President of TeamBest Global Companies Honored at AAPM’s First Post-Covid Annual Meeting
TeamBest Global Companies logo — http://www.teambest.com
Recipients of the AAPM BEST 2022 Awards.
Reverend Jesse Jackson (right) honors Mr. Suthanthiran (left) for his half a century of service and innovative contributions to medicine.
Krishnan Suthanthiran (right) accepting award (pictured with Congressman elect Jonathan Jackson (center) and his grandson (left).
Mr. Suthanthiran (left)…
View On WordPress
0 notes
Text

NBA News Today - 6/25/22 https://www.youtube.com/watch?v=1LJptr-AApM&utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text

NBA News Today - 6/25/22 https://www.youtube.com/watch?v=1LJptr-AApM&utm_source=dlvr.it&utm_medium=tumblr
0 notes
Last Seen Blogs

caradelevingne25
C.a.r.a

agua-con-canela
Desahogo Anónimo

xjustifiedxsundaysx
Smile Someday, Justified Sundays

placebopassion
Placebo Passion

peter4jx
Peter Shin