#Lewis Fogg
Text
I went through my house and collected most of the books that I have not read. There are more, but I wrote a list of the 100 books that I want to read relatively soon. If I start the challenge today, it can progress throughout this year and go into next year. By the end of 2023, I want to have read all these books.
Assassin’s Apprentice by Robin Hobb
A History of the English Language by Albert C. Baugh & Thomas Cable
The Power of One by Byrce Courtenay
Hogfather by Terry Pratchett
Nevernight by Jay Kristoff
Beyond Good and Evil by Friedrich Nietzsche
Criminology – A complete Introduction by Peter Joyce and Wendy Laverick
The Silmarillion by JRR Tolkien
Heidi by Johanna Spyri
Tarzan of the Apes and the Return of Tarzan by Edgar Rice Burroughs
Adventures of Huckleberry Finn by Mark Twainn
When Fashion Really Works by Marnie Fogg
Go the Distance – A Twisted Tale by Jen Calonita
The Museum of Things Left Behind by Seni Glaister
Trinity by Leon Uris
The Count of Monte Cristo by Alexandre Dumas
Makers of Rome by Plutarch
A Game of Thrones by George R.R Martin
Difficult Women by Helen Lewis
The Wreckage by Michael Robotham
The Twelve Caesars by Suetonius
Traitors by Frank Walker
A Fortunate Life by A.B. Facey
Traitor to the Blood by Barb & J.C. Hendee
Memoirs of a Geisha by Arthur Golden
Great Expectation by Charles Dickens
Heddy & Me by Susan Varga
No Silver Spoon by Katie Flynn
The Dance of Death and Other Stories by Algernon Blackwood
The Secret History by Donna Tartt
Wuthering Heights by Emily Bronte
Carrie by Stephen King
My Royal Story – Marie Antoinette by Kathryn Lasky
Theories of Race and Ethnic Relations by John Rex and David Mason
The Little Book of Psychology by DK
The World’s Greatest Idea by John Farndon
Don Quixote by Cevantes
The Survival Handbook by DK
Yes Yes Yes – Australia’s Journey to Marriage Equality by Alex Greenwich and Shirleene Robinson
The Grapes of Wrath by John Steinbeck
Wonder Woman Warbringer by Leigh Bardugo
The Fire of Joy by Clive James
Monsoon by Di Morrissey
Hamlet by William Shakespeare
Conquerers’ Road by Osmar White
The Art Book by DK
How to Garden by DK
How Science Works by DK
German for Everyone by DK
The History of the World by Alex Woolf
Cathy by Cathy Freeman
Song of Survival by Helen Colijn
Pet Semetary by Stephen King
The Crime Book by DK
The Bone Collection by Kathy Reichs
Basic Mandarin Chinese by Kubler & Wang
A Vindication of the Rights of Women by Mary Woolstonecraft
Joyland by Stephen King
The Jungle Book by Rudyard Kipling
The Scarlet Letter by Nathaniel Hawthorne
A Thousand Pieces of You by Claudia Gray
Gulliver’s Travels by Johanthan Swift
Eleanor Oliphant is Completely Fine by Gail Honeyman
Japanese Myths and Tales by Epic Tales
Eleni by Nicholas Cage
Psychology of Human Behaviour for Nurses by Dennis
Moby Dick by Herman Melville
More Rules for Life by Kitty Flanagan
Watership Down by Richard Adams
The Little Book of Politics by DK
Jews Don’t Count by David Baddiel
The Road by Cormack McCarthy
A Royal Duty by Paul Burrell
Jurassic Park by Michael Chrichton
Dracula by Bram Stoker
English Grammar Usage by McGraw Hill Education
Night at the Circus by Angela Carter
The Confidence Booster Workbook by Martin Perry
Ancient Egyptian Myths by Catherine Chambers
The Girl in the Picture by Denise Chong
Encyclopedia of Dinosaurs and Prehistoric Life by Miles Kelly
The Prince in the Heather by Eric Linklater
Simple Astronomy by DK
How to Kiss a Crocodile by Max Walker
The Fitness Instructor’s Handbook by Mark Coulson
Mool-nya-moonya Dreaming by Julie Tuckey
The No. 1 Ladies’ Detective Agency by Alexander McCall Smith
Pennies for Hitler by Jackie French
Boy Swallows Universe by Trent Dalton
Jane Eyre by Charlotte Bronte
The Shortest History of England by James Hawe
Mental by Dr Steve Ellen and Catherine Deveny
War and Peace by Leo Tolstoy
Work by Louisa May Alcott
Deranged Marriage by Sushi Das
Stranger the Dreamer by Laini Taylor
Emma by Jane Austen
The Alchemyst: The Secrets of the Immortal Nicholas Flamel by Michael Scott
The Book of Dust by Phillip Pullman
321 Seriously Smart Things You Need to Know by Mathilda Masters
Wish me luck.
4 notes
·
View notes
Text
Shortwood hit Kidlington for six
Kidlington Reserves 0
Shortwood 6
UHL Hellenic LeagueShortwood hit Kidlington for six to maintain their promotion push, writes Jim Cunneen.
Boss Ian Soule and assistant Lewis Fogg have assembled a squad to be reckoned with and added the signing of former Swindon Town defender Nathan Marks, who rejoins the club from Brimscombe, teaming up with his younger brother Keiran at Meadowbank
It only…

View On WordPress
0 notes
Text
Cardiovascular Disease Prevention Program for African American Women
Part I: Diagnosis
Mission Statement
To reduce the prevalence of cardiovascular disease among low- to middle-income African American women aged 35-50 years old living in the south-central Houston area by providing education regarding physical and mental health and their impacts on cardiovascular disease risk factors.
Cardiovascular Disease Among African American Women
Cardiovascular disease (CVD) is the leading cause of death for men and women in the United States, and there is a disproportionate burden of CVD seen in minority populations (Saban, Tell, & Janusek, 2019). African-American women (AAW) have the highest CVD rates in comparison to other ethnicities and genders. Compared to a prevalence of 36.1% in non-Hispanic white women, the prevalence of CVD in AAW was 48.3% in 2012 (Braun, Wilbur, Buchholz, Schoeny, Miller, Fogg, Volgman, & McDevitt, 2016). Moreover, cardiovascular health disparities among AAW are not fully explained by traditional risk factors (Saban et al., 2019). AAW experience additional CVD risk factors not experienced by men or women of other ethnic groups. Firstly, AAW have the highest rates for many CVD risk factors such as obesity, diabetes, hypertension, and physical inactivity (Ebong & Breathett, 2020). The article by Ebong & Breathett (2020) list many characteristics about AWW. They found that AAW are the least likely group to participate in physical activity, and the majority of AAW do not eat their recommended amounts of fruits and vegetables. They write that the reason for this is likely a result of deep-rooted, constant institutional and cultural oppression. In addition to the systemic formulation of racially segregated environments, AAW often live in areas with limited access to resources, limited educational opportunities, inadequate and/or unaffordable housing, high crime rates, and limited access to and/or prejudicial health care services. These circumstances experienced uniquely by AAW facilitates health behaviors associated with the development of CVD. Secondly, AAW are more likely to be affected by psychosocial risk factors than women of other ethnic groups (Copeland, Newhill, Foster, Braxter, Doswell, Lewis, & Eack, 2017). Many AAW must cope with chronic life stressors associated with racism and discrimination. In the study by Copeland et al. (2017), the authors write that the negative emotional response precipitated from such stressors elevates cortisol, adrenaline, and epinephrine levels, and overall heightens cardiovascular activity. Chronically, this physiological response increases the chances of developing CVD.
Because the traditional risk factors for CVD do not explain the health disparities seen in AAW, researchers have been looking into the connection between mental health status and CVD. Studies have found that individuals suffering from depression are 50% more likely to develop CVD, and AAW report symptoms of depression at higher rates in comparison to their White counterparts (Copeland et al., 2017). A possible explanation for this is the systemic disadvantages experienced by AAW and their resulting effects on mental health. Psychosocial stressors affect minority populations at a greater rate, especially African Americans. Remaining in a constant fight-or-flight mode physiologically can lead to an accumulation of visceral fat, high blood pressure, and hyperglycemia (Sims, Glover, Gebreab, & Spruill, 2020). Researchers also suggest AAW’s poor health behaviors may be a coping response to psychosocial stressors (Sims et al., 2020). This would explain the higher rates of diabetes, obesity, and hypertension among AAW. As stated by Copeland et al. (2017), the aforementioned bio-psycho-social factors that contribute to the poor mental health outcomes of AAW are collectively recognized as the ‘triple jeopardy’ of being African American, female, and impoverished.
Fortunately, researchers have found a connection between positive mental outlooks and lower CVD risks. Some studies show it is possible to reduce CVD risk when mental health issues are addressed. The study by Saban et al. (2019) found that resiliency can reduce the effect social stressors have on an individual’s risk of developing CVD and can improve risk factors. They write that higher resilience is seen to reduce the activation of stress response hormones and improve the physiologic response to stress. Another psychological attribute being studied associated with improved cardiovascular outcomes is gratitude. Evidence demonstrates that dispositional gratitude can actually foster protective factors against depression and improves the effect psychosocial stressors have on the body (Cousin, Redwine, Bricker, Kip, & Buck, 2020). Strengthening an individual’s sense of gratitude and spirituality is a possible way to improve AAW cardiovascular health.
Why This is a Problem
First and foremost, this is a public health problem because the observed disparities are a result of sociocultural risk factors that are otherwise completely preventable. Primary prevention practices, such as visiting a doctor and getting regular health screenings, should be a priority for this population, but evidence shows African Americans are less likely to participate in routine medical checkups compared to White Americans (Smedley, Stith, & Nelson, 2003). AAW who seek healthcare to improve their CVD risk factors often run into the same racial and discriminatory exposures within the health care system that they do in other areas of society. To make matters worse, the strongest evidence for the existence of racial and ethnic disparities in healthcare is found in studies of cardiovascular care, as noted by Smedley et al. (2003). Among their discoveries, researchers found that there is an underuse of treatment services amid racial and ethnic minorities. This either suggests that physicians are less likely to offer treatment services to minority patients, or minority patients are more likely to refuse treatment services. They also find that there is evidence supporting the theory that the race of a patient influences physicians’ decisions regarding diagnosis and treatment recommendations. In one study, physicians rated African American patients as least intelligent, more likely to abuse drugs/alcohol, and more likely to fail to comply with and participate in treatment protocols. AAW that seek to improve their cardiovascular health may be essentially deemed not worthy enough due to a physician’s implicit negative racial stereotype. Though physicians may be acting on their implicit biases, but AAW are still being negatively affected.
Additionally, there is a legacy of distrust among healthcare providers and racial minorities in America that may make AAW less likely to accept healthcare services and/or procedures. In the same study by Smedley et al. (2003), evidence suggests minority patients may be more receptive and trusting of physicians who are minorities themselves. However, minority physicians represent only 9% of the physicians in the country; of the 9%, one-third is African-American. AAW who have perceived discrimination from White physicians are less likely to seek health care and are even less likely to find a healthcare provider they feel they can trust. This could be the reason AAW are more likely to avoid healthcare services altogether.
Existing Programs
Successful Programs
AAW are more likely to have multiple CVD risk factors at one time, so interventions that target multiple risk factors are necessary for success (Ebong & Breathett, 2020). The Love Your Heart program was a 12-week nutrition and physical activity intervention that aimed to reduce cardiovascular risk factors among African American women living in the Boston area (Rodriguez, Christopher, Johnson, Wang, & Foody, 2012). This program was culturally tailored for African American women, and it used a self-help group methodology to address the physical, mental, emotional, and spiritual aspects that affect weight and cardiovascular health. The intervention included fitness classes, educational sessions spotlighting the importance of nutrition and exercise on CVD, group meetings and discussions, and personalized wellness plans. The results of the study found significant improvements in CVD risk factors. Comparing the pre-and post-test data, participants reduced their systolic blood pressure, body-mass-index, body weight, and waist circumference. This program highlights the effectiveness of community-based interventions that combine health information, individual support, and group support to lower CVD risk.
Another successful program, Prime Time Sister Circles, was a 10-week health program that aimed to improve diet and increase physical activity among African American women aged >35 years across the country (Gaston, Porter, & Thomas, 2007). It utilized the Social Cognitive Theory and Transtheoretical Model for program creation. The intervention was a curriculum-based approach to behavioral change and incorporated a support group appeal. The groups met once a week for 10 weeks and received information about spirituality, self-esteem, self-care, nutrition, exercise, CVD, and diabetes. This program is unique in that it also targeted stress-relief strategies. The results of the study found improvements in the participants self-reported stress management, physical activity, and nutrition. Data also shows that the program improved participants knowledge of CVD risk factors and attitudes towards prioritizing their health. This study is yet another that emphasizes the value culturally tailored interventions in support group settings have on reducing CVD risk in African American women.
Unsuccessful Programs
STEPS (Sisters Together Empowered for Prevention and Success) to a Healthier Heart was a 12- week, quasi-experimental, pre-posttest educational intervention that targeted AAW between 35 and 65 years of age (Brown, Alexander, Cummins, Price, & Anderson-Booker, 2018). The purpose of this health program was to assess if AAW’s general knowledge about risk factors of heart disease improved with participation in informational and physical activity sessions. The women chose to participate in either the intervention group, which involved information and physical activity sessions, or the comparison group, which received an informational packet only. The Coronary Heart Disease Knowledge Test was used to assess each participant’s knowledge of heart disease risk factors. This program was ultimately unsuccessful because, in comparing the pre- and posttest data, no significant changes occurred and there were no between-group differences. One possible reason this program was unsuccessful could be due to the use of standard surveys, and future studies should use a more reliable and valid measurement to assess knowledge among AAW. Another possibility is due to the intervention’s short duration with little attention on physical activity. This program underscores the importance of multicomponent, culturally tailored interventions that address multiple risk factors for AAW for success.
Part II: Planning
Program Goals and Objectives
Program Goal Number 1
Reduce the impact psychosocial stressors have on the priority population’s CVD risk.
Project Objective
By December 2021, when comparing pre-post test scores, one-half of the participants will report lower general stress as measured by the general stress subscale of the Chronic Stress Questionnaire (CSQ).
Health Education Objectives
- By the end of the first trimester, the majority of the participants will be able to list three healthy and three unhealthy stress and anxiety relief practices.
- Upon completion of the program, one-half of the participants will be able to identify stressors associated with racism and discrimination and effective coping methods.
- Six months after completion of the program, one-half of the participants will be able to list at least one coping and/or stress management skill utilized daily.
Project Objective
By June 2022, one-fourth of participants will report higher levels of resilience, in comparison to pre-test scores, as measured by the Conner-Davidson Resilience Scale (CD-RISC-25).
Health Education Objectives
- By the end of the second trimester, more than half of the participants will be able to identify factors that foster resilience.
- Upon completion of the program, one-fourth of the participants will be able to list three self-reflection practices.
Program Goal Number 2
Increase participation in physical activity and/or exercise that targets cardiac health among individuals in the priority population.
Project Objective
By June 2022, one-fourth of participants will engage in thirty minutes of moderate physical activity at least 3 times a week.
Health Education Objectives
- By the end of the first trimester, more than half of the participants will be able to identify three exercises that improve heart health.
- By the end of the first trimester, the majority of the participants will be able to identify three CVD risk factors associated with physical inactivity.
- One-half of the participants will be able to locate areas in the community with gyms and/or green space upon completion of the program.
Program Goal Number 3
Increase the awareness of primary and secondary prevention practices and their importance among individuals in the priority population.
Project Objective
By December 2023, yearly health care checkups among the participants will increase by 25%.
Health Education Objectives
- By the end of the second trimester, the majority of the participants will be able to identify two primary and two secondary prevention practices.
- By the end of the second trimester, the majority of the participants will be able to identify three CVD risk factors that are easily preventable by modifying behaviors.
- Upon completion of the program, one-third of the participants will be able to locate the nearest healthcare center in their community accessible to them.
- Upon completion of the program, one-fourth of the participants will be able to state the recommended schedule for healthcare screenings.
Theoretical Support of Intervention
Due to the high rates of depression seen among AAW, successful interventions must address both the physical and mental risk factors for CVD. The Transtheoretical Model (TTM) and the Social Cognitive Theory (SCT) will both be used to guide the development of this program (McKenzie, Neiger, & Thackeray, 2013). According to McKenzie et al. (2013), the TTM posits that behavior change happens over time, and that people move through five distinct “stages of change” phases in the process of adopting a health behavior change. This model has been effective for a variety of health behavior changes because it considers that people may begin in different stages. Most individuals will not respond to action-oriented behavior change programs because the majority are not prepared to act. Specific principles are applied at specific stages to maximize efficacy and ensure individuals move forward to the next stage. In other words, individuals are matched with interventions depending on the stage they are in. The SCT posits that learning happens in a social context. Individual experiences, environmental factors, and the actions of others influence health behavior. An important component of the SCT is reinforcement. Theorists believe reinforcement is essential for learning. Moreover, reinforcement with the addition of an individual’s expectations of the outcome is what determines behavior.
The reason I chose to use two theories is because mental needs to be addressed at a personal level, however, past programs have shown that AAW respond to interventions best when group support and social interactions are given. I chose the TTM because it addresses each participant as individuals. Some AAW may fare better in the face of adversity than others, so the mental health status of the participants is going to vary. Additionally, though some participants will share the same barriers to action, others are going to have barriers no one else has. This is the best intrapersonal level theory to use for many reasons. Firstly, we can implement interventions that can best facilitate change based on the stage the participants are in. Interventions that require immediate action will lose the participants that are not ready for action. By allowing the participants to progress through the stages on their own time ensures maximum participants retention in the program. The second reason I chose this theory was because of how well the Processes of Change correlate to what our participants are likely to go through throughout the intervention. For example, after learning more about the psychosocial factors, participants may begin to notice each time they are subjected to toxic, negative emotions due to their environment, which is explained by the process of dramatic relief. This will accompany the realization of the effects it has on them and their environment, which is explained by the constructs of self- and environmental reevaluation. Further, the intervention’s aim of finding new ways to cope with stressors and fostering resiliency is explained by the construct of counterconditioning. Lastly, as explained by the construct of social liberation, being able to effectively cope with negative emotions can/will allow the participants to focus their attention on all the positive experiences they have.
To target the interpersonal level, I chose the SCT because it addresses the influence that observational learning has on behavior. As stated above, similar programs with the most success have included group support/meetings in the intervention. Participants credited their continued participation and enthusiasm to the relationships they created with others and the desire to help one another succeed. Seeing others succeed due to a behavior change influences others to adopt that change as well. I also chose this theory because it addresses the idea of monitoring and adjusting behavior to gain control over it. This is the best interpersonal level theory to use because of the emphasis it has on learning in social contexts. We already know AAW respond best with group support, and the SCT has roots in learning from and believing in others. AAW who may not feel confident in the behavior changes will be encouraged by seeing other women succeed, or they will be encouraged to try when they see the support other participants are giving them. For example, participants will gain knowledge and skills about how to eat healthy after learning about healthy dinner options, as explained by the construct of behavioral capability. When a participant shares their meal plan that they have been following, positive feedback and praise from program instructors and other participants will help to maintain that participant’s behavior change, which is explained by direct reinforcement. On the other hand, participants who are struggling with that same behavior change may be encouraged to work for it after seeing the commendation others receive, as explained by vicarious reinforcement. To maintain this behavior, the participant will have to monitor and adjust their behavior, which is explained by the construct of self-control. As their self-control increases and their healthy eating behavior is maintained, they will gain confidence in their ability to create meaningful change in their life, as explained by self-efficacy.
Read the full article
0 notes
Text
Cardiovascular Disease Prevention Program for African American Women
Part I: Diagnosis
Mission Statement
To reduce the prevalence of cardiovascular disease among low- to middle-income African American women aged 35-50 years old living in the south-central Houston area by providing education regarding physical and mental health and their impacts on cardiovascular disease risk factors.
Cardiovascular Disease Among African American Women
Cardiovascular disease (CVD) is the leading cause of death for men and women in the United States, and there is a disproportionate burden of CVD seen in minority populations (Saban, Tell, & Janusek, 2019). African-American women (AAW) have the highest CVD rates in comparison to other ethnicities and genders. Compared to a prevalence of 36.1% in non-Hispanic white women, the prevalence of CVD in AAW was 48.3% in 2012 (Braun, Wilbur, Buchholz, Schoeny, Miller, Fogg, Volgman, & McDevitt, 2016). Moreover, cardiovascular health disparities among AAW are not fully explained by traditional risk factors (Saban et al., 2019). AAW experience additional CVD risk factors not experienced by men or women of other ethnic groups. Firstly, AAW have the highest rates for many CVD risk factors such as obesity, diabetes, hypertension, and physical inactivity (Ebong & Breathett, 2020). The article by Ebong & Breathett (2020) list many characteristics about AWW. They found that AAW are the least likely group to participate in physical activity, and the majority of AAW do not eat their recommended amounts of fruits and vegetables. They write that the reason for this is likely a result of deep-rooted, constant institutional and cultural oppression. In addition to the systemic formulation of racially segregated environments, AAW often live in areas with limited access to resources, limited educational opportunities, inadequate and/or unaffordable housing, high crime rates, and limited access to and/or prejudicial health care services. These circumstances experienced uniquely by AAW facilitates health behaviors associated with the development of CVD. Secondly, AAW are more likely to be affected by psychosocial risk factors than women of other ethnic groups (Copeland, Newhill, Foster, Braxter, Doswell, Lewis, & Eack, 2017). Many AAW must cope with chronic life stressors associated with racism and discrimination. In the study by Copeland et al. (2017), the authors write that the negative emotional response precipitated from such stressors elevates cortisol, adrenaline, and epinephrine levels, and overall heightens cardiovascular activity. Chronically, this physiological response increases the chances of developing CVD.
Because the traditional risk factors for CVD do not explain the health disparities seen in AAW, researchers have been looking into the connection between mental health status and CVD. Studies have found that individuals suffering from depression are 50% more likely to develop CVD, and AAW report symptoms of depression at higher rates in comparison to their White counterparts (Copeland et al., 2017). A possible explanation for this is the systemic disadvantages experienced by AAW and their resulting effects on mental health. Psychosocial stressors affect minority populations at a greater rate, especially African Americans. Remaining in a constant fight-or-flight mode physiologically can lead to an accumulation of visceral fat, high blood pressure, and hyperglycemia (Sims, Glover, Gebreab, & Spruill, 2020). Researchers also suggest AAW’s poor health behaviors may be a coping response to psychosocial stressors (Sims et al., 2020). This would explain the higher rates of diabetes, obesity, and hypertension among AAW. As stated by Copeland et al. (2017), the aforementioned bio-psycho-social factors that contribute to the poor mental health outcomes of AAW are collectively recognized as the ‘triple jeopardy’ of being African American, female, and impoverished.
Fortunately, researchers have found a connection between positive mental outlooks and lower CVD risks. Some studies show it is possible to reduce CVD risk when mental health issues are addressed. The study by Saban et al. (2019) found that resiliency can reduce the effect social stressors have on an individual’s risk of developing CVD and can improve risk factors. They write that higher resilience is seen to reduce the activation of stress response hormones and improve the physiologic response to stress. Another psychological attribute being studied associated with improved cardiovascular outcomes is gratitude. Evidence demonstrates that dispositional gratitude can actually foster protective factors against depression and improves the effect psychosocial stressors have on the body (Cousin, Redwine, Bricker, Kip, & Buck, 2020). Strengthening an individual’s sense of gratitude and spirituality is a possible way to improve AAW cardiovascular health.
Why This is a Problem
First and foremost, this is a public health problem because the observed disparities are a result of sociocultural risk factors that are otherwise completely preventable. Primary prevention practices, such as visiting a doctor and getting regular health screenings, should be a priority for this population, but evidence shows African Americans are less likely to participate in routine medical checkups compared to White Americans (Smedley, Stith, & Nelson, 2003). AAW who seek healthcare to improve their CVD risk factors often run into the same racial and discriminatory exposures within the health care system that they do in other areas of society. To make matters worse, the strongest evidence for the existence of racial and ethnic disparities in healthcare is found in studies of cardiovascular care, as noted by Smedley et al. (2003). Among their discoveries, researchers found that there is an underuse of treatment services amid racial and ethnic minorities. This either suggests that physicians are less likely to offer treatment services to minority patients, or minority patients are more likely to refuse treatment services. They also find that there is evidence supporting the theory that the race of a patient influences physicians’ decisions regarding diagnosis and treatment recommendations. In one study, physicians rated African American patients as least intelligent, more likely to abuse drugs/alcohol, and more likely to fail to comply with and participate in treatment protocols. AAW that seek to improve their cardiovascular health may be essentially deemed not worthy enough due to a physician’s implicit negative racial stereotype. Though physicians may be acting on their implicit biases, but AAW are still being negatively affected.
Additionally, there is a legacy of distrust among healthcare providers and racial minorities in America that may make AAW less likely to accept healthcare services and/or procedures. In the same study by Smedley et al. (2003), evidence suggests minority patients may be more receptive and trusting of physicians who are minorities themselves. However, minority physicians represent only 9% of the physicians in the country; of the 9%, one-third is African-American. AAW who have perceived discrimination from White physicians are less likely to seek health care and are even less likely to find a healthcare provider they feel they can trust. This could be the reason AAW are more likely to avoid healthcare services altogether.
Existing Programs
Successful Programs
AAW are more likely to have multiple CVD risk factors at one time, so interventions that target multiple risk factors are necessary for success (Ebong & Breathett, 2020). The Love Your Heart program was a 12-week nutrition and physical activity intervention that aimed to reduce cardiovascular risk factors among African American women living in the Boston area (Rodriguez, Christopher, Johnson, Wang, & Foody, 2012). This program was culturally tailored for African American women, and it used a self-help group methodology to address the physical, mental, emotional, and spiritual aspects that affect weight and cardiovascular health. The intervention included fitness classes, educational sessions spotlighting the importance of nutrition and exercise on CVD, group meetings and discussions, and personalized wellness plans. The results of the study found significant improvements in CVD risk factors. Comparing the pre-and post-test data, participants reduced their systolic blood pressure, body-mass-index, body weight, and waist circumference. This program highlights the effectiveness of community-based interventions that combine health information, individual support, and group support to lower CVD risk.
Another successful program, Prime Time Sister Circles, was a 10-week health program that aimed to improve diet and increase physical activity among African American women aged >35 years across the country (Gaston, Porter, & Thomas, 2007). It utilized the Social Cognitive Theory and Transtheoretical Model for program creation. The intervention was a curriculum-based approach to behavioral change and incorporated a support group appeal. The groups met once a week for 10 weeks and received information about spirituality, self-esteem, self-care, nutrition, exercise, CVD, and diabetes. This program is unique in that it also targeted stress-relief strategies. The results of the study found improvements in the participants self-reported stress management, physical activity, and nutrition. Data also shows that the program improved participants knowledge of CVD risk factors and attitudes towards prioritizing their health. This study is yet another that emphasizes the value culturally tailored interventions in support group settings have on reducing CVD risk in African American women.
Unsuccessful Programs
STEPS (Sisters Together Empowered for Prevention and Success) to a Healthier Heart was a 12- week, quasi-experimental, pre-posttest educational intervention that targeted AAW between 35 and 65 years of age (Brown, Alexander, Cummins, Price, & Anderson-Booker, 2018). The purpose of this health program was to assess if AAW’s general knowledge about risk factors of heart disease improved with participation in informational and physical activity sessions. The women chose to participate in either the intervention group, which involved information and physical activity sessions, or the comparison group, which received an informational packet only. The Coronary Heart Disease Knowledge Test was used to assess each participant’s knowledge of heart disease risk factors. This program was ultimately unsuccessful because, in comparing the pre- and posttest data, no significant changes occurred and there were no between-group differences. One possible reason this program was unsuccessful could be due to the use of standard surveys, and future studies should use a more reliable and valid measurement to assess knowledge among AAW. Another possibility is due to the intervention’s short duration with little attention on physical activity. This program underscores the importance of multicomponent, culturally tailored interventions that address multiple risk factors for AAW for success.
Part II: Planning
Program Goals and Objectives
Program Goal Number 1
Reduce the impact psychosocial stressors have on the priority population’s CVD risk.
Project Objective
By December 2021, when comparing pre-post test scores, one-half of the participants will report lower general stress as measured by the general stress subscale of the Chronic Stress Questionnaire (CSQ).
Health Education Objectives
- By the end of the first trimester, the majority of the participants will be able to list three healthy and three unhealthy stress and anxiety relief practices.
- Upon completion of the program, one-half of the participants will be able to identify stressors associated with racism and discrimination and effective coping methods.
- Six months after completion of the program, one-half of the participants will be able to list at least one coping and/or stress management skill utilized daily.
Project Objective
By June 2022, one-fourth of participants will report higher levels of resilience, in comparison to pre-test scores, as measured by the Conner-Davidson Resilience Scale (CD-RISC-25).
Health Education Objectives
- By the end of the second trimester, more than half of the participants will be able to identify factors that foster resilience.
- Upon completion of the program, one-fourth of the participants will be able to list three self-reflection practices.
Program Goal Number 2
Increase participation in physical activity and/or exercise that targets cardiac health among individuals in the priority population.
Project Objective
By June 2022, one-fourth of participants will engage in thirty minutes of moderate physical activity at least 3 times a week.
Health Education Objectives
- By the end of the first trimester, more than half of the participants will be able to identify three exercises that improve heart health.
- By the end of the first trimester, the majority of the participants will be able to identify three CVD risk factors associated with physical inactivity.
- One-half of the participants will be able to locate areas in the community with gyms and/or green space upon completion of the program.
Program Goal Number 3
Increase the awareness of primary and secondary prevention practices and their importance among individuals in the priority population.
Project Objective
By December 2023, yearly health care checkups among the participants will increase by 25%.
Health Education Objectives
- By the end of the second trimester, the majority of the participants will be able to identify two primary and two secondary prevention practices.
- By the end of the second trimester, the majority of the participants will be able to identify three CVD risk factors that are easily preventable by modifying behaviors.
- Upon completion of the program, one-third of the participants will be able to locate the nearest healthcare center in their community accessible to them.
- Upon completion of the program, one-fourth of the participants will be able to state the recommended schedule for healthcare screenings.
Theoretical Support of Intervention
Due to the high rates of depression seen among AAW, successful interventions must address both the physical and mental risk factors for CVD. The Transtheoretical Model (TTM) and the Social Cognitive Theory (SCT) will both be used to guide the development of this program (McKenzie, Neiger, & Thackeray, 2013). According to McKenzie et al. (2013), the TTM posits that behavior change happens over time, and that people move through five distinct “stages of change” phases in the process of adopting a health behavior change. This model has been effective for a variety of health behavior changes because it considers that people may begin in different stages. Most individuals will not respond to action-oriented behavior change programs because the majority are not prepared to act. Specific principles are applied at specific stages to maximize efficacy and ensure individuals move forward to the next stage. In other words, individuals are matched with interventions depending on the stage they are in. The SCT posits that learning happens in a social context. Individual experiences, environmental factors, and the actions of others influence health behavior. An important component of the SCT is reinforcement. Theorists believe reinforcement is essential for learning. Moreover, reinforcement with the addition of an individual’s expectations of the outcome is what determines behavior.
The reason I chose to use two theories is because mental needs to be addressed at a personal level, however, past programs have shown that AAW respond to interventions best when group support and social interactions are given. I chose the TTM because it addresses each participant as individuals. Some AAW may fare better in the face of adversity than others, so the mental health status of the participants is going to vary. Additionally, though some participants will share the same barriers to action, others are going to have barriers no one else has. This is the best intrapersonal level theory to use for many reasons. Firstly, we can implement interventions that can best facilitate change based on the stage the participants are in. Interventions that require immediate action will lose the participants that are not ready for action. By allowing the participants to progress through the stages on their own time ensures maximum participants retention in the program. The second reason I chose this theory was because of how well the Processes of Change correlate to what our participants are likely to go through throughout the intervention. For example, after learning more about the psychosocial factors, participants may begin to notice each time they are subjected to toxic, negative emotions due to their environment, which is explained by the process of dramatic relief. This will accompany the realization of the effects it has on them and their environment, which is explained by the constructs of self- and environmental reevaluation. Further, the intervention’s aim of finding new ways to cope with stressors and fostering resiliency is explained by the construct of counterconditioning. Lastly, as explained by the construct of social liberation, being able to effectively cope with negative emotions can/will allow the participants to focus their attention on all the positive experiences they have.
To target the interpersonal level, I chose the SCT because it addresses the influence that observational learning has on behavior. As stated above, similar programs with the most success have included group support/meetings in the intervention. Participants credited their continued participation and enthusiasm to the relationships they created with others and the desire to help one another succeed. Seeing others succeed due to a behavior change influences others to adopt that change as well. I also chose this theory because it addresses the idea of monitoring and adjusting behavior to gain control over it. This is the best interpersonal level theory to use because of the emphasis it has on learning in social contexts. We already know AAW respond best with group support, and the SCT has roots in learning from and believing in others. AAW who may not feel confident in the behavior changes will be encouraged by seeing other women succeed, or they will be encouraged to try when they see the support other participants are giving them. For example, participants will gain knowledge and skills about how to eat healthy after learning about healthy dinner options, as explained by the construct of behavioral capability. When a participant shares their meal plan that they have been following, positive feedback and praise from program instructors and other participants will help to maintain that participant’s behavior change, which is explained by direct reinforcement. On the other hand, participants who are struggling with that same behavior change may be encouraged to work for it after seeing the commendation others receive, as explained by vicarious reinforcement. To maintain this behavior, the participant will have to monitor and adjust their behavior, which is explained by the construct of self-control. As their self-control increases and their healthy eating behavior is maintained, they will gain confidence in their ability to create meaningful change in their life, as explained by self-efficacy.
Read the full article
0 notes
Photo

That’s how BFF work~
✏️ Text transcript:
Chise: Why are Maribel and Carol sitting with their back to each other?
Lewis: They had a fight.
Chise: Then why are they holding hands?
Lewis: They get sad when they fight.
_________________
• Text from @scatterpatter‘s Incorrect Quotes Generator
• Kokoro♡Clock Precure, fanseries by @rainbowmiraclestar & @pinceauarcenciel (More infos on the FancureParadise wikia)
#Kokoro Clock Precure#precure fanseries#precure oc#pretty cure#short comic#incorrect quotes generator#Carol Fogg#Maribel Boushizuku#Chise Kisaki#Lewis Fogg#My OC art#my art#actually Chise and Lewis lines could have been swaped
53 notes
·
View notes
Photo




🎀💙 Kokoro♡Clock Precure Aesthetics ☕💜
Maribel • Cure Dentelle | Carol • Cure Jasmin
Chise • Cure Ceylan | Lewis • Cure Gear
Credits:
All pictures © Pixabay
✨Link on FancureParadise Wikia✨
#my edits#precure#kokoro clock precure#aesthetics#maribel boushizuku#carol fogg#chise kisaki#lewis fogg#cure dentelle#cure jasmin#cure ceylan#cure gear
21 notes
·
View notes
Photo
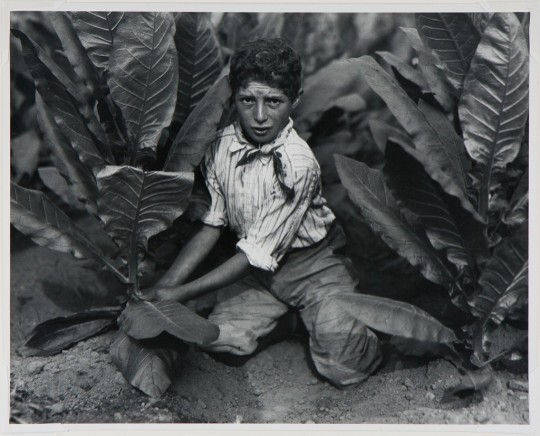
Picking Tobacco, Oklahoma, Lewis Wickes Hine, 1916, printed later?, Harvard Art Museums: Photographs
Harvard Art Museums/Fogg Museum, Gift of Naomi and Walter Rosemblum
Size: 28 x 34 cm (11 x 13 3/8 in.)
https://www.harvardartmuseums.org/collections/object/5199
209 notes
·
View notes
Photo

Profile Head of a Lioness, John Frederick Lewis, 1825, Harvard Art Museums: Prints
Harvard Art Museums/Fogg Museum, Bequest of Grenville L. Winthrop
https://www.harvardartmuseums.org/collections/object/254678
23 notes
·
View notes
Text
Okay, @mikesmoustache tagged me to share 10 characters I fell in love with in 2021, so in no particular order:
William Agar from Quacks

I mean, just look at him, how could I not love him? :D
Thomas Thorne from Ghosts

*cries* i just love him so much-
Basil Underwood from It's Love I'm After
watched this movie on the 27th of december and he just immediately became a new comfort character and the movie one of my favourites. he's a mess <3
Vex from Yonderland

name me one person who doesn't love him. he's a sweetie.
Dan Lewis from Doctor Who

look i already loved him before but after the special... yeah. you know.
The Captain from Ghosts
"pom-pom!" :D
Phileas Fogg from Around The World In 80 Days

It's David Tennant and that's already enough for me to love him. But also it was amazing to see this character brought to life by one of my favourite actors and I think I'm not alone in loving him :)
The Eighth Doctor (+ Charley Pollard) from Doctor Who

I could write a whole essay here about why I love 8, but let's just say that he's utterly amazing and always manages to make me smile <3 Also honourable mention of Charley Pollard, who now has a proud place among my favourite companions!
Withnail & Marwood from Withnail & I

absolute disaster gays. look at them. i love them. and yes they count as one, sshhh
Sam from Attack The Block
It's Jodie. I literally do not need any other reason to love a character of hers <3
There are of course many more characters I fell in love with over the year, but I can hardly just put every character played by the six idiots here xD
Tagging (no pressure): @sunny-lie-melody @x-ladydisdain-x @britomart @walkingcontradiction42 @eddymango
#once again it's visible i just jump from actor to actor and work my way through their filmography until i discover the next one lmao#long post#charlie rambles
14 notes
·
View notes
Photo
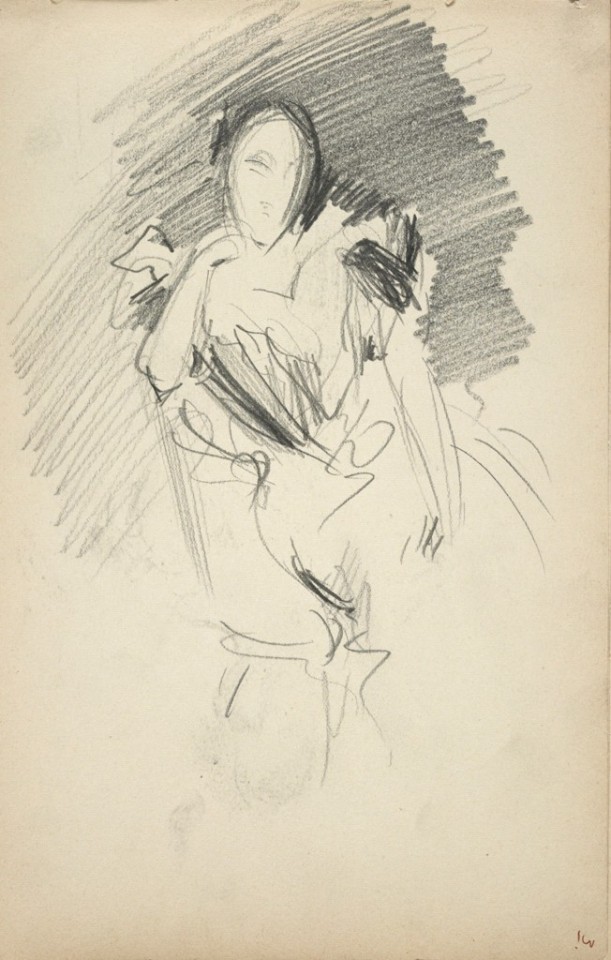
Henrietta Samuel Montagu Franklin (Mrs. Ernest Lewis Franklin) (recto and verso), John Singer Sargent, c. 1898, Harvard Art Museums: Drawings
Harvard Art Museums/Fogg Museum, Gift of Mrs. Francis Ormond
Size: 24 x 15.1 cm (9 7/16 x 5 15/16 in.)
Medium: Graphite on off-white wove paper (recto and verso)
https://www.harvardartmuseums.org/collections/object/197469
26 notes
·
View notes
Note
What if instead of Lewis Carroll (Alice in Wonderland), RT is setting up for a shout-out to JULE VERNE (Journey to the Center of the Earth) instead?
i think with yang at least they’re very much in alice in wonderland territory, but who knows, they might use different inspiration for others who end up in the void. quick wikipedia check does tell me that journey to the center of the earth has three travelers, so it would at least fit ruby, weiss and blake that way.
also damn if that name didn’t just punch me straight back into my childhood and to the phileas fogg adaptation of the story.
25 notes
·
View notes
Photo
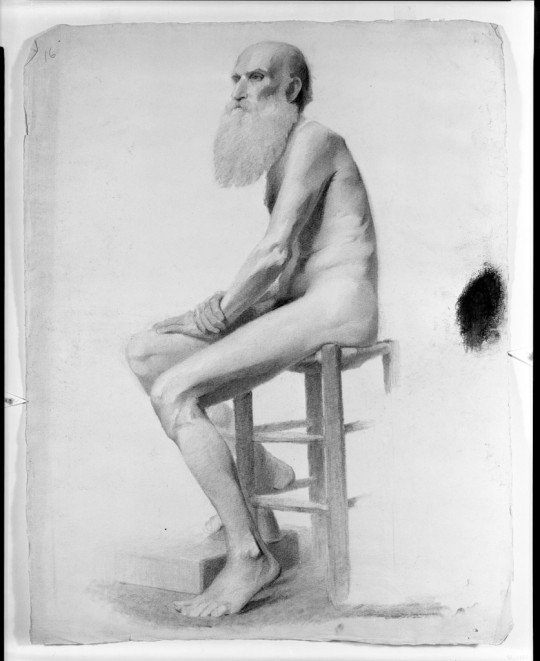
Seated Nude Male Model, Charles Lewis Fox, 19th-20th century, Harvard Art Museums: Drawings
Harvard Art Museums/Fogg Museum, The Melvin R. Seiden Fund, Louise Haskell Daly Fund and Paul J. Sachs Memorial Fund
Size: 64.4 x 50.1 cm (25 3/8 x 19 3/4 in.)
Medium: Charcoal on off-white laid paper
https://www.harvardartmuseums.org/collections/object/309306
2 notes
·
View notes
Text
Shortwood gain bragging rights over Cheltenham Saracens
Hellenic League Division One
Shortwood 3 Cheltenham Saracens 1 Wood came from a goal behind at Meadowbank on Tuesday night to ultimately enjoy a comfortable win over Cheltenham Saracens, writes Jim Cunneen.
Manager Ian Soule was delighted with his side’s performance after a difficult opening period and was even more pleased with the way they adapted to the style he and Lewis Fogg made at the…

View On WordPress
0 notes
Photo

Prodigal Son, Auguste Rodin, 19th century, HAM: Sculpture
Harvard Art Museums/Fogg Museum, Gift of Lewis H. Weinstein, AB '27, JD '30 and Selma Yeslawsky Weinstein, '32
Size: 140 x 104.1 x 65.2 cm (55 1/8 x 41 x 25 11/16 in.)
Medium: Bronze
https://www.harvardartmuseums.org/collections/object/226692
2 notes
·
View notes
Note
Hello! I would like to add my fancures to the Directory! The serie's name is "Kokoro♡Clock Precure" and its themes are steampunk and inventions. We have Maribel Boushizuku/ Cure Dentelle, Carol Fogg/ Cure Jasmin, Chise Kisaki/ Cure Ceylan, Lewis Fogg/ Cure Gear (Lewis is a boy Cure and Carol and Lewis are twins). The mascots are Chapelier (rabbit), Petit Beurre (mouse), Dinah (cat) and Owlga (owl). Thank you and have a nice day! :)
Hey, so it looks like you sent this information to us three times?
Sorry for taking so long, but if you’re not sure that we received it or not, you can always Tumblr IM me. My messages are open for this kind of thing.
- Cure Tidy
3 notes
·
View notes
Last Seen Blogs

kepave
Underneath the Mane..

satanruz
Wattpad🔸: Satanruz

a-chaotic-dumbass
.•~💫Latest brainrot: Jaime Lannister💫~•.

lovelysheree
Skidaddle skidoodle, this blog is full of doodles

zionsafetycollege
Untitled