#Journals on Emergency Medicine
Text
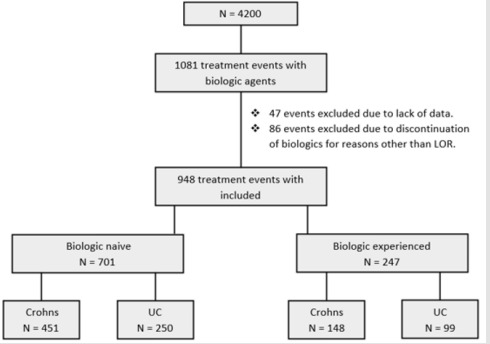
Sustainability of Biologic Therapy is Less in Ulcerative Colitis than Crohn’s Disease Patients, Independent of Prior Biologic Experience
Sustainability of Biologic Therapy is Less in Ulcerative Colitis than Crohn’s Disease Patients, Independent of Prior Biologic Experience in Biomedical Journal of Scientific & Technical Research
https://biomedres.us/fulltexts/BJSTR.MS.ID.006071.php
Background: Treatment of Inflammatory Bowel Disease (IBD) with biologics is effective but loss of response to treatment limits long-term treatment success. Few studies have examined what determines sustainability of biologic treatment. Objective: The aim of our study was to determine factors associated with sustainability of biologic therapy in IBD. Methods: We performed a retrospective study of 4,200 patients in a single healthcare network. Primary outcome was time to biologic treatment discontinuation (due to inadequate treatment response or adverse effects). Results: A total of 948 independent biologic treatment episodes were identified in 712 patients. Mean follow-up was 2.3years (range 0.0028 – 5.00). • Group 1: 701 biologic-naïve treatment episodes were included. 329 patients (47%) were treated with infliximab, 337(48%) with adalimumab and 32(5%) with golimumab. 250 (36%) had UC. Mean time to discontinuation in UC was 2.9 years compared to 3.6 years in CD (p = <0.001). • Group 2: 247 treatment episodes of biologic-experienced patients were included. 83(33%) were treated with infliximab, 57(23%) with adalimumab, 40(16%) with vedolizumab, 26(11%) with golimumab and 41(16.6%) with ustekinumab. 99(40 %) had UC. Mean time to discontinuation in UC was 2.3 years compared to 3.1 years in CD (p = 0.03). Conclusion: Our real-world data indicates sustainability of biologic treatment is less in UC than in CD patients and is not strongly determined by prior biologic exposure. These findings suggest the need for better understanding of the differing mechanisms for loss of biologic response which will assist in sequencing of therapies in the future.
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01
Follow on Blogger :https://biomedres01.blogspot.com/
Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Biomedical Intervention#Journals on Emergency Medicine#Physical Medicine and Rehabilitation#journal of biomedical research and reviews#journal of biomedical sciences research review
0 notes
Text
these are my star trek doctor ocs emtala jcaho (pronounced jay-ko) and ama n'jem
#ama njem is half terran-ghanian and half vulcan#Emergency Medical Treatment and Labor Act and American Medical Association#New England Journal of Medicine#dee s 9
6 notes
·
View notes
Text
JC: The DAShED Study - Diagnosis of Acute Aortic Syndrome in the Emergency Department
Estimated reading time: 8 minutes
Let’s be honest – acute aortic syndrome is the absolute bane of the emergency physician’s existence. A rare, but incredibly dangerous diagnostic needle in a chest pain haystack. Currently, our only really reliable diagnostic test is a CT aorta angiogram, but just how many of these do we need to do to pick up one case of dissection?
In this post, we discuss a…

View On WordPress
0 notes
Text
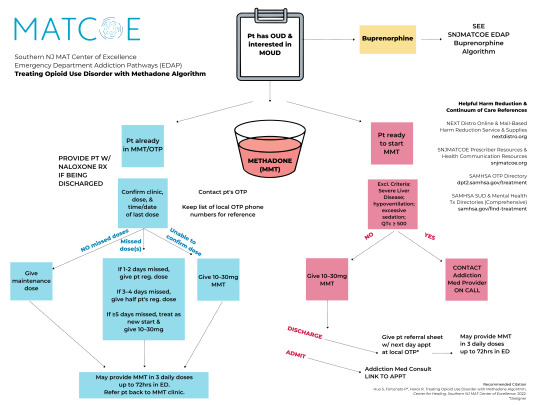
The methadone prescribing algorithm is published as part of the Southern New Jersey Medication for Addiction Treatment Center of Excellence (MATCOE) Emergency Department Addiction Pathways (EDAP) and in the Journal of Emergency Medicine (JEM), March 2023. Learn more here.
Recommended citation:
Huo S, Fortunato P, Haroz R. Treating Opioid Use Disorder with Methadone Algorithm. Southern New Jersey Medication for Addiction Treatment Center of Excellence. 2022.
#Methadone#Medication for Opioid Use Disorder#Medication for Addiction Treatment#MOUD#MAT#Opioid Use Disorder#OUD#Addiction Medicine#Emergency Medicine#Medicine#Southern New Jersey Medication for Addiction Treatment Center of Excellence Emergency Department Addiction Pathways#SNJMATCOE EDAP#Southern New Jersey Medication for Addiction Treatment Center of Excellence#Southern NJ MAT Center of Excellence#SNJMATCOE#Journal of Emergency Medicine#Patricia Fortunato#Personal
0 notes
Text
Hi, everyone.
Yesterday, I shared here a series of posts written by a girl named Nada Bedair on Twitter, where she discussed new information, she learned after watching a documentary.

It was revealed in this documentary that Israel has something called the "Bank of Skins," which is the largest skin bank in the world, specializing in treating burns, skin cancer, and more.
In this documentary, it became clear that most of these skins did not belong to Israeli soldiers but were taken from the bodies of deceased Palestinians, their identities deliberately obscured through disfigurement or lack of proper autopsy.
At the same time, numerous reports emerged from Palestinians, stating that after the arrest of individuals from Gaza and the West Bank, their families were surprised by their return as deceased, with their bodies missing certain body organs!
Simultaneously, an article was published by the head of the Forensic Medicine Institute, claiming that Israel kills and harvests organs from deceased Palestinians without their consent or their families' consent!
Here is the link to the complete post, including the sources:
https://www.tumblr.com/storiesfromgaza/732558400585613312/today-i-learned-about-something-terrible-and-i?source=share
It is crucial that you read this before continuing with this article.

After I shared it yesterday, @chimaeraonwards wrote a comment, attaching a link to a Journal Article | Social Research by anthropologist Nancy Scheper-Hughes titled, "The Body of the Terrorist: Blood Libels, Bio-Piracy, and the Spoils of War at the Israeli Forensic Institute."
In this article, the author describes in detail what happened and how it happened in around 38 pages.
you can read it here:
Scheper-Hughes, N. (2011). The Body of the Terrorist: Blood Libels, Bio-Piracy, and the Spoils of War at the Israeli Forensic Institute. Social Research, 78(3), 849–886. http://www.jstor.org/stable/23347019
Your reading of it won't take much of your time, but it will significantly increase your awareness of things you might not have imagined happening!
If reading it is a challenge, it's worth to mention that yesterday, @chimaeraonwards did an amazing thing.
She wrote a breakdown of some of the content of the 38-page article. Ensure you read it; it's not very long, but it's highly enlightening.
Link: https://www.tumblr.com/chimaeraonwards/732568635164524544/whatever-youre-thinking-about-this-its-actually?source=share
Support her by sharing it because she truly deserves it.
#gaza#palestine#gaza strip#free gaza#free palestine#storiesfromgaza#غزة#فلسطين#genocide#humanitarian crisis
661 notes
·
View notes
Text
We should journal and record what the pandemic hoax was really like...and I mean offline... because I have a feeling this is one the history books and digital world are going to intentionally forget about.
Like remember how they had stores where "for your safety" you were only allowed to buy products they deemed essential. Remember going into a store and sections were roped off and the fucking stores wouldn't let you buy certain things.
I remember going into a dollar store to buy emergency supplies but they were deemed non essential because they were in the camping/outdoor section. I remember that they had employees...regular ass people doing a minimum wage job walking around and harassing customers who were trying to buy anything but food or medicine. Because apparently if you buy food at the store covid wouldn't get you but if you bought a book you were sure to kill yourself and everyone around you. All this during a stage of this "pandemic" where nobody you knew had even heard of anyone who was sick...this was before the jabs came out and people really started "Dying of covid."
You could write a whole chapter about all the times some karen told you to put on a mask and you had to resist the urge to feed them theirs. And remember when they changed the meaning of karen midstream to apply to people who wanted to be left alone and not wear a mask instead of insane entitled people desperate for a sense of power over otherswho make unreasonable demands...like someone who approaches strangers to demand they cover their face so they feel less afraid.
862 notes
·
View notes
Text
“[...] Like other movements within political Islam, the movement [Hamas] reflected a complex local reaction to the harsh realities of occupation, and a response to the disorientated paths offered by secular and socialist Palestinian forces in the past. Those with a more engaged analysis of this situation were well prepared for the Hamas triumph in the 2006 elections, unlike the Israeli, American, and European governments. It is ironic that it was the pundits and orientalists, not to mention Israeli politicians and chiefs of intelligence, who were taken by surprise by the election results more than anyone else. What particularly dumbfounded the great experts on Islam in Israel was the democratic nature of the victory. In their collective reading, fanatical Muslims were meant to be neither democratic nor popular. These same experts displayed a similar misunderstanding of the past. Ever since the rise of political Islam in Iran and in the Arab world, the community of experts in Israel had behaved as if the impossible was unfolding in front of their eyes. [...]
In 2009, Avner Cohen, who served in the Gaza Strip around the time Hamas began to gain power in the late 1980s, and was responsible for religious affairs in the occupied territories, told the Wall Street Journal, “the Hamas, to my great regret, is Israel’s creation.” Cohen explains how Israel helped the charity al-Mujama al-Islamiya (the “Islamic Society”), founded by Sheikh Ahmed Yassin in 1979, to become a powerful political movement, out of which the Hamas movement emerged in 1987. Sheikh Yassin, a crippled, semi-blind Islamic cleric, founded Hamas and was its spiritual leader until his assassination in 2004. He was originally approached by Israel with an offer of help and the promise of a license to expand. The Israelis hoped that, through his charity and educational work, this charismatic leader would counterbalance the power of the secular Fatah in the Gaza Strip and beyond. [...]
In 1993, Hamas became the main opposition to the Oslo Accord. While there was still support for Oslo, it saw a drop in its popularity; however, as Israel began to renege on almost all the pledges it had made during the negotiations, support for Hamas once again received a boost. Particularly important was Israel’s settlement policy and its excessive use of force against the civilian population in the territories. [...]
It also captured the hearts and minds of many Muslims (who make up the majority in the occupied territories) due [to] the failure of secular modernity to find solutions to the daily hardships of life under occupation. [...]
The new Israeli methods of oppression introduced during the Second Intifada—particularly the building of the wall, the roadblocks, and the targeted assassinations—further diminished the support for the Palestinian Authority and increased the popularity and prestige of Hamas. It would be fair to conclude, then, that successive Israeli governments did all they could to leave the Palestinians with no option but to trust, and vote for, the one group prepared to resist an occupation described by the renowned American author Michael Chabon as “the most grievous injustice I have seen in my life.” [...]
The obvious failure of the Palestinian groups and individuals who had come to prominence on the promise of negotiations with Israel clearly made it seem as if there were very few alternatives. In this situation the apparent success of the Islamic militant groups in driving the Israelis out of the Gaza Strip offered some hope. However, there is more to it than this. Hamas is now deeply embedded in Palestinian society thanks to its genuine attempts to alleviate the suffering of ordinary people by providing schooling, medicine, and welfare. No less important, Hamas’s position on the 1948 refugees’ right of return, unlike the PA’s stance, was clear and unambiguous. Hamas openly endorsed this right, while the PA sent out ambiguous messages, including a speech by Abu Mazen in which he rescinded his own right to return to his hometown of Safad. [...]”
—Ten Myths About Israel by Ilan Pappé, Chapter 9: “The Gaza Mythologies”, the section titled “Hamas Is a Terrorist Organization”
282 notes
·
View notes
Text

October 12th
Medical Play, Papa Emeritus III x Reader
Masterlist
Words: 2.5k
Warnings: Medical play; GN!Reader; dom!Reader?; cringey Terzo; subby!Terzo; established relationship; latex kink?; glove kink; hand job; mild praise; anal fingering; taunting; mild degradation; mild humiliation; power kink; mild edging; cum eating; cumswap; reads like an 80s porno; awful medical terminology, I'm sorry to all the doctors and nurses reading this lmao;
Taglist: @sodoswitchimage @enchantedbunny @bitchywitchygardener @thew0man @sodomiser @the-did-i-ask @copias-sewer-rat @gehrmansbignaturals
🔞 MDNI 🔞

The graveyard shift was always the worst - or rather, the slowest. As most of the Siblings were asleep in the dead of the night, you had free roam of the medical centre of the Ministry. Not that there was ever much to see given that it was hardly decorated and filled to the brim with medicine and multiple medical journals, all of which you’d perused on your off or slow hours.
Thankfully, your job was always made easier by the fact that no one in the Ministry was stupid enough to get themselves into a lot of trouble. Even during the day, the worst injury you’d seen was someone’s ritual or blood play wounds get infected, but thankfully it was easy enough to sort out. It was the most difficult thing, becoming a doctor and going through university - even getting a job within the Ministry itself was a difficult task. The job itself though - paid to read books mostly.
Though, it was different that night. Your socked feet were up on your desk and a book was in your lap. You were, of course, reading what your friends liked to call your “dirty girl books”, when there was a gentle knock at the door. “Come in!” You called. Immediately you brought your feet off the desk and put your bookmark in the book, hiding it from the view of your guest. You still didn’t want to appear unprofessional, even though there was no one around… well, almost no one.
The door opened to reveal a smaller man, black hair and wrinkles. You recognised him instantly. “Good morning, Papa.” You said, standing to your feet out of respect.
“Ah, hello, doctor. I hope I am not disturbing you while you are busy?” Terzo stood there in the doorway uncharacteristically awkward in his demeanour and make up chipping from his face. He looked tired.
You looked at the clock: four o’clock. It was so early. “I always have time for you, Papa. How can I help you?”
“Ah, it is a little embarrassing, doctor.”
“Whatever it is I’m here to help, judgment-free.”
This was the moment you’d been waiting for. The thing is - you weren’t Terzo’s personal physician. Given the nature of their job and the importance of their status, each of the Papas had their own personal physicians at their beck and call all times of the day and night. You weren’t part of that club, rather, dealing with the rest of the Ministry including the Ghouls and the Clergy. You may not have been Terzo’s physician, but you were his partner… so to speak. This whole arrangement had been set up and pre-decided weeks ago, and when he had time, he’d drop in to see you with some “medical emergency” and you would be the doctor to “treat him”. You would pretend not to know each other which was the most crucial part of the whole scene. So now you were just waiting for Terzo to say his next line, not that you knew what his next line was.
“Well you see, I am an old man. And my, how do you say? My dick is broken.”
This fucking guy.
“Okay, in what way?”
“It doesn’t stand for very long. It grows tired very quickly, like me. Or my fratello.”
Please don’t compare your penis to your brothers.
“R-right.” You blinked at him a few times, not quite expecting him to be so forthcoming with his “issue” - or even quite so chaotic. “Please come and take a seat on the bench for me.” He did as you instructed. “Would you mind unbuttoning your shirt, Papa?”
“Ah, doctor, that is the other thing. My fingers are tired today, too. I am afraid they can’t unbutton anything.”
Of course they can’t.
He looked at you and gave you the biggest shit-eating grin, clearly eating up his role. Despite knowing Terzo as intimately as you did for a number of years, he still managed to find ways to fluster you.
You moved forward, trying your best not to smile and keep it “professional”, but the excitement within him was simply radiating off of him and infecting you. He was, for lack of a better term, buzzing with it. Your fingers carefully began to unbutton his white shirt and avoiding his gaze, but you could feel it on you. His mischievous eyes studying you and your expression so intently you were sure it would leave a mark.
Once his incredibly hairy chest was completely exposed to you, you took the stethoscope from around your neck and set yourself up to use it. “This may be a little cold.” You warned before placing the bell over his heart. Of course, this wasn’t a real check up, so it didn’t matter what you heard. In fact, you were only doing this for his benefit because you knew he’d want it.
“Can you hear that, doctor?” He asked.
“There’s nothing unusual.”
“But my heart, you should hear that it beats only for you.”
This. Fucking. Guy.
It took everything in you not to blush or react to his words in any way. “Okay, I think we should do a few tests just to make sure everything’s okay. Would you mind removing your pants, Papa?”
You took a step back and allowed Terzo to stand from the bench and do as you’d asked. You looked away to feign privacy, despite the fact that you’d been up close and personal with that part of his body for a long while. But out the corner of your eye, you noticed that the little shit had decided to forgo underwear. How you were surprised was a mystery unto itself.
“You know, doctor, usually I buy ladies dinner before I let them undress me in their offices.” He teased.
“Usually ladies don’t examine you for erectile dysfunction.” You taunted back. “Are you ready, Papa?”
“Of course, doctor. I await your professional opinion.” He plonked himself back up on the bed and leant back confidently, completely exposing himself to you. He was enjoying this game a little too much for your liking. You began prepping your hands, first sanitizing them then putting latex gloves on to keep up appearances. When you moved back over to him, you noticed that his mismatched eyes were heavily trained on you, only moving when you did and fixating on your gloved hands. Time to bullshit your way through this. “To make sure you can maintain a healthy erection, we need to give you one first. Is this normally something you have a problem with?”
“Not at all. Usually my partner is able to get me up just by looking at me.”
You nodded. “So you won’t need any help from me today, then?”
“On the contrary, doctor. My partner is not here, and so I am having trouble. Please take care of me.”
He gave you the best doe eyes he could muster knowing that it would work on you because it usually did. And so, you nodded, and poured some of the office’s lubricant onto your hand. “This will be cold.” You warned him.
As soon as your lubed hand made contact he hissed and jumped, perhaps making more of a show of it than he ought to. Your hand began to work away at his flaccid length, which was filling up with blood a lot quicker than you anticipated. With each tight stroke of your hand, Terzo’s hips bucked slightly. He wasn’t quite ready or sensitive enough for it to feel mind-numbingly good, but the little breaths and whimpers he was releasing was proof enough that it was working. One of his own gloved hands came up to your arm and gripped onto it, trying to keep himself grounded. The other hand grasped onto the bench with as much force as he could.
You tightened your grip and began focusing entirely on the head of his cock, making sure he was feeling as much pleasure as possible. The feeling of the lubed latex on his head had his mind reeling. His eyes were tightly shut, his bottom lip had been taken into his mouth and trapped between his teeth. He was trying so hard to keep up the pretense but he was obviously feeling good. You decided to be a bitch. “Tell me, Papa, what do you usually do to keep the erection?”
“What?” He asked, opening his eyes and coming to his senses.
“Well, this is a new problem, isn’t it? What usually works? What usually feels good?”
Terzo, whom you had never seen so flustered before, gulped and took in a sharp inhale before continuing. “M-my partner usually uses their mouth.”
“Where?”
“What?”
“Where does their mouth go?”
“M-my cock and sometimes my a-asshole.”
You moved your other hand to his taint and then to the rim of his hole. “Here?”
“Yes! Merda! There!”
Then, all of a sudden, you removed all of your hands and took a step back. “You seem to be healthy, Papa. I think maybe you’re just stressed.”
His eyes were wide and he couldn’t quite believe you’d done that. “What?”
“Lack of sleep can also be a cause of dysfunction. Do you get enough sleep?”
“Yes. Doctor, I- I am confused.”
“What with?”
“Well, I… you… stopped.”
“Of course, Papa. You needed help maintaining an erection, we’ve since discovered that you don’t struggle with that regularly, and you’re certainly not now.”
“You can’t just leave me like this.” He gestured to his now angrily erect cock before muttering something in Italian, clearly irritated by you.
“Maybe if you were to ask nicely, I might help you out.”
Terzo hesitated for a second, clearly wanting to say something but not wanting to either be so desperate that he begs for it, but also being to embarrassed to say anything. He was perhaps the filthiest person you knew, never shy or bashful, but apparently when his partner had the upper hand he was a total mess.
“Per favore.”
“Not good enough. Try again.”
“Will you… help me out?”
“Sure, what with?”
“Porca puttana! Make me cum… please, Doctor.”
He almost forgot himself.
You stood and sauntered back over to him applying more lube to your gloved hand as you passed that shelf. “Good boy.” You told him with a teasing smile, wrapping his cock back up in your hand and continuing exactly where you left off. “Nothing wrong with you now, is there? You’re keeping it up well enough, aren’t you?”
The same hand that was gripping onto the bed had moved up onto your shoulder, a gorilla grip on it. His eyes were open but focused on the wall, glazed over a little in the sheer pleasure your hand was providing. Your other hand went straight back to the rim and began rubbing over it again. His noises got louder when you did, hips having a mind of their own. The position wasn’t great so you got him to sit back, keeping him width-ways on the bench with his cheeks on the edge and his feet propped up and legs spread. You cursed your boss for giving you the wrong chair to use for today, what you would have killed to use the gynecology chair with the stirrups. It would have humiliated him so much to be so exposed. He would have loved it. Though he looked like such a whore in this position, you thought perhaps this was more humiliating.
With more lube on your hands, one went back to his head, and the other started pushing inside his hole. His mouth dropped open in a perfect ‘O’ and his brow furrowed, the pleasure almost overwhelming him. “We do have to make sure all parts of you are working correctly, hm? Especially this nice little button in here.”
“Cazzo!”
Only your pinkie was inside him at the moment. You didn’t want to hurt him and as he hadn’t pre-stretched himself out, you thought it was best to take your time. You wiggled it around a little, trying to make his hole fit two of your better, and kept at it until he was lose enough. Eventually, your index and middle fingers were able to fit inside him, and so you went in search of that button you mentioned. “Touch your cock for me.” You instructed. Like the obedient whore he was today, he did as you asked, wrapping his own hand around the head and moving quickly. “Ah-ah.” You scolded. “Slow down.”
“But-”
“Slow!”
His hand gradually put the breaks on, dropping to an almost torturous level. You could see how much it pained him. Given the fluttering of his hole around your two fingers, you could tell he was already too close. He was too overwhelmed. He needed that sweet release that you were refusing to give him. Why? Why wouldn’t you just make him cum? Why would you drag it out as much as you did? He couldn’t fathom it. But he was so desperate to finish he couldn’t ask you to stop.
This was a completely different man in front of you. The head of the Satanic Church was riding your fingers in your office as if he didn’t hold all of the power. Because right now he didn’t. You did. In his desperate need to cum, he was obeying your orders down to the letter. He was whining and writhing for you and only you. No one else got to see him like this: his entire body on fire and chasing a release he’d practically been begging for since he entered the medical ward, drool dripping from the corner of his mouth where it had opened so wide, and loud moans were spilling out with it. His pants completely removed and his white shirt unbuttoned completely. He was positively sinful right now - a proper Babylonian whore giving himself to another for his own pleasure. And oh how he sang for you when you reached that spot. How he stopped breathing when you finally hit it. How expletives poured from his lips to cope with the devastating bliss your fingers were giving him. Choruses of “yes!” and “right there!” and “don’t stop!” providing him comfort while you had your way with him. His own hand matched yours and as you got faster, so did he. He was so close. He could almost taste the sweet release that was on its way to him.
It was when your hands came up to play with his balls he finally tipped over the edge. Cum spurted from his cock and pooled over his hairy stomach, and even reaching up his chest in the intensity of the orgasm he was experiencing. His toes curled and his body seized up. You were, the whole time, talking him through it. “That’s it,” you told him, “give it all to me, Papa. Give me everything. Such a good boy.”
When you were sure he was fine, you gently removed yourself from inside him and bent forward, your tongue running through his spend and lapping it up into your mouth, keeping it there. You looked up at him and saw his eyes were ablaze with something. More lust? Frustration that you were doing something so sexy and he was too tired to do anything about it? You weren’t entirely sure. But the moan he released when you kissed him, swapping his cum from your mouth to his was enough to tell you all was forgiven… at least for now.

Previous Day ⛧ Next Day
#mel writes#kinktober#kinktober 2023#ghost kinktober#the band ghost#ghost#ghost bc#ghost band#ghost the band#papa emeritus#papa emeritus iii#papa terzo#terzo#smut#x reader#x reader smut#papa emeritus x reader#papa emeritus x reader smut#papa emeritus iii x reader#papa emeritus iii x reader smut#papa terzo x reader#papa terzo x reader smut#terzo x reader#terzo x reader smut#terzo emeritus#terzo my beloved#ghost terzo
268 notes
·
View notes
Note
Could I request brothers of Obey Me with an s/o who's a medical expert?
Obey me Brothers + medical expert s/o
Lucifer
Finds it interesting.
He doesn’t know much about human anatomy or medicine, so it’s always interesting when someone knows more about a topic than he does.
Really has no interest in the physicality of humans or healing. Just interested in their knowledge and hobby.
Provides them with as many resources as possible if they wish to learn demon medicine as well. But only if they want to.
Mammon
Probably says a lot about him that he finds it so hot….
Hearing them talk about medicine, and take authority in an emergency, gets his blood going.
He has no idea what they are talking about, as he’s pretty think with anything biology or health related, but it sounds impressive.
Makes jokes about wanting to play doctor, but gets too flustered & embarrassed if they take him up on it to follow through.
Levi
Finds it interesting, but only for fact checking games or his otome fanfic needs.
He got really into medical information when Hataraku Saibō came out. However he quickly lost interest when he had to actually learn stuff and look at pictures of blood.
Levi has a slight Hemophobia complex.
Will go ask them things like “how quickly does the human body drain of blood?” “what’s the difference between a laceration and a hematoma?” “could someone live if they were stabbed in the stomach 13 times?” For literary purposes only.
Satan
Of course loves anything to do with knowledge, and the amount of reading required to become a medical expert is just a bonus.
Satan also has an interest in medicine and medical information due to his love of mystery drama, which are his favorite type.
Forensic knowledge has a great crossover. So he spends a lot of time speculating with s/o on the cause of death or suspects in a book before it reaches the end.
Finds a lot of obscure medical books & journals to share with them, should they cross his path.
Asmo
Says he’s interested, but only to play doctor.
A lot of it really goes over his head as Asmo is only interested in figures. Not literal anatomy.
He does like to listen to them though, as they always get so passionate when they talk about some medical marvel of obscure fact. He’s always found passion to be a person’s sexiest quality.
Dresses up like a nurse a lot to surprise them. Thinks it’s helpful.
Beel
A lot of it is too technical for Beel too, but he tries to pay more attention than Asmo.
He is actually really interested in anatomy. Particularly as it relates to kinesis and physicality.
He asks a lot of questions on how to move his body better to improve his results. Or avoid injury.
Injuries do happen though, as it’s inevitable with sports or the high intensity work outs, he’s doing. Goes to s/o to have them bandage him up and take care of him. They always have to ask if he’s running a fever as well with how much he blushes.
Belphie
Belphie is a bit of the medical expert too. He had a lot of time to read when he was locked up in that attic, and anatomy was actually always an interest of his before s/o.
He plays dumb though and acts like he doesn’t understand things, so they’ll reteach him. Mostly just to hear them talk.
He also plays sick a lot so they’ll take care of him. Not necessarily a Munchausen, just needy.
It usually works. However there are sometimes when the treatments get a little….intense, and more than he bargained for. At least they haven’t tried surgery on him yet.
#;ask and ye shall receive (request answers)#obey me#obey me headcanons#obey me hc#headcanons#obey me lucifer#obey me mammon#obey me leviathan#obey me levi#obey me satan#obey me asmo#obey me asmodeus#obey me beel#obey me beelzebub#obey me belphie#lucifer#mammon#leviathan#satan#asmodeous#beel#belphie#obey me x reader
167 notes
·
View notes
Text
From heart disease to IUDs: How doctors dismiss women’s pain
Several studies support the claim that gender bias in medicine routinely leads to a denial of pain relief for female patients for a range of health conditions
One woman was told she was being “dramatic” when she pleaded for a brain scan after suffering months of headaches and pounding in her ears. It turned out she had a brain tumor. Another was ignored as she cried out in pain during a 33-hour labor. She was supposed to be getting pain medication through her epidural, but it had fallen out. Dozens of women complained of torturous pain as their vaginal walls were punctured during an egg retrieval process. They were told their pain was normal, but, in actuality, they were getting saline instead of anesthesia. These are just some of the stories of women who say their pain and suffering has been dismissed or misdiagnosed by doctors. Although these are anecdotal reports, a number of studies support the claim that women in pain often are not taken as seriously as men.
This year, the Journal of the American Heart Association reported that women who visited emergency departments with chest pain waited 29 percent longer than men to be evaluated for possible heart attacks. An analysis of 981 emergency room visits showed that women with acute abdominal pain were up to 25 percent less likely than their male counterparts to be treated with powerful opioid painkillers. Another study showed that middle-aged women with chest pain and other symptoms of heart disease were twice as likely to be diagnosed with a mental illness compared with men who had the same symptoms. “I was told I knew too much, that I was working too hard, that I was stressed out, that I was anxious,” said Ilene Ruhoy, a 53-year-old neurologist from Seattle, who had head pain and pounding in her ears. Despite having a medical degree, Ruhoy said she struggled to get doctors to order a brain scan. By the time she got it in 2015, a tennis ball-sized tumor was pushing her brain to one side. She needed surgery, but first, she rushed home, hugged her 11-year-old daughter and wrote her a letter to tell her goodbye.
Ruhoy did not die on the operating table, but her tumor had grown so large it could not be entirely removed. Now, she has several smaller tumors that require radiation treatment. She said many of her female patients have had experiences similar to hers. “They’re not validated with regards to their concerns; they’re gaslit; they’re not understood,” she said. “They feel like no one is listening to them.”
Doubts about women’s pain can affect treatment for a wide range of health issues, including heart problems, stroke, reproductive health, chronic illnesses, adolescent pain and physical pain, among other things, studies show. Research also suggests that women are more sensitive to pain than men and are more likely to express it, so their pain is often seen as an overreaction rather than a reality, said Roger Fillingim, director of the Pain Research and Intervention Center of Excellence at the University of Florida. Fillingim, who co-wrote a review article on sex differences in pain, said there are many possible explanations, including hormones, genetics and even social factors such as gender roles. Regardless, he said, “you treat the pain that the patient has, not the pain that you think the patient should have.”
Women say reproductive health complaints are commonly ignored
Women often cite pain bias around areas of reproductive health, including endometriosis, labor pain and insertion of an intrauterine device, or IUD. When Molly Hill made an appointment at a Connecticut clinic in 2017 to get an IUD, she said she was warned it would be uncomfortable, but she was not prepared for “horrific” pain. Hill, now 27 and living in San Francisco, recalled that during the procedure, she began crying in pain and shouted at the doctor to stop. “We’re almost done,” she said the doctor told her and continued the procedure. “It was full-body, electrifying, knife-stabbing pain,” she said. After it was done, she said she lay sobbing on the table in physical and emotional pain. “It felt violating, too, to have that pain that deep in your core where you feel the most vulnerable.”
Studies consistently show that women who have not experienced vaginal birth have much higher pain during IUD insertion compared with women who have given birth. A Swedish study found that among 224 women who had not given birth, 89 percent reported moderate or severe pain. One in six of the women said the pain was severe. Although numbing agents and local anesthetics are available, they are rarely used.
In some cases, women have sued physicians for ignoring their pain. Dozens of women sued Yale University claiming that during an egg harvesting procedure at its infertility clinic, they were supposed to be receiving the powerful painkiller fentanyl. But some women were getting only diluted pain medication or none at all, according to lawsuits filed in the state Superior Court in Connecticut. Later, the clinic discovered a nurse had been stealing vials of fentanyl and replacing the painkiller with saline solution. The nurse pleaded guilty last year and was sentenced for tampering with the drugs. One of the plaintiffs, Laura Czar, wrote about her experience for Elle magazine, describing it as “a horrible, gut-wrenching pain,” and told a doctor at the time, “I can feel everything you’re doing.” Despite her protests, the doctor continued. Yale said in a statement that it “deeply regrets” the women’s distress and has “reviewed its procedures and made changes to further oversight of pain control and controlled substances.”
Racial disparities in pain management
For Sharee Turpin, the pain of sickle-cell disease sometimes feels like tiny knives slicing her open. Sickle cell disease is an inherited blood disorder that can cause suffering so severe, its attacks are called “pain crises.” But when Turpin, who is Black, experiences a pain crisis, the 34-year-old does not rush to the ER in Rochester, N.Y. Instead, she combs her hair, mists some perfume and slips on her “Sunday best” in hopes that the doctors and nurses won’t peg her as a drug seeker, she said. Sometimes, Turpin gets a care team that understands her pain. Other times, she is treated as a bother. “I’ve even been told ‘shut up’ by a nurse because I was screaming too loud while I was in pain,” she said.
Abundant research shows racial bias in pain treatment. A 2016 study found half of white medical students and residents held at least one false belief about biological differences between Blacks and Whites, and were more likely to underestimate Black patients’ pain. “The management of pain is one of the largest disparities that we see between Black people and White people in the American health-care system,” said Tina Sacks, an associate professor at the University of California at Berkeley and author of “Invisible Visits: Black Middle-Class Women in the American Healthcare System.”
Labeling women “hysterical” or blaming psychological causes
Research shows men in chronic pain tend to be regarded as “stoic” while women are more likely to be considered “emotional” and “hysterical” and accused of “fabricating the pain.” Carol Klay, a 68-year-old from Tampa, had endured years of chronic pain from arthritis, degenerative disk disease and spinal stenosis. During a hospital stay last year, her doctor noted in her medical record that she was crying “hysterically.” Klay said she was crying because she was unable to sit, stand or walk without agony, and the doctor had removed morphine from her cocktail of pain medications. She wonders whether the doctor “would have called me hysterical if I was a man,” she said. Tampa General Hospital said it could not discuss specific patients, but stated: “Patient treatment plans, including medication orders to reduce pain, are prescribed by multi-disciplinary clinical teams.” Research shows women’s physical pain is also often attributed to psychological causes.
Jan Maderios, a 72-year-old Air Force veteran from Chipley, Fla., said the trauma of having pain dismissed by doctors has stayed with her for years. She saw about a dozen doctors in the early 1970s for pelvic pain. When clinicians could not identify the cause of her pain, she was referred to a psychiatrist.
“You start to doubt yourself after so many medical experts tell you there’s nothing wrong with you,” she said. After a hysterectomy in 1976, Maderios learned that fibroid tumors in her uterus had been the source of her pain. She said learning her pain was real — and physical — “made all the difference in the world.”
Why women’s pain complaints often aren’t taken seriously
During a 33-hour labor with her first child in 2011, Anushay Hossain, 42, of D.C., opted for epidural pain relief but said she still felt it all — every contraction, every cramp and every dismissal of her pain by her medical team. The doctor reassured her that she was getting the maximum dosage of pain medication.
In fact, she wasn’t getting any at all. She said her epidural had slipped out. By the time the error was caught, she was shaking uncontrollably and in need of an emergency Caesarean section, she said. “There’s a pain gap, but there’s also a credibility gap,” said Hossain, author of “The Pain Gap: How Sexism and Racism in Healthcare Kill Women.” “Women are not believed about their bodies —period.”
This pain gap may stem, in part, from the fact that women have historically been excluded from medical research. It wasn’t until 2016 that the National Institutes of Health (NIH) required sex to be considered as a biological variable in most studies it funded. “We’re making progress,” said David Thomas, special adviser to the director of NIH’s Office of Research on Women’s Health. “But we do have a long way to go because there’s this whole institutional approach to doing research — pain and beyond — where it tends to be male-focused.”
Nearly 95 percent of U.S. medical school students said instruction on sex and gender differences in medicine should be included in curriculums, according to a 2015 survey. But only 43 percent said their curriculum had helped them understand those differences and only 34.5 percent said they felt prepared to manage them in a health-care setting.
“It is changing, but it’s changing very slowly,” said Janice Werbinski, immediate past president of the American Medical Women’s Association and chair of the mentorship committee of the association’s Sex and Gender Health Collaborative.
How women can advocate for better pain care
It took decades to solve the mystery of Maureen Woods’s chronic pain. Woods, 64, of Myersville, Md., started having joint pain in her teens and, over the years, told dozens of doctors her pain was “debilitating,” she said. Some told her it was all in her head. In 2017, she was diagnosed with hypermobile Ehlers-Danlos syndrome, a connective tissue disorder often causing loose joints, dislocations and chronic pain. She said women who are not being heard should keep advocating for themselves. “You have to go with your gut — something is wrong and I need to find a doctor who can figure it out,” she said. Marjorie Jenkins, dean of the University of South Carolina School of Medicine Greenville, urged women against feeling pressured to accept an “everything is normal” non-diagnosis. “If your provider does not appear to be listening to you or believing what you’re saying, then you need a new provider,” Jenkins said. “You are the client, you are the customer and you are the owner of your health.”
Women can also take a family member, friend or other support person who can corroborate their stories, said Alyson McGregor, an emergency medicine professor at the University of South Carolina School of Medicine Greenville and author of the book “Sex Matters: How Male-Centric Medicine Endangers Women’s Health and What We Can Do About It.” Particularly in emergency departments, she said, there can be an inherent bias. “There’s this assumption that women are emotional and they’re anxious and that that’s the main issue,” she said.
534 notes
·
View notes
Text
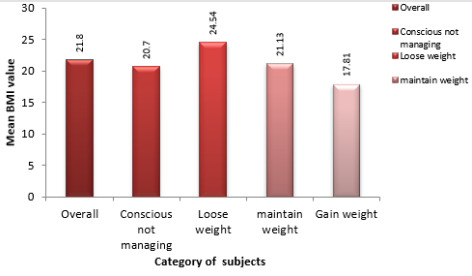
Assessment of Body Composition of Adult Females among Weight Managing and not Managing Groups
Assessment of Body Composition of Adult Females among Weight Managing and not Managing Groups in Biomedical Journal of Scientific & Technical Research
https://biomedres.us/fulltexts/BJSTR.MS.ID.006070.php
One exquisite component that marks the personality of an individual is his or her body weight. Accordingly there is a body image perception in the mind of an individual. According to the body image perception, about oneself one frames in his or her mind, the individual follows specific exercise and dietary modifications for weight management. Weight management may involve loosing weight, maintaining weight, or a desire to gain weight. Targets for managing weight may involve loosing weight, maintaining weight, or gaining weight. An individual’s target for weight management may be further assessed and justified by body composition analysis. Moreover body composition analysis helps to assess the nutritional status of an individual. The present research study was a cross sectional study conducted to assess the body composition of females 18-30 years, 147 in number with reference to Body mass Index (BMI), fat mass per cent, fat free mass per cent and total body water per cent. Also a comparison of the above parameters was done among different groups of subjects namely conscious for weight but not managing weight (CNM), making attempts to loose weight (group I), making attempts to maintain weight (group II) and making attempts to gain weight (group III). An ANNOVA test was conducted to assess the difference in these parameters both within and between groups. The results of the study revealed that the difference in BMI, fat mass per cent, fat free mass per cent was highly significant both within and between subjects of various groups, while the difference in body water per cent was found to be significant both within and between subjects of various groups. Besides this the fat mass per cent values were found to be highest in subjects of group I (loose weight), while the values were found to be lowest in subjects of group III (gain weight). The fat free mass per cent values were highest in subjects of group III (gain weight) while the values were found to be lowest among subjects of group I (loose weight). Body water is a part of fat free mass. This was confirmed since subjects in group III (gain weight) had highest quantity of total body water per cent. With reference to BMI, majority of the subjects in group I (Loose weight) fell in the Overweight or Obese category, while majority of the subjects (66.66%) in group III (gain weight) fell into the category of being Underweight. Majority of the subjects in the conscious not managing category (48.48%) and 73.08% subjects in group II (maintain weight) were classified as Normal. The assessment results for body composition parameters justify the weight management targets by subjects and confirm the appropriate body image perception in the individuals also.
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01
Follow on Blogger :https://biomedres01.blogspot.com/
Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Medical Microbiology#Journals on Emergency Medicine#Physical Medicine and Rehabilitation#journal of biomedical sciences research review#journal of biomedical research and reviews
0 notes
Text
Alright whump writers. Here’s a little something based on personal experience.
Whumpee with a hidden medical condition/disability
This is based on myself as someone with a heart condition and symptoms that I often don’t recognize until too late. Imagine a whumpee:
Forgetting to bring medicine on a trip and trying to hide symptoms
Stopping more often than others on missions to steady themself
Not telling the group about the condition to avoid concern
Disappearing for a few days without a word because they had to spend a few days in the hospital after a scare
Experiencing the beginnings of a cardiac episode but not saying anything
Getting worked up in an argument and having to leave so they don’t hurt themself
Confiding in one member of the group and having them promise to keep it secret
Passing out during an important mission
Fatigued from being put on new medication
Keeping a hidden medical journal with resting heart rate (RHR) and peaks for the week
Worrying about something unexpected causing an episode
Being kidnapped and going without medicine days/weeks
Being given placebos by an enemy and having a heart attack because of them
And imagine their caretaker:
Analyzing every model of defibrillator in case of an episode
Getting CPR certified
Watching them sleep after a medical scare
Constantly checking that they took their medicine/have their prescriptions filled
Panicking the first time they go into cardiac arrest
Losing sleep trying to find them, knowing they’re kidnapped without medicine
Booking/taking them to doctor’s appointments
Becoming their emergency contact
Getting them a medical ID/dog tag with their condition listed
Studying all warning signs connected to their condition and similar conditions
Traveling hours away to bring them their medicine
Treating them like their made of glass after they’ve had an episode
I love medical whump and I should write something with loads of it!!!
#whump#fainting#passing out#medical whump#hospital whump#hidden condition#hidden disability#heart condition#caretaker#disabled whumpee#hidden medical condition#medical condition#cpr#kidnapping#fatigue
226 notes
·
View notes
Text
The Annual ILCOR Update - what's new in adult life support
Estimated reading time: 6 minutes
The International Liaison Committee on Resuscitation (ILCOR) is the umbrella organisation for national resuscitation councils and federations around the world (including the American Heart Association. Australian and New Zealand Committee on Resuscitation, the European Resuscitation Council and groups in Canada, India, Asia, and Southern Africa).
Every year…

View On WordPress
1 note
·
View note
Text
As reported in the journal Science Advances, the findings create a foundation for a new area of investigation, fueled by the timely impact of environmental factors on human biology.
“Parkinson’s disease has been called the fastest growing neurological disorder in the world,” says principal investigator Andrew West, professor in the pharmacology and cancer biology department at Duke University School of Medicine. “Numerous lines of data suggest environmental factors might play a prominent role in Parkinson’s disease, but such factors have for the most part not been identified.”
Improperly disposed plastics have been shown to break into very small pieces and accumulate in water and food supplies, and were found in the blood of most adults in a recent study.
“Our study suggests that the emergence of micro and nanoplastics in the environment might represent a new toxin challenge with respect to Parkinson’s disease risk and progression,” West says. “This is especially concerning given the predicted increase in concentrations of these contaminants in our water and food supplies.”
Continue Reading.
58 notes
·
View notes
Text
Universities secretly sold their students to online casinos

End-stage capitalism’s defining characteristic is making money rather than making things. Think of how Jack Welch destroyed GE by transforming it from a manufacturing company to a financial engineering shop:
https://the.ink/p/like-capitalism-itself-business-journalism
Hospitals are invoice-generating factories with a sideline in medicine. The electronic health record only incidentally records your health. Its primary purpose is to record your billing-codes:
https://www.beckershospitalreview.com/ehrs/physicians-spending-nearly-2-hours-a-day-on-ehr-tasks-outside-work.html
And universities? Ugh. Most universities now have more administrators than faculty:
https://www.jamesgmartin.center/2022/08/administrative-bloat-harms-teaching-and-learning/
Much of that “administration” comes down to begging alums for money to funnel into vast endowments, but heaven forfend those endowments would be used to cover payroll and other essentials, even in a pandemic emergency:
https://www.forbes.com/sites/reneemorad/2020/04/21/harvard-under-fire-for-accepting-nearly-9-million-in-coronavirus-relief-funds/
Nor are endowment funds available to pay the education workers who actually teach students, but can’t afford the rent, food, or family:
https://www.capradio.org/articles/2022/11/14/nearly-50000-university-of-california-graduate-student-employees-launch-open-ended-strike/
The point of the endowment is to increase the size of the endowment — not to improve educational outcomes or research. That’s why Harvard is “A hedge fund that has a university”:
https://www.wsj.com/articles/a-hedge-fund-that-has-a-university-1510615228
This is the overwhelming logic of capital: capital exists to increase capital, and the underlying mechanism for that increase is irrelevant. This was the reasoning behind the surreal bid to sell the .ORG nonprofit registry to a secretive hedge-fund.
The point of the .ORG registry is to host domain records for nonprofits; incidentally, this throws off some extra money that is turned into grants for public interest projects. The board decided to sell off .ORG so it could make more of these grants, despite the fact that this would compromise the mission of hosting .ORG domain records:
https://www.eff.org/press/releases/org-domain-registry-sale-ethos-capital-rejected-stunning-victory-public-interest
Likewise, this was the reasoning of the Mountain Equipment Co-Op board when they decided to sell off the member-owned co-op (“the most trusted brand in Canada”) to a US private equity fund without consulting the members:
https://pluralistic.net/2020/09/16/spike-lee-joint/#casse-le-mec
The expand-capital-at-all-costs mindset is a virulent species of brain worms. It’s the basis for surreal movements like effective altruism, which encourages people who want to do good for the world to sell out to the most toxic industries on Earth, amass gigantic fortunes, and then, upon their death, donate them to causes that in some way remediate the harms they themselves wreaked:
https://en.wikipedia.org/wiki/Earning_to_give
In his new book Survival of the Richest, Douglas Rushkoff calls this “The Mindset” — “I need to make vast amounts of money, no matter what the consequences, or I will not be able to afford to insulate myself from the consequences of how I made all that money”:
https://pluralistic.net/2022/09/13/collapse-porn/#collapse-porn
Once you let people with The Mindset anywhere near your institution, they will take it over and turn it into a paperclip-maximizing killing machine, one that abandons and then betrays its mission to increase its profits, eventually killing its host. Anything that can’t go on forever will eventually stop:
https://doctorow.medium.com/anything-that-cant-go-on-forever-will-eventually-stop-110ba9711133
That’s what’s happened to higher ed. It’s not just the payroll full of starving adjuncts, facilities workers, etc. It’s not just the way that universities join forces with textbook monopolists to gouge their students:
https://pluralistic.net/2021/10/07/markets-in-everything/#textbook-abuses
Beyond academics having to rely on food-stamps, students going into lifetime debt to enrich predatory textbook monopolies, and the other horrors of financialized higher ed, there’s the special evil of college sports.
Like all finance-bro motivated reasoning, college sports are sold as a way to do well by doing good: “Look! We’re giving poor people a chance at a great education based on their physical prowess, and we’re racking up tons of money for the university!”
But — like all finance schemes — college sports is a self-licking ice-cream cone that destroys the lives of the people who generate value for it, even as it devours its host institution from within.
Did you know that until very recently, college athletes weren’t allowed to make a penny from their labor?
https://www.scotusblog.com/2021/06/in-unanimous-ruling-court-agrees-with-athletes-that-ncaa-violated-antitrust-laws/
Did you know that those same athletes experience lifelong brain injuries?
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2791303
Did you know that college sports are a cesspit of long-term, officially tolerated sexual abuse?
https://www.theguardian.com/sport/2021/nov/30/ohio-state-michigan-doctors-sexual-abuse-college-football
Did you know that the highest paid public employee in many states is a football coach at a state college?
https://www.profootballnetwork.com/highest-paid-college-football-coaches-2022/
Did you know that college coaches conspired with the rich parents to steal sport-related admission slots from poor kids and give them to mediocre winners of the orifice-lottery?
https://en.wikipedia.org/wiki/Varsity_Blues_scandal
In many universities — whether public or private — the sports program effectively runs the show. Take the University of New Hampshire: back in 2016, a university librarian named Robert Morin left his life’s savings to the school after 50 years of service. Morin lived frugally for that half century and amassed a personal fortune of $4m.
He believed so deeply in the university’s mission that he turned it all over to the school without any restrictions. Talk about earning to give! The university blew Morin’s gift on a new jumbotron for their sports stadium:
https://www.washingtonpost.com/news/morning-mix/wp/2016/09/16/university-to-buy-1-million-football-scoreboard-with-thrifty-librarians-money-outraging-critics/
The people who see universities as inconvenient adjuncts to exploitative sports teams know that there are still rivals within higher ed who think the point of the school is to educate students.
That’s why the universities that arranged to allow sports gambling websites to target the young people in their care did so in secret.
https://www.nytimes.com/2022/11/20/business/caesars-sports-betting-universities-colleges.html?unlocked_article_code=AAAAAAAAAAAAAAAACEIPuonUktbfqYhlSVUZAybfQMMmqBCdnr_EybEnj2XlaTONTixe1KEfDpSc-kHCILdlZsU-xS-aWN5MK_okQ_h2w-BSJAptVwys6NOiqagyHh8U-8i1T39kmNXER6w5-jvnKWDmIe5ymOTn-hvbbzH1XKzbg2lxIVpvvZY2d12t3yMDwKmVFfVnmYUrhYdXDZ54TT8KZiWY7bK_W1glZoLwPlyL4RI2WupZRTnQgdWfjrsCew5TAl7FJ2httSd-sJgPfYNKY9usakIoa8H8gr4OCmd3LYvPBpQ5RILck70Coqf9dPDE9RFVhqXegnp2EK4F
Writing for the New York Times, Anna Betts, Andrew Little, Elizabeth Sander, Alexandra Tremayne-Pengelly and Walt Bogdanich reveal the extraordinary corruption and depravity of college administrators who colluded with sports book companies to bring gambling to campus.
Implicated in the scandal are such top schools as Michigan State, U Colorado Bolder, Louisiana State, Syracuse and Texas Christian Univeristy (mission: “to educate individuals to think and act as ethical leaders and responsible citizens”).
On the casino side, the major player is Caesar’s, which is only fitting — Caesar’s was driven to bankruptcy by private equity who managed to financialize a casino into ruin:
https://www.ft.com/content/a0ed27c6-a2d4-11e7-b797-b61809486fe2
Caesar’s offered universities millions of dollars for the right to directly sports betting to students. The MSU deal, brokered by university officials Paul Schager and Alan Haller, was worth $8.4m. That is to say, Caesar’s was asking the university to help it drain at least $8.4m from students’ bank accounts in order to turn a profit.
Louisiana State U did a similar deal with Caesar’s, and then embarked on a direct marketing campaign to sell sports gambling to students who were too young to legally place a bet.
LSU says this was a mistake. Cody Worsham, a university official who holds two offices — associate athletic director and chief brand officer (!!) — said that Caesar’s and LSU “share a commitment to responsible, age-appropriate marketing.”
Meanwhile, U Colorado Boulder struck a deal where it earned a $30 bounty every time a student went from non-gambler to gambler — in other words, Boulder didn’t make money by advertising gambling to students — it made money only if its students started gambling.
These student gambling programs are designed to keep children betting even if they lose money, with teaser offers that refund some losses if students keep placing bets.
This is obviously unsavory stuff. That’s why the architects of these programs went to enormous lengths to keep it secret. The state schools involved funneled their deals through private marketing agencies that were shielded from FOIA requests, specifically to prevent the public from learning how public universities were conducting their affairs.
As MSU executive associate athletic director Paul Schager put it: “With the multimedia rights holder, public institutions like Michigan State no longer have to disclose all those sponsorship deals. This helps with the sponsors being able to spend what they feel is appropriate without having the public or employees or stockholders question that investment.”
The deals themselves are far-reaching. As part of MSU’s Caesar’s deal, tailgate parties before big games would be “Caesarized,” with the casino providing ad-copy for the live announcers to read to attendees. As a figleaf, $25,000 of the millions that MSU received from Caesar’s was earmarked for gambling addiction education.
The deals weren’t just kept secret from the public — they were also hidden from top university oversight. At UC Bolder, the Board of Regents was informed of the deal mere hours before it was announced to the public.
These deals have only been running for a couple months and it’s too soon to chart the long-term harms they’ll create in the student body. But, the Times* notes, there is an one harm that surfaced almost immediately: student athletes are now subject to vicious abuse by their fellow students, who lose money they can’t afford when their peers lose a game.
[Image ID: A gaudy casino floor. In the foreground is a figure in college graduation robes giving a double thumbs-up. His head is a grinning skull with a mortarboard.]
665 notes
·
View notes
Text
COVID is airborne. Airborne transmission is different from droplets, which are large particles containing the virus, expelled when you speak, cough, sneeze, etc. Droplets are heavy enough that they will eventually drop to the ground or nearby surfaces, meaning it’s relatively easy to contain: any physical barrier — like a cloth mask or plexiglass — will block these droplets before they can reach another person. “Social distancing” is a concept that applies to droplet transmission, under the presumption that the virus-containing droplets will fall to the ground before reaching someone 6 feet away. Sanitizing surfaces kills any viral droplets that have landed on them before someone can touch them and then touch their orifices.
However, COVID is not confined to droplets. We have known for years that it can spread through aerosol as papers published in the New England Journal of Medicine, Emerging Infectious Diseases, and Risk Analysis demonstrate going back to 2020. Aerosol is composed of much smaller particles that bounce around between air particles, and can stay suspended and infectious in the air. Picture someone smoking: the behavior of the smoke is much more akin to the behavior of viral aerosols. Can you still smell the smoke behind a plexiglass shield? How about if you’re six feet apart? In a crowded, enclosed space, how many people would breathe in the smoke of one smoker? Measures designed to protect against droplets aren’t exactly pointless against COVID, since it also spreads via droplets. But just because you’re not spewing COVID-laden spittle in someone’s face does not mean you’re keeping your germs to yourself.
43 notes
·
View notes
Last Seen Blogs

maxiao2019
無標題

midfandom
immortal twat

gh0stofb0nes
Untitled

randoscottbobchloe61
Music is my happy place

freyaishtar
Normal is Overrated